
Abstract
Correction of apical descent is an essential component of a durable prolapse surgery and can be achieved by multiple different techniques and surgical approaches. Laparoscopic prolapse surgery produces excellent outcomes and lower costs, compared to robotic surgery, without compromising success and remains a valuable surgical approach to prolapse repair. This review summarizes the evidence for conventional laparoscopic apical prolapse repair, compared to alternative surgical approaches, and provides recommended techniques with tips and tricks to optimize this approach. (J GYNECOL SURG 39:19)
Introduction
Nearly half of the female population is affected by pelvic organ prolapse (POP), and surgical intervention is performed 11%–19% of the time. 1 Correction of apical descent is an essential component of a durable prolapse surgery and can be performed vaginally or abdominally. 2
The earliest apical procedure performed abdominally was described in the late 1950s and it secured the vagina directly to the sacrum. 3 The use of a graft to bridge the vagina to the sacrum, in order to decrease tension on the vagina, was introduced in 1962. 4 Even in studies early in the 2000s, abdominal sacrocolpopexy (ASC) produced successful long-term outcomes ranging from 58% to 100%. 5 However, the morbidity associated with an open procedure spurred surgeons to innovate minimally invasive techniques. The first case series of laparoscopic sacrocolpopexies was described by Nezhat et al. in 1994. 6
Although comparative studies have shown similar success for both minimally invasive sacrocolpopexy and conventional laparotomy, 7 the use of laparoscopic prolapse repair has not been widely adopted in practice. One reason is that the implementation of robotic-assisted surgery overshadowed conventional laparoscopy by advertising 3-dimensional visualization, dexterity, and ergonomics. A second reason is that achieving competency and proficiency in laparoscopic surgical techniques requires a longer learning curve. However, laparoscopic prolapse surgery produces excellent outcomes and lower costs, without compromising success, and remains a valuable surgical approach for prolapse repair. 8 This review summarizes the evidence for conventional laparoscopic prolapse repair, compared to alternative surgical approaches, and provides recommended techniques for performing a laparoscopic prolapse repair successfully.
Evidence Based Comparisons Between Approaches
Laparoscopic sacrocolpopexy compared to ASC
Laparoscopic sacrocolpopexy (LSC) and ASC have comparable subjective cure rates of 80% and 90%, respectively, at 1 year in prospective cohort studies. 9 Two randomized controlled trials showed no significant difference in anatomical outcomes at 12 months between ASC and LSC (mean difference [MD]: 0.06 cm; 95% confidence interval [CI]: −0.49 to 0.61). 10 There was also no difference in reoperation for recurrent prolapse between the 2 approaches (odds ratio [OR]: 1.52; 95% CI: 0.7–3.28). 11 Compared to ASC, LSC was associated with a shorter hospital stay (2 days [interquartile range (IQR): 2–3] versus 4 days [IQR: 3–5; p < 0.001]) and less blood loss (median: 86 versus 200 mL), 12 and there was no difference in intraoperative complications, duration of surgery, or mesh exposure.11,12
LSC compared to robotic sacrocolpopexy
Anatomical success using the POP-Q [Pelvic Organ Prolapse Quantification] system at 6 months after surgery was similar between both robotic sacrocolpopexy (RSC) and LSC approaches. 7 There was also no difference in reoperation for recurrent prolapse, indicating equivalent treatment success. 7 A recent systematic review reported a longer operative time for RSC than LSC (MD: 29.53 minutes; 95% CI: 12.88–46.18 minutes). 7 There was no significant difference between RSC and LSC groups in intraoperative complications of bladder, bowel, ureteral, or vascular injuries. 7 Estimated blood loss was lower in the RSC group, compared to the LSC group (MD: −86.52 mL; 95% CI: −130.26 to −42.79 mL). 7 While 1 systematic review suggested a higher conversion rate with LSC, compared to RSC (2.97% versus 1.04%), 7 other studies reported no significant difference, with overall conversion rates of <5%. 13
A similar incidence of postoperative complications was noted between RSC and LSC (16.39% and 20.3%; OR: 0.9; 95% CI: 0.57–1.41; p = 0.63). 7 Higher postoperative pain scores and analgesic requirements occurred with RSC, compared to LSC. 8 There was no significant difference between the 2 surgical approaches in terms of mesh exposure. 8 In 1 study, RSC incurred a $1936 higher cost, compared to LSC, even when adjusting for confounding operating-room costs. 8 The question remains if there is a benefit to balance the higher cost of robotic surgery for the sacrocolpopexy procedure.
