
Abstract
Objective:
This Surgical Techniques report demonstrates the efficacy of laparoscopic management for complications of cesarean scar pregnancy (CSP). The study aim was to detail the procedure for treating 2 patients and report on their postsurgical outcomes.
Materials and Methods:
A study of 2 cases of CSP complications was conducted at a tertiary university hospital. The 2 women had CSP pregnancy terminations performed by evacuations at private clinics. They were susequently admitted to the tertiary university hospital with vaginal bleeding and pelvic pain. Cesarean-scar dehiscence and hematoma were noted in each patient. Both patients underwent laparoscopy. The hematomas were evacuated, and residual placental necrotic tissues were removed. The edges of the cesarean scars were stitched laparoscopically.
Results:
In both patients, no isthmocele formations were seen at the first-month follow-up.
Conclusions:
The laparoscopic approach may be an efficient option for patients with particularly complicated cases of CSP. (J GYNECOL SURG 38:408)
Introduction
The cesarean-section rate is increasing worldwide. Although the World Health Organization stated that ideal cesarean-section rates should be between 10% and 15%, 1 these rates are higher than 30% in most countries. 2 An increased cesarean-section rate results in more cesarean section–related maternal and fetal complications. The most-frequent complications are placental-adherence abnormality, uterine rupture, isthmocele, and cesarean-scar pregnancy (CSP). 3 All of these complications are related to one another.
First, the presence of an isthmocele—a cesarean scar defect or uterine niche 4 —is the major risk factor for CSP. It is also known that untreated CSP mainly results in placental-adherence abnormality. 5 Therefore, CSP should be treated immediately after diagnosis. Thousands of CSP cases have been reported up to the present.6,7 The dramatic increase in CSPs has spurred the development novel treatment approaches. Numerous treatment protocols are widely used and these protocols are published in the literature.1,8,9 There are various complications of CSP treatment, depending on the treatment approach. These approaches, while intended to help patients, may, in fact, cause complications, such as severe vaginal bleeding, uterine rupture, and retained placental tissue in the cesarean-scar region. 10
