
Abstract
Objective:
Sentinel lymph-node biopsy (SLNB) is now as alternative to pelvic and para-aortic lymph-node dissection (PPALND) for managing endometrial cancers. These data have been largely published from high-volume specialized institutions, but complete PPALND is still performed by many surgeons at smaller nonspecialized centers. The aim of this research was to demonstrate that SLNB is feasible, reproducible, and sensitive without affecting cancer-specific outcomes when implemented at nonspecialized centers.
Materials and Methods:
Cases of patients with clinical stage-I endometrial cancer were retrospectively reviewed from September 2016 through February 2020. Endometrioid, uterine papillary serous (UPSC), malignant mixed-mesodermal tumor (MMMT), and clear-cell (CC) histologies were included. All patients had undergone either robot-assisted or laparoscopic hysterectomies with SLNB. Indocyanine green was injected into the cervix bilaterally. Per the algorithm, patients with suboptimal lymph-node mapping or nodes suspicious for metastasis underwent a side-specific pelvic lymph-node dissection (LND). Para-aortic LND was performed at the discretion of the surgeon. In addition to SLNB, PPALND was performed for patients with MMMT, UPSC, or CC. Sentinel lymph nodes (SLNs) were evaluated using ultrastaging protocols with serial sectioning and cytokeratin staining. The medical records were queried for clinical or radiographic evidence of recurrences.
Results:
A total of 92 cases were included: 69 stage IA; 12 stage IB; 3 stage II; and 8 stage III (2 IIIA, 2 IIIC1, 4 IIIC2). The majority of cancers were endometrioid (73%), followed by UPSC (15.0%), MMMT (5.0%), and CC (4%). At least 1 SLN was detected in 95.4% of cases. The rate of bilateral SLN detection was 74.3% and improved over time from 2017 to 2019: 70% (2017); 74.4% (2018); and 80% (2019). Twenty patients underwent PPALND. Non-SLNs were positive in 3 patients, all with high-risk histologies. No other patients had false–negative SLNs. No recurrences occurred in this cohort with a median follow-up of 22 months.
Conclusions:
SLNB is a sensitive and specific method for assessing lymph-node involvement in patients with clinical stage-I endometrial cancers. These results are comparable to the rates reported in the literature and shows that, in nonspecialized centers, this approach is safe and reproducible without affecting cancer-specific outcomes. (J GYNECOL SURG 38:305)
Introduction
Endometrial cancer is the most-common gynecologic malignancy in the United States; 65,620 new cases were estimated and 12,000 deaths were predicted for the year 2020. 1 Most women present with early stage disease, and surgical resection of the primary tumor, along with comprehensive lymph-node dissection (LND) has conventionally been the mainstay of treatment.
Historically, complete pelvic and para-aortic lymphadenectomy has been performed as part of surgical staging and to guide subsequent adjuvant therapies for women diagnosed with uterine cancer. Complete pelvic lymphadenectomy is not without surgical morbidity, and is associated with a 20%–47% risk of lymphedema in patients with endometrial cancer, as well as prolonged operative time and increased risks of neurologic or vascular injuries. 2
Sentinel lymph-node mapping has emerged as an alternate approach to comprehensive staging that enables surgeons to identify lymph-node metastasis while reducing the surgical morbidity associated with full pelvic and para-aortic lymphadenectomy. 2 Sentinel lymph-node (SLN) mapping was initially described in cases of breast cancer and cutaneous melanoma 3 and has been incorporated more recently into the staging of vulvar, cervical, and endometrial cancers.
Initial studies of endometrial cancers reported the use of blue dyes and radioactive colloid technetium-99, while more-recent protocols have utilized indocyanine green, as near-infrared camera capabilities become more widely available. The majority of these studies were performed at cancer specialty centers while many surgeons in nonspecialty centers continued to perform comprehensive LNDs.
A survey performed by the American Society of Clinical Oncology (ASCO) several years ago reported that only 28.6% of respondents were performing SLN mapping routinely for endometrial cancers. 4 When performing SLN mapping, technique and expertise are critical and a learning curve of ∼30 cases has been described previously. 2
The objective of the current study was to demonstrate that SLNB is feasible, reproducible, and sensitive when implemented at nonspecialized centers, without affecting cancer-specific outcomes.