Laparoscopic uterosacral ligament suspension, compared to vaginal uterosacral ligament suspension
Currently, the available data on laparoscopic uterosacral ligament suspension (USLS; L-USLS) is limited to retrospective studies. Rardin et al. reported a trend toward lower apical failure rates (0% versus 6.3%; p = 0.22) and recurrent symptomatic vault prolapse requiring intervention (0% versus 10%; p = 0.28) with L-USLS compared to vaginal USLS (V-USLS). 14 Other studies have not shown a significant difference in recurrences. 15 Postoperative anatomical outcomes revealed a longer total vaginal length (8.3 ± 1.1 cm versus 7.4 ± 1.2 cm; p < 0.001) 15 and higher C point (−7.0 versus −5.9 cm; p = 0.04) in L-USLS compared to V-USLS. 14 In another study, there was no statistical difference in operative times, blood losses, or transfusions. 16 A higher incidence of ureteral obstruction was seen in V-USLS, compared to L-USLS, with rates ranging between 4% and 6%; p = 0.32.14,16 As the above studies were limited by small sample sizes, larger robustly designed randomized trials are needed to assess the role of L-USLS properly. However, observed trends indicate that L-USLS is a feasible and safe option for treating apical prolapse.
Minimally invasive sacrocolpopexy versus native-tissue repair
Comparative literature on vaginal apical suspension procedures and LSC is limited to retrospective studies. Chen et al. compared LSC/laparoscopic sacrohysteropexy (LSH) with vaginal sacrospinous ligament suspension (SSLS) showing an overall success rate (LSC/LSH: 90.3% versus SSLS: 85.1%; p = 0.257) and recurrent anterior/posterior prolapse rates (LSC/LSH: 10.6% versus SSLS: 16%; p = 0.256) being similar between the 2 groups. 17 After a 2 year follow-up, subjective improvement did not differ between groups (LSC/LSH: 92.9% versus SSLS: 87.2%). 17 Moreover, a smaller retrospective cohort study showed longer operative times with LSC compared to sacrospinous ligament fixation, iliococcygeus fixation, and abdominal sacrocolpopexy with 179 minutes, 122.8 minutes, 107.1 minutes, and 117.3 minutes (p < 0.01), respectively. 18 Similarly, an observational study noted longer operative times with a minimally invasive sacrocolpopexy compared to SSLS and USLS (175 versus 96 and 120 minutes, respectively; p < 0.001). 19
Compared to nonmesh vaginal surgeries for vaginal vault prolapse, a retrospective analysis of a nationwide database revealed a lower rate of 30-day minor complications (3.9% versus 5.6%; p = 0.004), lower urinary tract infection (UTI) rates (3.3% versus 4.8%; p = 0.004), and fewer prolonged admissions (5.2% versus 7.9%; p < 0.0001) with minimally invasive sacrocolpopexy. 20 No association between minimally invasive sacrocolpopexy and risks for 30-day complications, hospitalizations, readmissions, or reoperations was seen. 20
Furthermore, Anand et al. completed a retrospective study that showed a higher rate of UTIs with the Mayo–McCall culdoplasty (MMC) compared to RSC and ASC (MMC: 22.1% versus ASC: 13.2%; p = 0.02; MMC: 27.9% versus RSC: 7%; p < 0.001). 21 The RSC group had more complications requiring procedural interventions, compared with the MMC group (9.4% versus 1.1%; p = 0.008). 21 In addition, wound complications were seen more frequently in the ASC and RSC groups, compared to the MMC group, with granulation tissue accounting for 92% of wound complications in the MMC group. 21 Overall, a similar perioperative safety profile was noted between transvaginal native tissue repair and the minimally invasive sacrocolpopexy procedure. 19 See Table 1.
Alternative Surgical Approaches, Compared to Laparoscopic Approach to Pelvic Organ Prolapse Surgery
ASC, abdominal sacrocolpopexy; LSC, laparoscopic sacrocolpopexy; GI, gastrointestinal; RSC, robotic sacrocolpopexy; OR, operating room; V-USLS, vaginal uterosacral ligament suspension; L-USLS, laparoscopic uterosacral ligament suspension; POP, pelvic organ prolapse; TVL, total vaginal length; UTI, urinary-tract infection.
