
Abstract
Objective:
This research compared laparoscopic hysterectomy (LH) and vaginal hysterectomy (VH) for operative time, complications, postoperative pain, inflammatory response, hospital stay, and costs.
Materials and Methods:
A randomized controlled trial compared LH and VH for 80 patients equally allocated to undergo either for benign pathology (Canadian Task Force Classification I).
Results:
Mean operative time was significantly higher for LH (127.5 ± 25.9 minutes; 95% confidence interval [CI]: 119.2, 135.8) than for VH (104 ± 30.8 minutes; 95% CI: 94.2, 113.9); p = 0.0004. There was no significant difference in median blood loss (LH: 250 mL and VH: 235 mL); p = 0.7983). There was a strong positive correlation between operative time and estimated uterine weight, especially for VH. Adnexal surgery was performed as planned preoperatively in 62.5% of LHs versus 27.5% of VHs; p < 0.0035. Both groups were comparable regarding intra- and postoperative complications (p = 1.0). Median postoperative pain intensity was lower in LH than in VH at 2 hours (51 versus 64.5; p = 0.0038), 6 hours (38.5 versus 46; p = 0.0009), and 24 hours (24.5 versus 36.5; p < 0.0001). Inflammatory response did not differ between the groups, neither as postoperative fever (7.5% of LH versus 2.5% of VH; p = 0.6153) nor as postoperative C-reactive protein rise (median: 57.4 mg/L for LH; 41.6 mg/L for VH; p = 0.1489). There was no difference in hospital stay (LH median: 35.5 hours; VH median: 30 hours; p = 0.6991). Costs for LH were higher (LH median: 5525 Egyptian pounds (EGPs), 335 US dollars (USD); VH median: 3400 EGPs, 207 USD; p < 0.0001).
Conclusions:
LH has longer operative time, yet better postoperative pain profile, than VH. However, cost considerations make LH fall behind VH as a primary choice for benign hysterectomy, especially in low-resource settings. (J GYNECOL SURG 38:400)
Introduction
Hysterectomy is one of the most frequently performed operations in gynecologic practice. Selection of abdominal hysterectomy (AH), vaginal hysterectomy (VH), or laparoscopic hysterectomy (LH) routes for benign pathology is governed by many factors, including the condition and preference of the informed patient, training and skill of the surgeon, and equipment at the facility. 1
In the United States over the last 20 years, the overall number of benign hysterectomies dropped substantially, and the distribution of routes has also changed. This is shown by studies examining data from the Nationwide Inpatient Sample (a 20% stratified random sample of discharges from all community hospitals) in 20032 and 2012, 3 wherein the proportion of LHs had increased (12%–19%), reflected in a decline in both AH (66%–51%) and VH (22%–16%). This trend continued in later samples that were studied more recently, 4 with LH being more popular than VH, and AH still being the most common. VH and LH are considered “minimally invasive” for not requiring a large abdominal incision, 5 and typically are associated with shorter hospitalization and quicker return to normal activities, compared with AH. Thus, minimally invasive approaches should be adopted, whenever applicable, based on their well-documented advantages over laparotomy. 6
A paucity of Egyptian studies compared the outcomes of LH and VH. The aim of this study was to compare the 2 approaches in Ain Shams University Maternity Hospital, in Cairo, one of Egypt's leading tertiary centers in terms of public medical service. The main outcome was to evaluate the difference in operative time; secondary outcomes included complications, postoperative pain, inflammatory response, hospital stay, and costs in a low-resource setting.
Materials and Methods
From March 2019 to February 2020, women admitted to the General Gynecology Outpatient Clinic at Ain Shams University Maternity Hospital to undergo hysterectomy for benign indications were invited to a randomized trial to compare LH and VH, with a 1:1 allocation ratio (Canadian Task Force Classification I). Exclusion criteria were women with more than 2 previous cesarean deliveries, adnexal pathology, pelvic organ prolapse requiring additional procedures (uterine procidentia or enterocele), obesity (body mass index [BMI] ≥30 kg/m2), cardiopulmonary disease precluding laparoscopic surgery, and large uteri making VH difficult (clinically >16-week size). Preoperative evaluation for eligible women included detailed history-taking; thorough general, abdominal and vaginal examinations; preoperative laboratory tests; and transvaginal scan (TVS), with emphasis on the following uterine dimensions: longitudinal (including the cervix); transverse; and anteroposterior. An ellipsoid formula was used to estimate uterine volume. This formula is simplified as:
with the density of uterine tissue being ∼1 g/cm3. 7 Hence, the value of estimated volume in cm3 was taken for the estimated weight in g.
