
Abstract
Background:
An interstitial ectopic pregnancy implants within the proximal and intramural portion of the fallopian tube that is enveloped by the myometrium. The high mortality rate in this type of pregnancy is due, in part, to delay in diagnosis, as well as from massive intraperitoneal hemorrhage. Excessive blood loss can occur after a rupture or during surgical treatment of an interstitial pregnancy. Several ways to reduce surgical blood loss have been reported. Our team's experiences and management tools are described in this article and in a video (Supplementary Video S1; Supplementary data are available online at www.liebertonline.com/GYN) Both show a laparoscopic approach for managing an interstitial ectopic pregnancy to reduce the risk of uterine rupture and to preserve future fertility. To minimize surgical blood loss, both uterine arteries are temporarily occluded with surgical clips.
Technique:
Laparoscopic cornual resection of a left interstitial ectopic pregnancy involves: (1) successfully identifying the ureters and uterine arteries, and occluding the latter by surgical clipping; (2) making a circular incision in the left horn up to the gestational sac; (3) removing the cornual capsule and ipsilateral fallopian tube; (4) enucleating the entire gestational sac; and (5) suturing the myometrial bed and repairing the incision.
Conclusions:
Laparoscopic cornual resection is appropriate for interstitial pregnancy in patients wishing to preserve fertility. Temporary occlusion of bilateral uterine arteries using surgical clips is a safe, effective, blood-sparing intraoperative technique. (J GYNECOL SURG 39:82)
Introduction
Interstitial ectopic pregnancy occurs when a pregnancy develops within the proximal and intramural portion of the fallopian tube that is surrounded by the myometrium. 1 This pregnancy is difficult to distinguish from an intrauterine pregnancy on ultrasound (US) due to the implantation site of the fallopian tubes and the invasion through the uterine wall. Interstitial ectopic pregnancy is a rare entity, representing 2%–4% of ectopic pregnancies. 2 The high mortality rate in this type of pregnancy is due, in part, to the delay in diagnosis, as well as massive intraperitoneal hemorrhage. 3
The aim of this article and online video (Supplementary Video S1; Supplementary data are available online at www.liebertonline.com/GYN) is to show a laparoscopic approach for managing interstitial ectopic pregnancies to reduce the risk of uterine rupture and to preserve future fertility. To minimize surgical blood loss, both uterine arteries are temporary occluded with surgical clips.
Technique
We present a case of interstitial ectopic pregnancy with initial medical treatment and later with cornual resection, with the aim of reducing the risk of uterine rupture and preserving future fertility.
To minimize blood loss during enucleation of the gestational sac, both uterine arteries and gonadal vessels are temporarily occluded with clips. A circular incision is made in the left horn, until reaching the gestational sac (Fig. 1). The cornual capsule and ipsilateral fallopian tube are removed. The gestational sac is enucleated in its entirety (Fig. 2). The myometrial bed is sutured, and the incision is repaired with Vicryl #1 (Fig. 3).
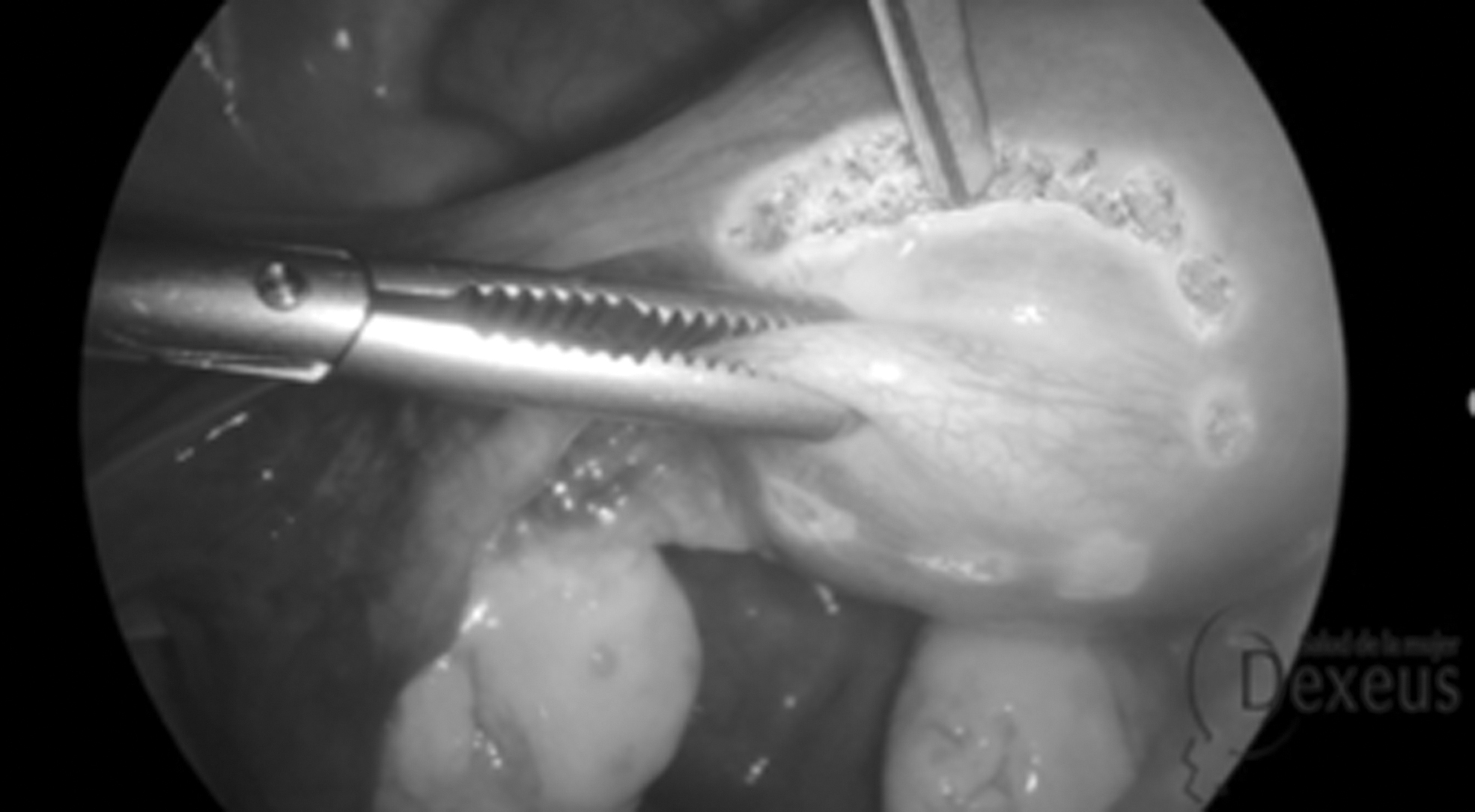
Circular incision in the left uterine horn.