One of the most-preferred treatment approaches is dilation and (suction) curettage (D&C). However, patients may be admitted to a hospital with vaginal discharge, bleeding, or spotting after D&C.
It is difficult to manage patients with severe vaginal bleeding related to CSP treatment. Patients may even undergo hysterectomy due to uncontrolled uterine bleeding. Therefore, minimally invasive approaches have importance for addressing complications of CSP. Herein, is a study of 2 patients who had complicated CSPs with irregular vaginal bleeding after D&C. Each woman was diagnosed as having residual placental tissue in an isthmocele. These patients were treated via a laparoscopic approach. The study aim was to detail the treatments and outcomes for both patients.
Cases
Case 1
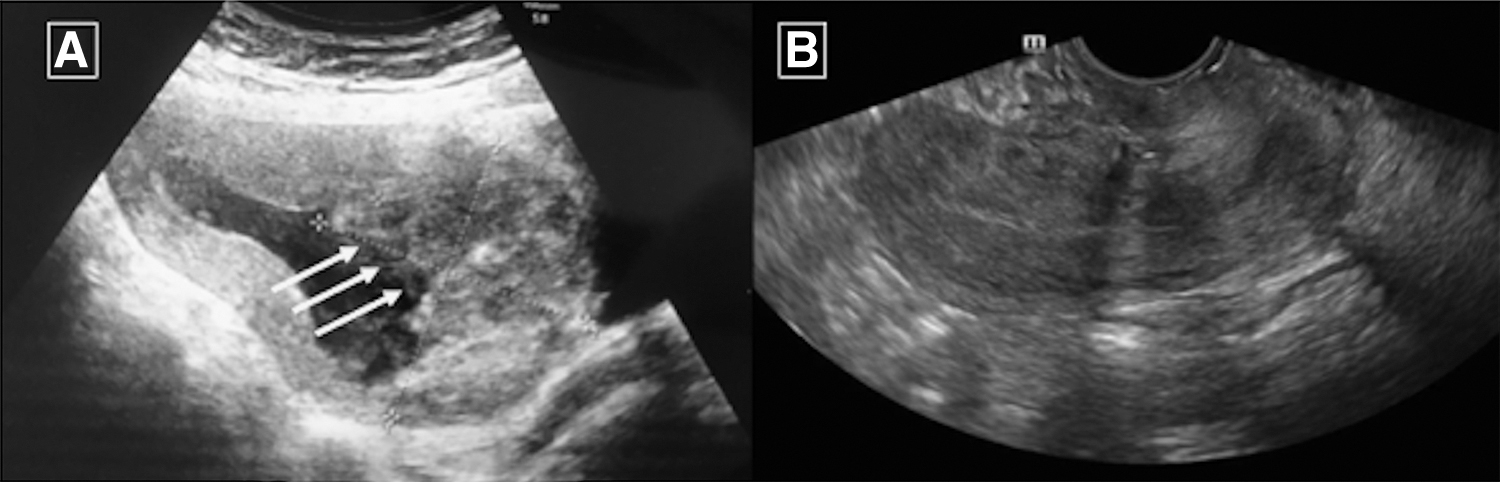
A 32-year-old woman who had undergone 2 previous cesarean sections was admitted to a private clinic for a first pregnancy check at 8 weeks of gestation for a new pregnancy. However, via transvaginal ultrasound (TVUS), she was diagnosed as having a missed abortus. After this diagnosis, a D&C was performed under general anesthesia. There was no pathologic findings in a postoperative TVUS scan. However, 1 week after being discharged from the clinic, she was readmitted with vaginal bleeding and abdominal pain. At that time, she had an 8-cm diameter hematoma in her cesarean scar (Fig. 1A). She was referred to a tertiary university hospital for surgical treatment, which involved laparoscopic excision of the residual tissue and hematoma as well as repair of her cesarean scar. Figure 1B shows a scan performed 1 month postsurgery.
Case 2
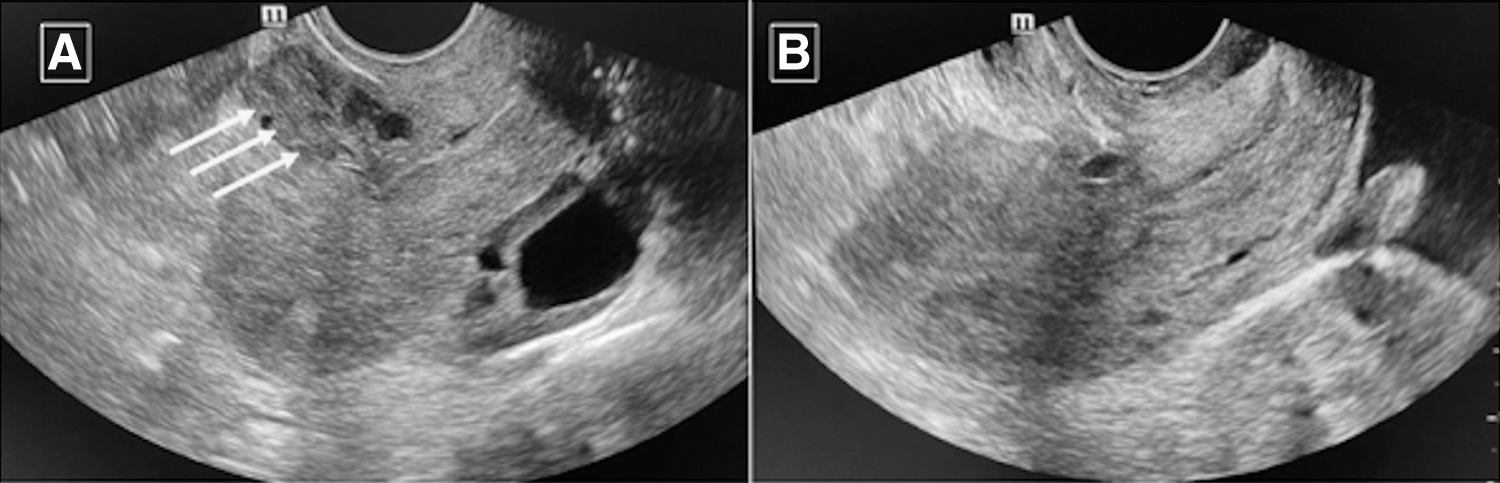
A 36-year-old woman with 1 previous cesarean section was diagnosed with a missed abortion during what would have been her seventh week of pregnancy. She underwent D&C and was discharged from the hospital without any complaints. After a couple of months, she had vaginal spotting. When she was scanned by TVUS, a 3 × 3–cm hypoechoic lesion was noted in her cesarean scar (Fig. 2A). It was considered to be a complication secondary to her CSP treatment. Therefore, laparoscopic surgery was planned, and the same procedure of Case 1 was performed for the patient. Figure 2B shows a scan performed 1 month postsurgery.