Recruited women provided written informed consent to participate in the study. Premenopausal women were scheduled for total hysterectomy with bilateral opportunistic salpingectomy. Menopausal women were scheduled for bilateral salpingo-oophorectomy (BSO) to avoid subsequent surgery for ovarian neoplasia, which tends to present in advanced stages (with consequent morbidity, low survival rates, and poor quality of life). With no adnexal pathology in any of the participants, there would be no additional risk in case of an unperformed adnexectomy.
The surgical team for any operation included an experienced consultant and an assistant who was well-acquainted with the operative steps. LH was type IV-E according to the American Association of Gynecological Laparoscopists (AAGL) classification, 8 in which the entire uterus is detached laparoscopically. LigaSuretm (Covidien, Minneapolis, MN, USA) for coagulation and division of tissues and pedicles, and a Mangeshikar uterine manipulator (Karl Storz, Tuttlingen, Germany) were used. The vaginal cuff was closed vaginally (due to lack of instruments needed for laparoscopic suturing), and the abdomen was reexamined laparoscopically to visualize the suture line. VH followed the Heaney technique. 9
Prior to study initiation, the protocol was approved by the Research Ethics Committee, Faculty of Medicine, of Ain Shams University (FWA 000017585), approval number: FMASU MD64/2019; and was registered in ClinicalTrials.gov, ID: NCT03692832.
For each patient, anamnestic data were recorded, including age, parity, previous surgery, body mass index, preoperative hemoglobin (Hb), C-reactive protein (CRP), and the indication for hysterectomy. Intraoperative data included duration of surgery, blood loss, adnexal surgery performed intraoperatively (compared to preoperatively scheduled), and complications. Postoperative data included febrile episodes (temperature >38°C), next-day Hb and CRP, and length of hospital stay. A visual analogue scale score for pain intensity was used to evaluate pain at 2-, 6- and 24-hours after surgery. All patients received general endotracheal anesthesia, and intravenous antibiotic prophylaxis (2 g of cefoxitin, with induction according to the hospital's protocol).
The primary outcome of the trial was the operative time, from introduction of the first laparoscopy port or vaginal incision, till suturing the vaginal vault. Secondary outcome measures included blood loss and need for blood transfusion; feasibility of vaginal opportunistic salpingectomy or salpingo-oophorectomy, compared to laparoscopic approach; complications; postoperative pain; inflammatory response to surgery both clinical (postoperative fever) and laboratory (CRP rise 24 hours postoperatively), length of hospital stay, and health care costs.
The sample size was calculated using Stata Statistical Software: Release 13 (StataCorp, College Station, TX, USA), setting the α error at 5% and the study power at 80%. A previous study by Candiani et al. 10 showed mean operative times were: for LH: 99.3 ± 25.4 minutes; and for VH: 82 ± 29.6 minutes. Calculating the sample size according to these values, 40 patients were required in each arm of the study. Participants were given the next available number via a computer-generated randomization plan. Sequentially numbered, opaque, sealed envelopes enclosing treatment allocation were opened after enrollment for administrative reasons (anesthetic consultations and preparation of instrument sets).
Excel 2019 (Microsoft Corporation, Redmond, WA, USA) and MedCalc Statistical Software version 14.8.1 (MedCalc Software, Ostend, Belgium) were used for data presentation and statistical analysis. Normally distributed numerical data were summarized by mean and standard deviation, whereas skewed numerical data were summarized by median and interquartile ranges. Categorical data were summarized as numbers and proportions. Comparisons were performed using an unpaired t-test and an analysis of variance for normally distributed numerical variables; Mann–Whitney-U and Kruskal–Wallis tests for skewed numerical variables; and χ 2 or Fisher's exact tests for categorical variables. Intention-to-treat analysis was applied, with a 2-sided p-value <0.05 being statistically significant.
Results
A total of 80 patients were randomized equally to LH or VH. Figure 1 shows the flow of the patients through the study. The initial patient characteristics were comparable in the 2 groups (Table 1). LH had a longer mean operative time than VH; the mean difference was 23.5 minutes; 95% CI (confidence interval): 10.8–36.2.