Materials and Methods
After institutional board review approval, cases of all patients with clinical stage-I endometrial cancer who underwent either robot-assisted or laparoscopic total hysterectomy at Lenox Hill Hospital, New York, NY, USA, were retrospectively selected from 2016 to 2020. Clinical stage-I endometrial cancer was determined by preoperative physical examination and imaging. The decisions to perform surgery robotically verses laparoscopically was based on surgeon preferences. Patients with endometrioid, uterine papillary serous (UPSC), malignant mixed-mesodermal tumor (MMMT), and clear-cell (CC) histologic subtypes were included.
For each procedure, indocyanine green had been reconstituted per the manufacturer's directions and injected into the patient's cervix bilaterally at 3 o'clock and 9 o'clock positions, both superficially (submucosaly) and deeply (1 cm into the stroma). Sentinel nodes were identified using near-infrared technology.
Patients with suboptimal lymph-node mapping or nodes suspicious for metastasis during surgical evaluation underwent side-specific pelvic LND. Para-aortic LND was performed at the discretion of the surgeon.
In addition to SLNB, complete pelvic and para-aortic LND (PPALND) was performed for patients with the following high-risk histologic subtypes: UPSC; CC; and MMMT. SLNs were then evaluated by gynecologic pathologists using ultrastaging protocols, including serial sectioning and cytokeratin staining.
The medical records were checked for clinical or radiographic evidence of recurrences; the median follow-up was 22 months for this cohort.
The primary objective of this study was to evaluate the accuracy and sensitivity of SLN mapping at our university-affiliated community-based institution. In addition, rates of SLN detection were evaluated over 3 years to chart potential improvements over time that correlated to surgeon experience.
Descriptive statistics—such as frequency distribution, mean, median, interquartile range, and minimum and maximum—were calculated for relevant variables. To compare successful mapping rates at our institution to those in the literature a 1-sample test of proportion was performed.
χ
2
and Fisher's exact test were performed to determine if successful mapping rates among patients was related to patient-specific factors, such as body mass index (BMI), as well as pathologic factors, such as the presence of uterine leiomyoma, adenomyosis, lymphovascular-space invasion (LVSI), and tumor depth of invasion (DOI) <50% versus
Results
Between September 2016 and February 2020, 92 patients with endometrial cancer underwent total hysterectomy, bilateral salpingo-oophorectomy, and lymphatic mapping. The surgeries were all performed at Lenox Hill Hospital by 2 gynecologic oncology surgeons. Demographic and clinicopathologic characteristics of the study population are summarized in Table 1. The median age of the patients was 62 (range: 28–83), and the median BMI was 30.85 kg/m2 (range: 19.9–53.4). Surgical approach was at the discretion of the provider. Of the 92 cases evaluated, 70 were performed with robotic assistance (76%), while 22 procedures were completed laparoscopically (24%).
Demographic Characteristics
BMI, body mass index; CC, clear-cell; MMT; malignant mixed-mesodermal tumor FIGO, International Federation of Gynaecology and Obstetrics.
The distribution of histologic types was endometrioid (73%), followed by UPSC (15.0%), MMMT (5.0%), and CC (4%). Stage-I disease was confirmed in the majority of patients; 69 were stage IA (71%) and 12 were stage IB (14%). A total of 8 patients had stage-III disease, of which 6 were stage III based on node positivity: 2 IIIA; 2 IIIC1; and 4 IIIC2. Of the stage-III patients, 2 patients had endometrioid histology and 6 had UPSC.
One unilateral SLN was detected in 88 (95.4%) patients. The overall rate of bilateral SLND was 75.3%. Over time, the bilateral SLN detection rate improved from 70.5% in 2017 to 80% in 2020 (Fig. 1). Twenty patients underwent PPALND (16 for high-grade histology, 3 for failed mapping, and 1 secondary to a clinically suspicious lymph node). Per the algorithm, intraoperative evaluations of uterine specimen were performed for 12 patients with failed SLN mapping and findings were consistent with low-risk for lymph-node metastasis and, therefore, PPALND was not performed.