Ethics approval
Ethics approval for the study of the 2 patients' procedures was obtained from the Bursa Uludag University Clinical Trials Ethical Committee (Approval number: 2021-1/26).
Techniques
Laparoscopy setup
Both of these patients underwent laparoscopy after diagnosis. The operations were performed under general anesthesia. Each patient was placed in a dorsal lithotomy position. A Foley catheter was inserted into her bladder. A curette was inserted carefully into the uterine cavity and used as a uterine manipulator. After CO2 insufflation with a Veress needle through the umbilicus, a 10-mm port was placed intraumbilically for the telescope, and 2 other 5-mm ports were placed through the left superior and inferior quadrant for the surgeon.
Surgery
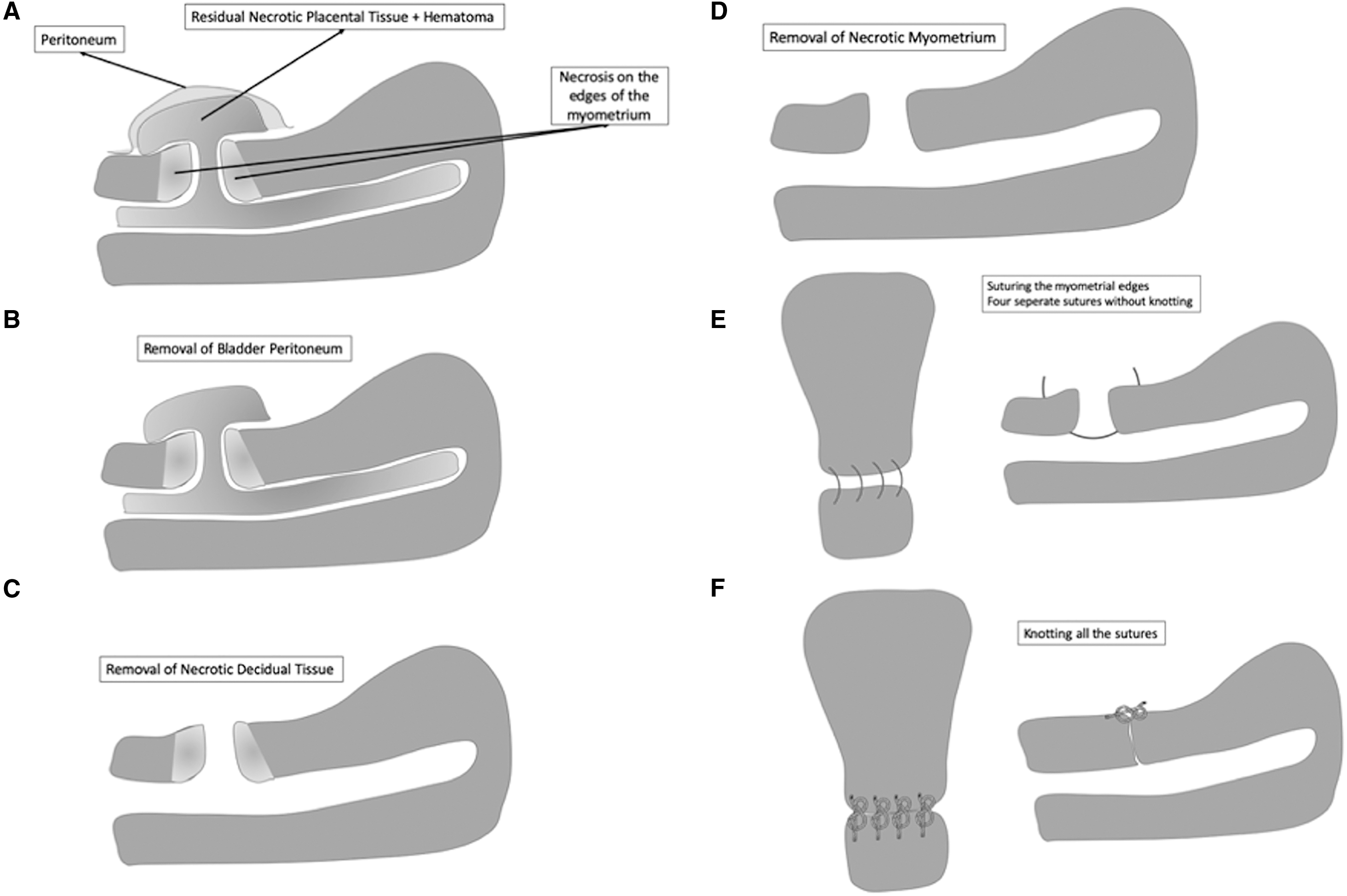
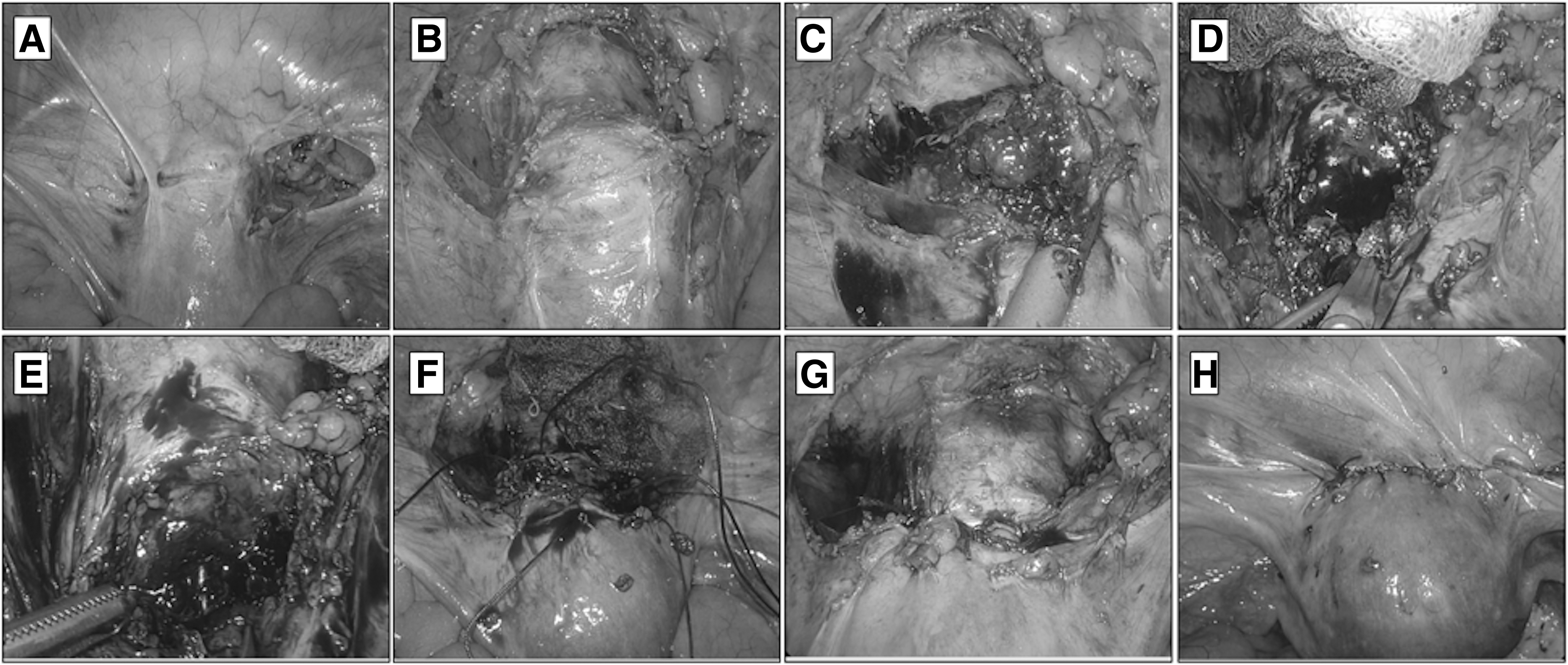
The peritoneum was carefully dissected over the bulging region. After peritoneal dissection, the bladder was captured with a grasper, and the vesicocervical space was dissected down to the cervicovaginal junction. The decidual tissue and hematoma were cleaned from the cesarean scar region (the isthmocele). Both upper and lower necrotic edges of the cesarean scar were cut and excised using laparoscopic scissors to avoid insufficient tissue healing and isthmocele recurrence. The curette was visible in the cervical canal after excision of the necrotic tissue.