Laparoscopic Surgical Technique
Uterosacral ligament suspension
L-USLS can be performed at the time of hysterectomy for nonprolapse indications to prevent vault prolapse or L-USLS can be performed as a high USLS to treat apical prolapse, with or without hysterectomy.
L-USLS for a nonprolapse indication is performed at the time of vaginal cuff closure. While closing the corners of the cuff, the suture needle is placed through the uterosacral ligament (USL) 2–3 cm proximal to the cuff. Instead of incorporating the USL into the cuff closure, a separate suture can be used similarly to secure the USL to the cuff. This ensures good purchase of the ligament to re-support the vaginal cuff. A key concept is to incorporate the full thickness of the vagina to secure the apex.
High-USLS to treat apical prolapse aims to place the most proximal suture through the USL at the level of the ischial spine. Various techniques have been described in the literature, but the following sections summarize the current authors' technique, which is similar for colpopexy and hysteropexy.
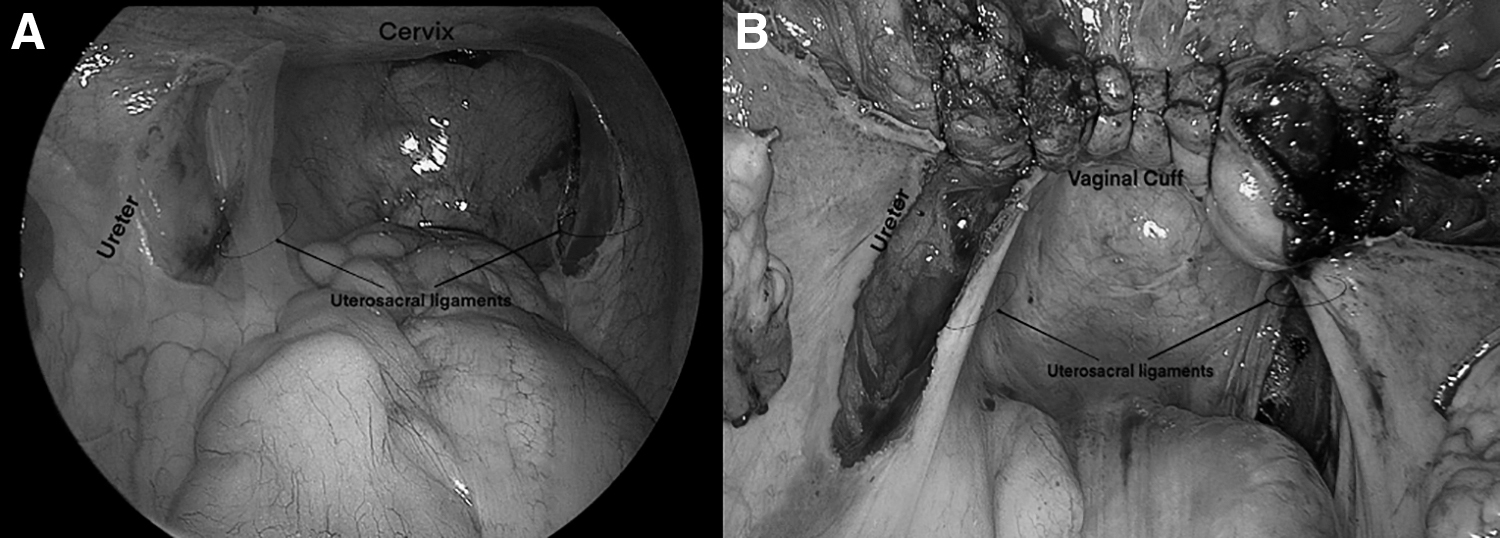
(1) Peritoneal releasing incisions. Given that it is easier to identify the USL before the uterus is removed, the current authors recommend performing releasing incisions on the peritoneum along the lateral border of the USL prior to starting the hysterectomy (Fig. 1). With a manipulator in the uterus, the uterus is anteflexed to place tension on the USL. The ureter lateral to the ligament is Identified. Then, one should identify where the USL arcs posteriorly to the level of the ischial spine. A releasing incision is made in the peritoneum at the level of the ischial spine just lateral to the ligament for at least 3 cm in length along the ligament to ensure that the suture goes into the ligament—not just into a peritoneal fold. This peritoneal incision can be continued along the entire length of the ligament toward the vaginal cuff to allow the ureter to retract laterally and to decrease the risk of placing medial traction on the ureters with the suspension sutures. These releasing incisions are performed bilaterally. This dissection also enables visualization of the right and left inferior hypogastric plexus (IHP) and care can be taken to avoid incorporating these into the suture.