CONSORT [Consolidated Standard of Reporting Trials] flow diagram of the study. LH, laparoscopic hysterectomy; VH, vaginal hysterectomy.
Comparison Between the 2 Study Groups Regarding Demographic and Preoperative Data
Data presented as mean ± standard deviation, median (interquartile range), or number (percentage).
Unpaired t-test; bMann–Whitney-U test; cχ2 test.
LH, laparoscopic hysterectomy; VH, vaginal hysterectomy; yrs, years; BMI, body mass index; CD, cesarean delivery; CRP, C-reactive protein; H, hysterectomy.
Of those preoperatively scheduled, the performance rate of adnexal surgery overall (bilateral salpingectomy or BSO) was 62.5% in the LH arm, while it was much lower (27.5%) in the VH arm (Table 2). BSO was performed in 100% of the scheduled LH cases (17/17), compared to 40% (8/20) of the scheduled VH cases. Opportunistic bilateral salpingectomy without oophorectomy was performed in 35% of scheduled LH cases (8/23), compared to 15% of scheduled VH cases (3/20).
Comparison Between the 2 Study Groups Regarding Operative Data
Data presented as mean [95% confidence interval] ± standard deviation, median (interquartile range), or number (percentage).
Unpaired t-test; bMann–Whitney-U test; cχ2 test.
Bolded p-values are significant: **p < 0.01 is statistically significant; ***p < 0.001 is statistically highly significant.
min, minutes.
The 2 groups were comparable regarding blood loss; Table 2 shows medians of the complete data set with no disruption of data integrity. In addition, when outliers (2 VH cases: 620 and 720 mL, detected upon applying Tukey's rule) were omitted from analysis to obtain normally distributed data (verified by a Shapiro–Wilk test), there was also no statistically significant difference between mean blood loss; LH: 251.8 ± 81.6 mL; VH: 250.7 ± 85.3 mL; p = 0.9541; unpaired t-test. Five patients required blood transfusion. In the LH group, 2 patients had average blood loss (250 and 150 mL), received intraoperative transfusions due to low preoperative Hb (<10 g/dL); no postoperative transfusions were required. One of 3 patients in the VH group had a similar situation (blood loss 200 mL). The other 2 patients received postoperative transfusions to correct postoperative anemia (Hb <8 g/dL): 1 patient had below-average blood loss (90 mL) but required correction due to low preoperative Hb, while the other patient had excessive hemorrhage (720 mL) from a slipped uterine pedicle during a difficult ligation.
On subgroup analysis (comparing patients who underwent no adnexal surgery, bilateral salpingectomy, or BSO), no evidence was found that the extent of adnexal surgery affected operative time or blood loss in either of the study arms (Table 3).
Extent of Adnexal Surgery and Its Impact on Operative Time and Blood Loss
Data presented as mean ± standard deviation or as median (interquartile range).
One-way analysis of variance; bKruskal–Wallis test.
LH, laparoscopic hysterectomy; min, minutes; VH, vaginal hysterectomy.
There was no statistical difference regarding intra- and postoperative complications. The frequency of complications grouped according to the Clavien–Dindo 5-grade classification 11 and the risks of them happening during LH versus VH are detailed in Table 4. No febrile episodes were >38.5°C. One patient in the LH arm was converted to laparotomy after an inadvertent bladder injury during colpotomy, and her bladder was repaired by urologic surgeons. This patient was discharged from the hospital after 3 days with an indwelling urethral catheter, which was removed after 14 days with no residual disability noted at her follow-up.
Relative Frequencies of Complications in the 2 Study Groups According to Clavien–Dindo 11 Classification (Not Mutually Exclusive)
Data presented as number (percentage) and relative risk [95% confidence interval].
Fisher's exact test; bLH versus VH.
LH, laparoscopic hysterectomy; VH, vaginal hysterectomy; RR, relative risk; CI, confidence interval.
Pain intensity was lower in the LH group at 2, 6 and 24 hours postoperatively. The inflammatory response to surgery did not differ between the 2 groups— neither clinically (postoperative fever; Table 4) nor on laboratory tests (postoperative rise in CRP, Table 5). There was no difference between the 2 groups regarding length of postoperative hospital stay. However, the costs for LH were higher (Table 5).