The second part of the operation was suturing after visualizing healthy cervical tissue. First, the upper and lower parts of the incision were sutured with No.1.0 Vicryl sutures, which were not tied—and would not be until the last suture was in place. Next, the entire myometrium layer was sutured to avoid more isthmocele formation. Then, all of the sutures were knotted. After closure, the peritoneum was closed with No. 2.0 Vicryl. Both operations were performed by the same surgeon. Surgical steps of the operation are illustrated and labeled in Figure 3. Laparoscopic views of the steps are shown in Figures 4 and 5 and in Supplementary Video 1 (Supplementary Data are available online at: www.liebertonline.com/GYN).
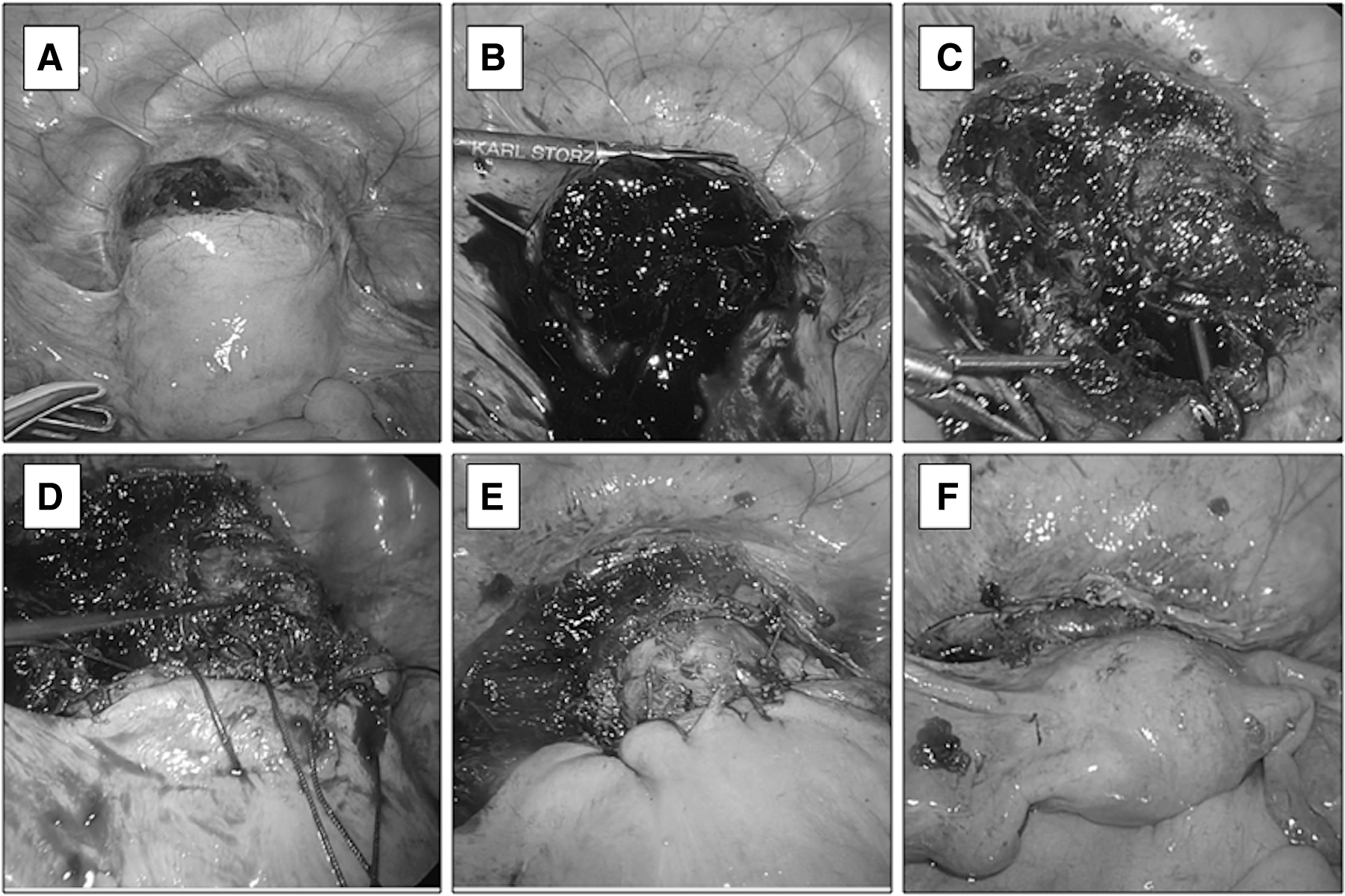
Laparoscopic views of each surgical step of Case 1.
Laparoscopic views of each surgical step of Case 2
Results
The patients were able to get up 6 hours postsurgery and were discharged the next morning. A TVUS scan was performed before discharge from the hospital. No isthmocele formation was seen after surgery. There