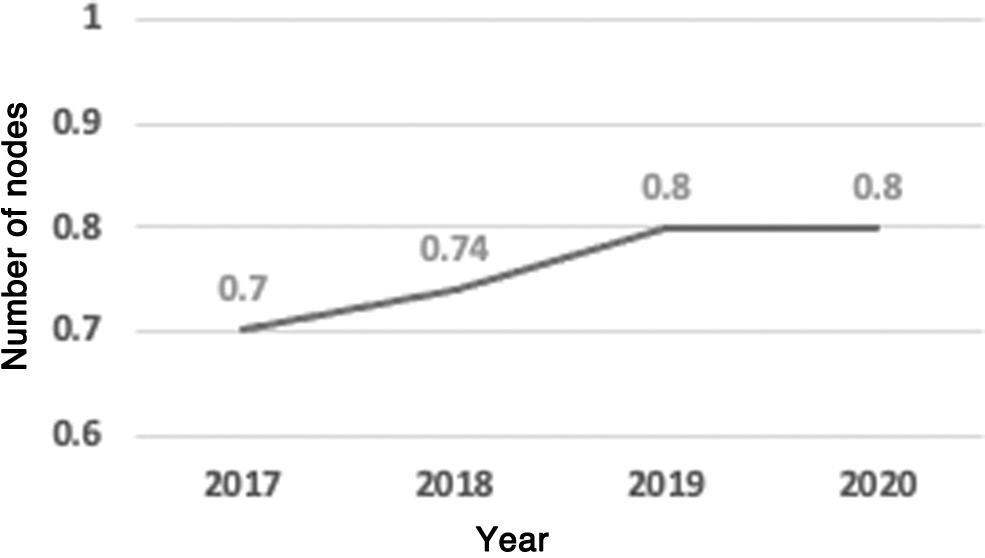
Bilateral sentinel lymph node detection rates by year.
SLN mapping rates were analyzed among 5 subgroups based on additional patient-specific and pathologic factors: (1) DOI; (2) presence of LVSI; (3) uterine leiomyoma; (4) uterine adenomyosis; (5) and BMI. None of these factors were significantly associated with rate of successful bilateral SLN mapping (DOI p = 0.1; LVSI p = 0.22; uterine leiomyoma p = 1.0; adenomyosis p = 0.29; and BMI p = 0.91).
Three patients had positive nodes other than the surgically identified SLNs. All 3 patients had serous histology. Two of them underwent planned PPALND for known high-risk histology. The third patient had a suspicious enlarged lymph node seen on preoperative imaging; this lymph node was positive for disease at the time of the surgery. Of note, the preoperative diagnosis for this patient was endometrioid adenocarcinoma and the UPSC component was diagnosed on final pathology.
In a comparison to the selected meta-analysis, 5 both bilateral (75.3% versus 61%; p = 0.0001) and unilateral (95.4% versus 78%; p = 0.0111) SLN mapping rates were significantly higher in the current study's cohort.
Discussion
The results of the current study support that SLNB is feasible, reproducible, and sensitive without affecting cancer-specific outcomes when implemented at nonspecialized centers for type-I endometrial cancer.
SLN mapping alone identified at least 1 lymph node accurately in 95.4% of patients with endometrial cancer in our cohort and the overall bilateral SLN mapping rate reached 80% by the end of the study. These rates are on a par with—if not better than—those reported in the literature. Two meta-analyses, 1 performed by Bodurtha Smith et al. 2 and 1 performed by Kang et al., 5 on endometrial-cancer SLN mapping reported unilateral pooled average detection rates of 78%–81% with a bilateral detection rate of 61%.
Although single institution data are difficult to compare to a meta-analysis, this finding supports that the current study's results were comparable to those at other institutions.