Comparison Between the 2 Study Groups Regarding Postoperative Data
Data presented as median (interquartile range).
Mann–Whitney-U test.
Bolded p-values are significant: **p < 0.01 is statistically significant; ***p < 0.001 is statistically highly significant.
hrs, hours; Hb, hemoglobin; CRP, C-reactive protein; EGP, Egyptian pounds; USD, US dollars.
Actual uterine weight measured after uterine extirpation was strongly positively correlated with uterine weight estimated preoperatively via TVS (rs = 0.823; p < 0.0001). Operative times in both arms was significantly positively correlated only with estimated and actual uterine weights. Figure 2 shows scatter plots with regression lines and equations for operative times on estimated uterine weight for LH and VH. Blood loss, however, was not significantly correlated with any studied predictors (age, BMI, parity, number of previous cesarean deliveries, estimated or actual uterine weight, operative time, and whether bilateral salpingectomy or BSO was performed).
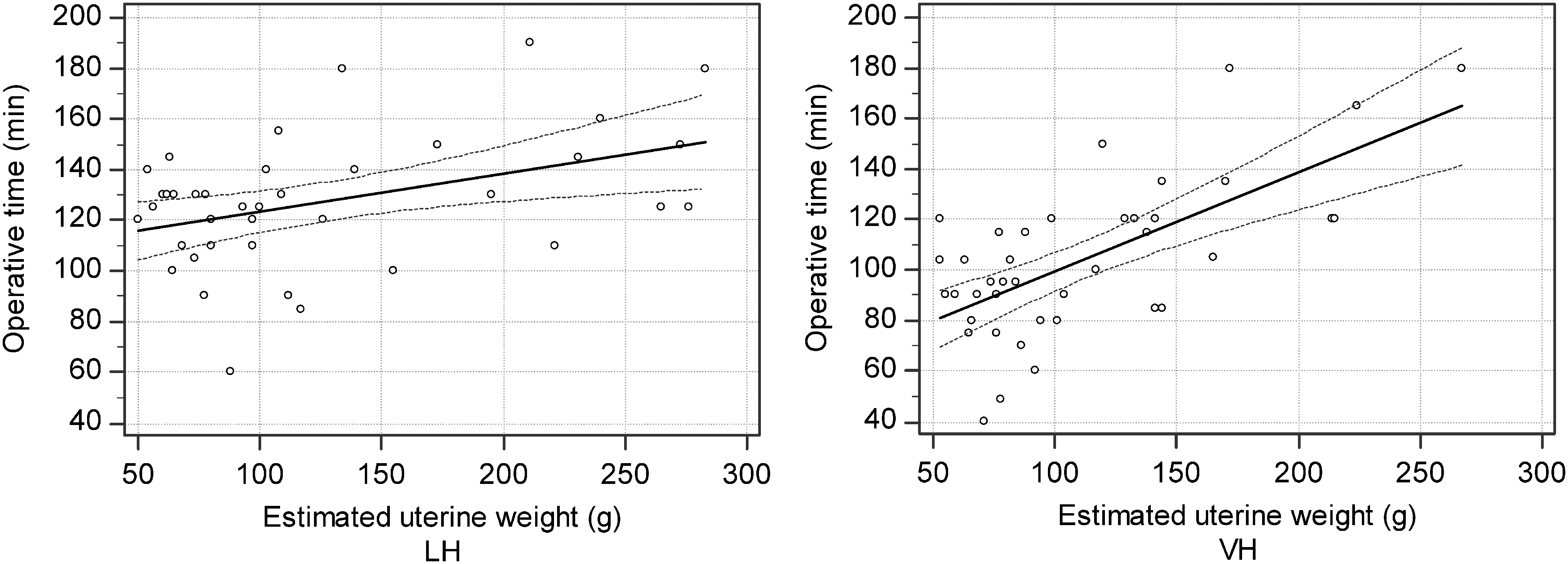
Scatter plots and regression lines (dashed lines bound the 95% confidence intervals [CI]) for the relationship between operative times (y) and uterine weights estimated preoperatively by transvaginal scan (x); left, in patients who underwent laparoscopic hysterectomy (LH), regression equation:
Data sharing
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Discussion
This prospective trial represents a vision for implementing minimally invasive hysterectomy for benign indications in limited-resource settings, where 80 patients, with no contraindications to vaginal or laparoscopic approaches, were randomized to undergo either of the 2 procedures. There were no statistically significant differences between the 2 groups regarding preoperative patient characteristics or indications for hysterectomy.