were no symptoms, such as abnormal bleeding, spotting, or pain noted at the first postoperative month checkup. The pathologic investigation results revealed the presence of necrotic placental tissue and coagulum formations. Postoperative TVUS images of each patient are shown in Figures 1B and 2B.
Discussion
This study showed that laparoscopic management of complete uterine dehiscence due to late complications of CSP could be performed safely and efficiently. There are different treatment modalities of CSP. A review mentioned ∼14 treatment options for CSP. 7 Although numerous studies exist in the literature regarding such treatments, none of them are superior to each other. Most studies advise D&C as a safe option in particular cases. 11 However, blind-suction curettage may cause severe complications such as abnormal uterine bleeding, scar dehiscence, or retained tissue.
A few studies reported on managing persistent CSP or hematoma after D&C failure. Qian et al. advised using hysteroscopy to remove the retained tissue. 12 However, hysteroscopic resection of a huge hematoma, as seen in the 2 current cases, is nearly impossible. The laparoscopic approach provides isthmocele repair in addition to the hematoma suction. As far as the current authors were able to find, there is only one case report 13 in the literature about a postabortion cesarean-scar defect hematoma (3 × 3 cm) as occurred in the 2 current cases. In that prior report, the patient was clinically stable, a conservative approach was taken to address her case. 13 Prior to this report, there had been no other publication about surgical management of CSP hematomas in the literature.
Conclusions
The best treatment modality for CSP or its complications should be curative for CSP and isthmocele. The most-efficient and safe treatment modality has yet to be determined. The current authors suggest laparoscopic surgery as an optimal choice for patients with CSP complications, especially when these involve uterine dehiscence.
Footnotes
Authors' Contributions
Drs. K. Aslan, E.K. Aslan, and C. Mesut were the surgeons. Dr. G. Uncu designed the study, Dr. K. Aslan drafted and wrote the final version of the article. Dr. A. Orhan contributed by preparing figures and the supplemental video.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
The authors did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors for conducting this research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.