(2) Hysterectomy and cuff closure. If the uterus is removed, suspension sutures can be placed either before or after cuff closure. One benefit to closing the vaginal cuff first is the ability to use a vaginal probe gently to create tension on the vagina while performing the uterosacral ligament sutures. A benefit to leaving the cuff open until after the ligament sutures are placed is the ability to ensure that the sutures are placed through the full thickness of the posterior and anterior vagina.
(3) Bilateral high USL sutures. An extracorporeal knot-tying technique is used. Two suspension sutures are placed on each USL. The first suture is inserted into the USL at the level of the ischial spine and is then brought through the anterior and posterior vaginal cuff at the corner. The second suture is inserted into the USL 1 cm proximal to the first suture and is brought through the anterior and posterior vaginal cuff medial to the corners. This is performed bilaterally (Fig. 2). If a surgeon is performing a hysteropexy, sutures can be placed at the upper posterior vagina or into the posterior cervix at the level of the internal os. It is helpful to have a vaginal probe direct the upper vagina toward the USL as it is being tied to relieve tension and avoid air-knots or tearing through the tissue.
Sacrocolpopexy
Successful optimization of an LSC requires significant training and setup with a team-based approach. Setup for the procedure is critical, as there is an extensive amount of suturing required. Training the surgical technician for setup is a critical step that should not be overlooked.
Laparoscopic peritoneal incisions.
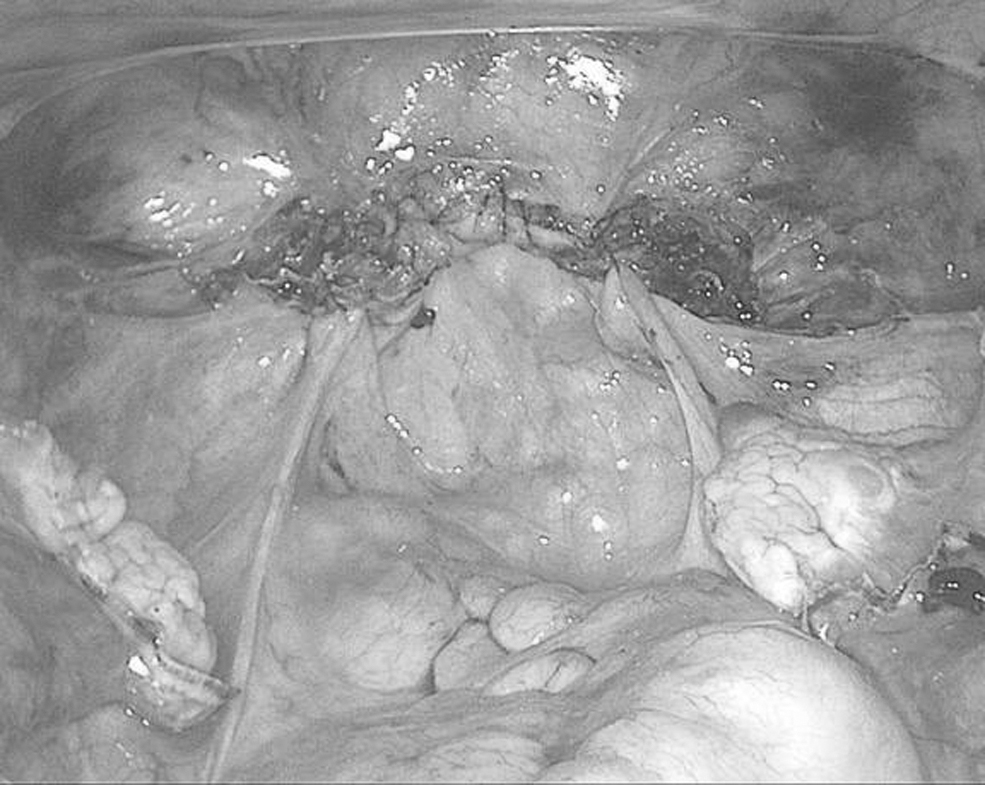
Laparoscopic uterosacral ligament suspension. The first suture is placed into the uterosacral ligament (USL) at the level of the ischial spine and brought through the anterior and posterior vaginal cuff at the corner. The second suture is inserted in the USL 1 cm proximal to the first suture and is brought through the anterior and posterior vaginal cuff medial to the corners. This is performed bilaterally.