Operative time
The significantly longer mean operative time for LH compared to VH agrees with other studies.10,12,13 The operative times for both techniques in these studies was also significantly shorter than the current authors' corresponding counterparts, which is likely related to surgical expertise. The average estimated uterine weights being larger (yet still <300 g) in some studies10,13 supports this explanation. Nonetheless, Kim and others 14 reported a mean operative time of 149.3 ± 59.5 minutes for multiport LH in a university-associated hospital, which was significantly longer than its corresponding technique in the current study (p = 0.0224; unpaired t-test), showing that the performance at the current authors' institution was at least noninferior to some centers.
Operative time was significantly positively correlated with uterine weight in both LH and VH. In earlier studies, this relationship was reported with LH in some studies, 15 but not in others. 16 Bogani and coworkers 17 reported such a relationship in a collective population of both techniques together. Regression analysis on the current study's data showed that estimated uterine weight can explain 17% of the variations in operative times for LH, compared to 45% for VH. One can conclude indirectly that, for uteri <300 g, the influence of uterine weight on operative time is more pronounced in VH than in LH. Estimated uterine weight can possibly be used to predict operative time before the surgery, which can help when arranging the operative schedule in a busy operating theater and assigning a suitably skilled surgeon for each patient. It would also help designate patients whose cases would be appropriate for training, but this needs validation to detect a suitable cutoff.
Blood loss and blood transfusion
Median blood loss in LH and VH were significantly greater than the 100-mL medians reported by Ghezzi and coworkers 18 for both techniques. Likewise, no patients received blood transfusions in that study, compared to the current study's 5% (2/40) and 7.5% (3/40) in LH and VH, respectively. However, Allam and coworkers 19 reported significantly higher medians for blood loss in LH (350 mL) and VH (675 mL), which may be related to higher median uterine weights, although those weights were <300 g. This is reflected in that study's higher incidence of blood transfusions in VH (13.3%) but not in LH (3.3%). Notably, of the 5 transfusions in the current study (2 in LH and 3 in VH), only 1 VH was related to a technical difficulty.
Adnexectomy and opportunistic salpingectomy
Regardless of the route, there was a predilection to perform adnexal surgery when BSO was scheduled rather than bilateral salpingectomy alone. Although the difference in BSO rates between the LH and VH study arms was statistically significant, the difference in bilateral salpingectomy rates did not show statistical significance due to the small number of patients. The low rates of vaginal BSO were due to the unnecessary surgical risk in dealing with inaccessible ovaries with no adnexal pathology. The lower rates for salpingectomy alone, even during laparoscopy, were due to inaccessible tubes (vaginally) or perceived additional surgical risks from tubo-ovarian dissection (vaginal or laparoscopic) in the absence of a compelling indication.
The significant difference in performance of scheduled BSO between the 2 groups agreed with 2 other studies,10,20 in which adnexectomy was performed if it was scheduled preoperatively in 100% of LH cases, while, in 73% and 68% of VH cases, in these 2 studies respectively. While studying vaginal salpingectomy during VH, Antosh and coworkers 21 performed it successfully in 81% of these cases, with 11 minutes added to mean operating time and 6 mL added to estimated blood loss. In the 2 current study groups, however, patients who had no concomitant adnexal surgery did not consistently have shorter operations or less hemorrhage than patients who had bilateral salpingectomy or BSO. Nevertheless, this conclusion should not be generalized from a small number of events as in the current study.
Surgical complications
No complications more serious than Clavien–Dindo grade III occurred in the current study, and no significant differences were found between both arms regarding any grade of complications.
In the multicenter eVALuate study by Garry and coworkers, 12 there was no difference in major complication rates between LH and VH (9.8% versus 9.5%; p = 0.92). Of 336 LHs and 168 VHs: major hemorrhage was reported in 17 LHs (5.1%) and 5 VHs (2.9%); ureteric injury in 1 LH (0.3%) and none in VH; and conversion to laparotomy in 9 LHs (2.7%) and 7 VHs (4.2%). Fever was reported in 18 LHs (5.4%) and 12 VHs (7.1%).