Guidelines extrapolated from studies of breast cancer, melanoma, and vulvar cancer suggest that surgeons need to complete 30 cases in order to achieve competency for reliable detection of SLNs in endometrial-cancer staging procedures. 6 Following recommendations from the ASCO on acceptable proficiency for breast-cancer SLN mapping, the metastatic detection rate should be >80%–90% and the false–negative rate should be <5%. 4
In the current study's cohort, the rates of successful SLN mapping improved over the course of the study. This reflects increased provider detection rates over time with improvement of surgical skill.
With regard to false–negative rates, the current study's data performed well with disease detected in only 3 non-SLNs. All 3 patients had serous components to their tumors, and received adjuvant treatment with chemotherapy and radiation. To date, there have been no disease recurrences in this cohort over a median follow-up of 22 months.
Prior to introducing SLNB as an alternative to full pelvic and para-aortic lymphadenectomy, it was important to first demonstrate that lymphadenectomy does not provide an independent therapeutic benefit. The CONSORT [CONsolidated Standards Of Reporting Trials] and ASTEC trials [A Study on the Treatment of Endometrial Cancer], are often considered together and were fundamental in demonstrating that complete lymphadenectomy is not associated with an overall survival benefit in women with endometrial cancer.7,8 Despite this evidence, many practicing gynecologic oncologists continue to perform full LNDs in surgical staging for endometrial cancer. In 2015, only 28.6% of gynecologic oncologists participating in a survey conducted by the ASCO performed SLN mapping for patients who had endometrial cancer, thus, continuing to reflect a wide range of provider-specific practices. 4
More-recent studies generated by large cancer specialty centers reported overall recurrence rates as low as 1.4%–9.4% in SLN cohorts with stage-I endometrial cancer.7,9 In 1 such study, 1-year disease-free recurrence rates among patients who underwent SLN mapping were similar to the rates of patients who underwent complete lymphadenectomy, with a 9.4% recurrence rate in an SLN group and a 14% recurrence in a complete LND cohort.
Additionally, SLN cohorts had improved pelvic side-wall recurrence-free survival, compared to patients undergoing complete pelvic LND. 10 The current study's data also showed that there were no recurrences in the cohort.
Taken together, these data support the growing consensus that SLN mapping can be implemented as an appropriate balance between nodal assessment and the morbidities associated with complete pelvic and para-aortic lymphadenectomy, while increasing the detection rate of clinically significant metastatic disease.
The current study had several limitations. Given that the clinical impact of SLN mapping for high-risk endometrial histologies, such as UPSC, CC and MMMT, have not been studied robustly, it is difficult to assess the significance of the 3 documented false–negative SLNs in patients with UPSC histology in the current study's cohort. It has been shown previously that elimination of lymphadenectomy in cases of high-risk histology may be associated with more risk of treatment failure.9,11 Given the relatively small sample size, the data in the current study are insufficient to comment on safety or feasibility of SLNB in high-risk endometrial histologic subtypes; the current authors perform complete lymphadenectomy after SLN mapping for these cases.
Additionally, although no associations were discovered between SLN mapping rates and BMI, presence of leiomyoma, adenomyosis, and DOI, it is possible that associations would be seen in a larger cohort. 12 Overall, the power of this study was limited by the sample size of patients and the retrospective nature of the study design. There were no recurrences in these patients up to the end point follow-up, but long-term follow-up will provide additional information with regard to disease recurrences.
Conclusions
The current study's data indicated that high SLN detection rates can be achieved by gynecologic oncologists who are treating women with endometrial cancer at nonspecialty surgical institutions. Optimization of provider technique and expertise is critical to meet defined standards of SLN-detection accuracy. Once individual surgeons demonstrate proficiency in SLN mapping and detection, based on the current study's data, it would seem reasonable to recommend SLN mapping and biopsy as standard of care for treatment and management of uterine endometrial cancer across all institutions.
Footnotes
Authors' Contributions
Dr. Pereira conceptualized this project. She collected the data and, together with Drs. Gadomski and Leung, analyzed it. Dr. Werner also wrote the article and abstract, Drs. Pereira and Villella edited the abstract and article, and Dr. Gadomski edited the article.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No external funding was provided for this work.