(1) Set up. The surgical technician and instrument table should be on the same side as the surgeon who will be performing the extracorporeal knot tying. This enables the instruments to be passed easily without going across the surgical field. A monofilament suture of 36” or longer facilitates extracorporeal knot tying. This is usually passed by the surgeon on the right, to the surgeon on the left, who is performing the suturing. A second setup of suture, knot pusher, and clamp improves surgical efficiency. To improve surgical exposure of the pelvis and sacral promontory, a suture may be used to retract the colon. After the suture is placed through 2–3 epiploic appendages, it is grasped and drawn out of the left lower abdominal wall with a port-site closure needle to retract the colon laterally. The suture is clamped external to the patient's abdomen. Clamping the suture outside the patient's abdomen provides adjustable traction to the colon during the dissection.
(2) Dissection. There is significant variety in dissection techniques. Whether hysterectomy is performed or not, anterior vesicovaginal dissection is necessary and is typically carried down to the distal one-third of the vagina to avoid placing mesh posterior to the trigone of the bladder. Similarly, the rectovaginal space is dissected to the distal one-third posteriorly. Some surgeons advocate sutures in the levator ani 22 ; however, this is not the current authors' standard technique because of concern about causing postoperative myofascial pain.
(3) Mesh placement. Whether a Y-mesh or 2 strips of mesh are utilized, the mesh is attached to the anterior and posterior vaginal walls. A space-occupying probe is placed in the vagina, which produces tension against the vaginal walls. A typical suturing principle teaches the surgeon to enter the tissue plane perpendicularly. However, due to the vaginal probe, this is not possible, and suturing should be parallel to the tissue plane, taking a superficial bite that is sufficient to anchor the mesh in place. An extracorporeal knot-tying technique is used to place 5–6 sutures on each vaginal wall.
(4) Sacral dissection. The dissection of the presacral peritoneum is performed at the level of the sacral promontory and distal. The superior hypogastric plexus (SHP) is most often found to the left of this dissection, and the right branch of the pelvic nerve should be identified to avoid injury. 23 Dissection distal from the level of the promontory enables clearance of the anterior longitudinal ligament at the level of S1–S2, where the mesh attachment should be performed to avoid placing the suture into the L5–S1 disc. A 30° laparoscope enables adequate visualization beyond the promontory.
Nerve-sparing techniques
Restoration of function is the goal of the pelvic-reconstructive surgeon. With this, careful attention should be placed on the neuroanatomy of the pelvic viscera to avoid compromising its function. A clear understanding of the autonomic-nervous supply of the pelvis enables the surgeon to identify these structures and avoid injury, with either transection or entrapment. Nerve-sparing techniques has been described for oncologic procedures such as radical hysterectomy. Outcomes have shown this technique to produce improved bladder function without compromising oncologic outcome. 24 Although urogynecologists typically work to restore function, nerve-sparing techniques in pelvic reconstructive surgery have not been well-described. Data are limited to a few case series of nerve-sparing sacrocolpopexy, wherein outcomes have shown decreased de novo bowel dysfunction when a nerve-sparing approach is applied.25,26
The areas of risk to the autonomic nerves are at the level of the sacral promontory and also at the level of the USL. The SHP is often encountered to the left of the midline of the sacral promontory. During dissection of the presacral space, the right branch of the pelvic nerve should be identified carefully. 23 When performing the peritoneal incision to connect the presacral dissection to the posterior vaginal wall, careful dissection will avoid injury to this nerve and the IHP at the level of the USL. With careful visualization, the mesh attachment for SCP can be performed without injury to the SHP and its branches.
The right pelvic-nerve branches from the SHP and meets the IHP to become the mixed autonomic nerves of the pelvic viscera. The IHP is encountered lateral to the USL and medial to the ureter. (Fig. 3) With careful dissection, this can be lateralized from the USL. A laparoscopic approach to USLS enables this dissection with a peritoneal-releasing incision. Sutures can then be placed while visualizing the IHP and avoiding nerve entrapment.