In a retrospective study by Kim and coworkers, 14 of 366 multiport LHs, there were 4 bladder injuries (1.1%) and 5 ureteral injuries (1.4%); the total urinary-tract injuries was 2.5%.
A Cochrane review by Aarts and coworkers 22 found no evidence of a difference in risk of bladder injury in LH versus VH (odds ratio: 0.91 [0.32–2.56]). In a systematic review by Wong and coworkers, 23 bladder injury occurred in 0.24% of all benign gynecologic laparoscopies, with 91 incidents in 86,683 total laparoscopic hysterectomies (0.1%). The current study's rate of 2.5% and the relative risk of 3 were exaggerated due to the single incident of bladder injury and the small sample size.
Postoperative pain
Median pain intensity was consistently lower in the LH group in every postoperative evaluation, similar to the findings by Ghezzi and coworkers, 18 likely due to the more physiologic leg positioning and less traction on ligaments during LH than VH, despite the longer mean operative time. In addition, routine vaginal packing after VH likely contributes to the higher postoperative pain scores.
Inflammatory response
Albeit not routine in the current authors' practice, the surgical inflammatory response was tested in the current study's population as previous studies had reported contradicting results. Although the difference was nonsignificant, the clinical and laboratory inflammatory responses to surgery were less marked in VH than in LH, with a higher median increase in CRP and a higher rate of febrile morbidity in LH, compared to VH. Ribeiro and coworkers 24 also reported lower mean CRP values 24 hours postoperative in VH than LH. This may be related to the longer operative time for LH, or the use of surgical energy, with the associated—yet minimal—lateral spread and tissue necrosis. In contrast, Drahonovsky and coworkers 13 showed that VH had significantly higher rises in markers of inflammation (including CRP) and tissue trauma, as well as a higher rate of fevers, compared to LH. They attributed this finding to the frequency of vaginal-vault hematomas (25%) in their VH group, which was absent in the current study.
Length of hospital stay
Ghezzi et al. 18 reported significantly shorter hospital stays after LH than after VH (median 1 day versus 2 days). In the current study's patient groups, although nonsignificant, the median length of stay for LH (1.5 days) was longer than for VH (1.25 days), likely due to extra caution regarding the relatively recently implemented laparoscopic route than the more-familiar vaginal one. The current study's lengths of stay were significantly shorter than the 4-day medians for LH and VH in the eVALuate trial according to Sculpher et al., 25 which may be related to complications accounted for by their larger study population.
Health care costs
A cost-effectiveness analysis by Sculpher et al. 25 undertaken with eVALuate trial data by Garry et al. 12 concluded that LH is not cost-effective relative to VH. The marked difference is likely related to theater costs, reflecting differences in the time in theater and using disposable equipment for the laparoscopic procedure.
Study limitations
Performance of both techniques in patients with larger uteri and in obese patients was not covered, as the study focused on low-risk cases rather than special situations requiring additional expertise or having special technical and anesthetic concerns. Thus, these results should not be generalized to such populations. The current study was not sufficiently powered to detect differences in complication rates between the 2 techniques, especially rare events. Larger samples are also recommended to validate predictors likely affecting the key outcomes.
Conclusions
LH has longer operative time, compared to VH, yet has better postoperative pain profile. In low-resource settings, cost considerations make LH fall behind VH as a primary choice for benign hysterectomy; however, the similar complication rates of the relatively new laparoscopic approach, compared to the more-familiar vaginal approach would encourage the rising appeal for LH to replace open AH, whenever appropriate. The regression model to predict the operative time from preoperatively estimated uterine weight can help arrange the operative schedule in busy operative theaters and assign a suitably skilled surgeon for supposedly difficult cases. It would also help to designate operations appropriate for training, but this requires validation to detect a suitable cutoff.
Footnotes
Authors' Contributions
Dr. Moharram conceptualized the study and supervised it, and, together with Dr. Mohammad, worked on the methodology. Drs. Mohammad, Raafat, and Abdelrahman were responsible for resources, while Dr. Alqenawy performed the formal analysis. All of the authors were involved with writing the article's original draft; Drs. Mohammad and Alqenawy reviewed and edited the article; and all authors approved its final version.
Acknowledgments
This trial was registered in ClinicalTrials.gov, ID: NCT03692832.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this work.