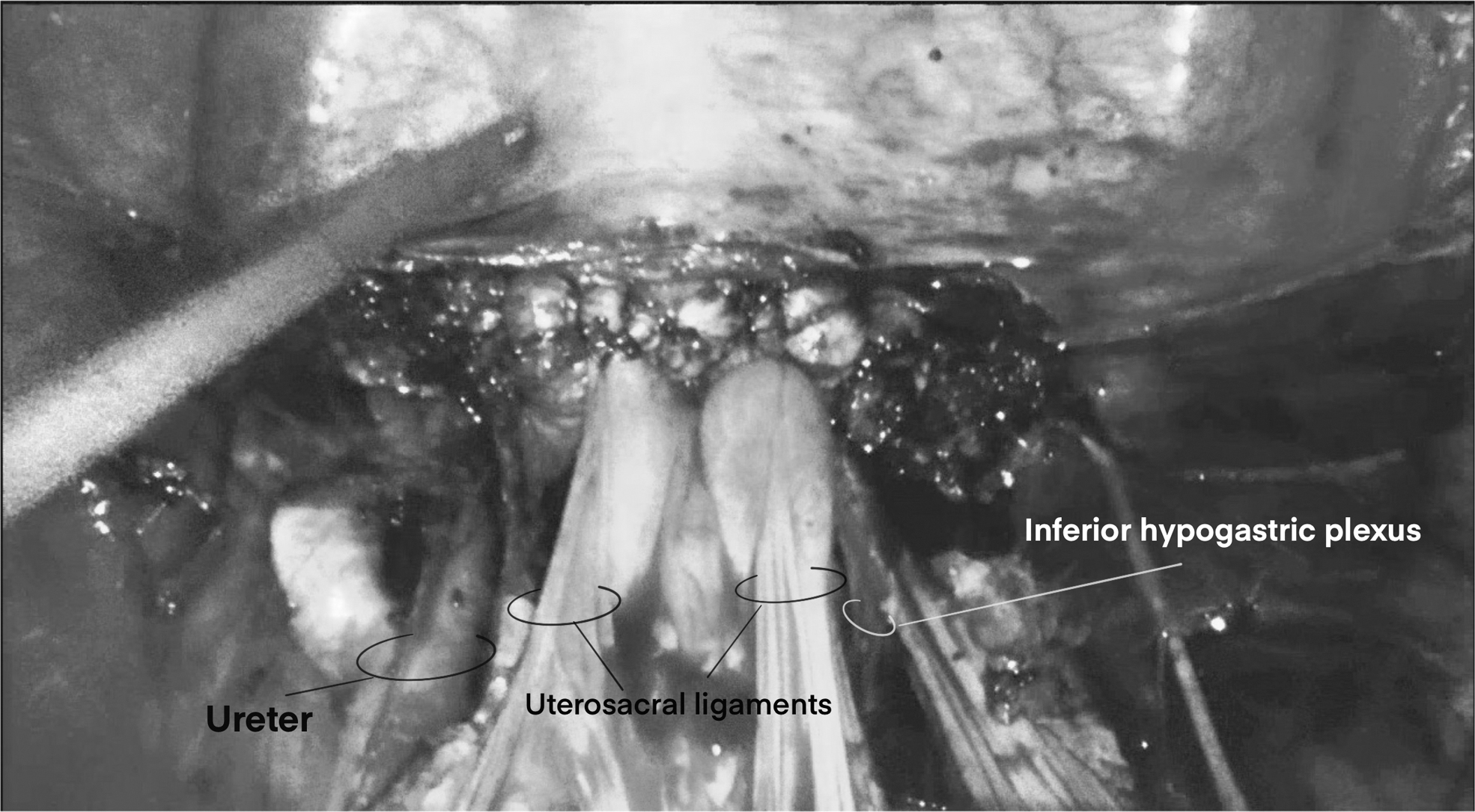
Hypogastric plexus. The inferior hypogastric plexus is encountered lateral to the uterosacral ligament and medial to the ureter.
Magnification during laparoscopy enables the neuroanatomy to be well-visualized, and care should be taken to avoid nerve injury. While further clinical trials are necessary to identify the effects of nerve-sparing techniques on functional outcomes, the pelvic nerves and hypogastric plexus should be recognized as critical structures during pelvic reconstructive surgery.
Conclusions
Although robotic surgery has become a common approach to vaginal-prolapse repair, laparoscopic surgery produces excellent outcomes and lower costs without compromising success and remains a valuable surgical approach for prolapse repair. This article reviewed surgical technique tips to enable successful and efficient laparoscopic prolapse surgery. Given that laparoscopy enables visualization of the pelvic nerves and hypogastric plexus, the current authors encourage using a nerve-sparing technique because of its potential to improve functional outcomes after surgery.
Footnotes
Authors' Contribution
All of the authors were involved with project development, data collection, and article writing and editing
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was received for this work.