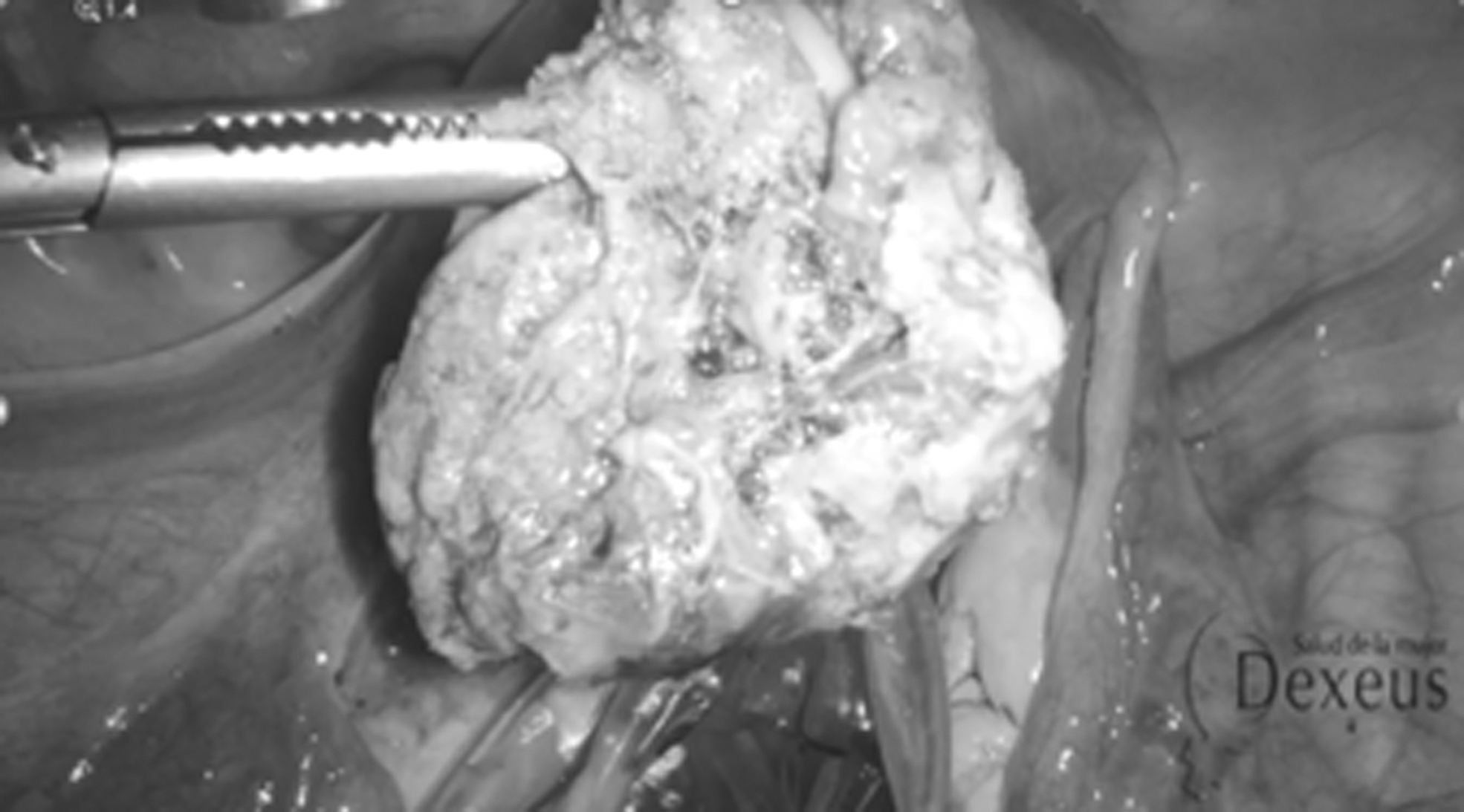
Enucleation of the gestational sac.
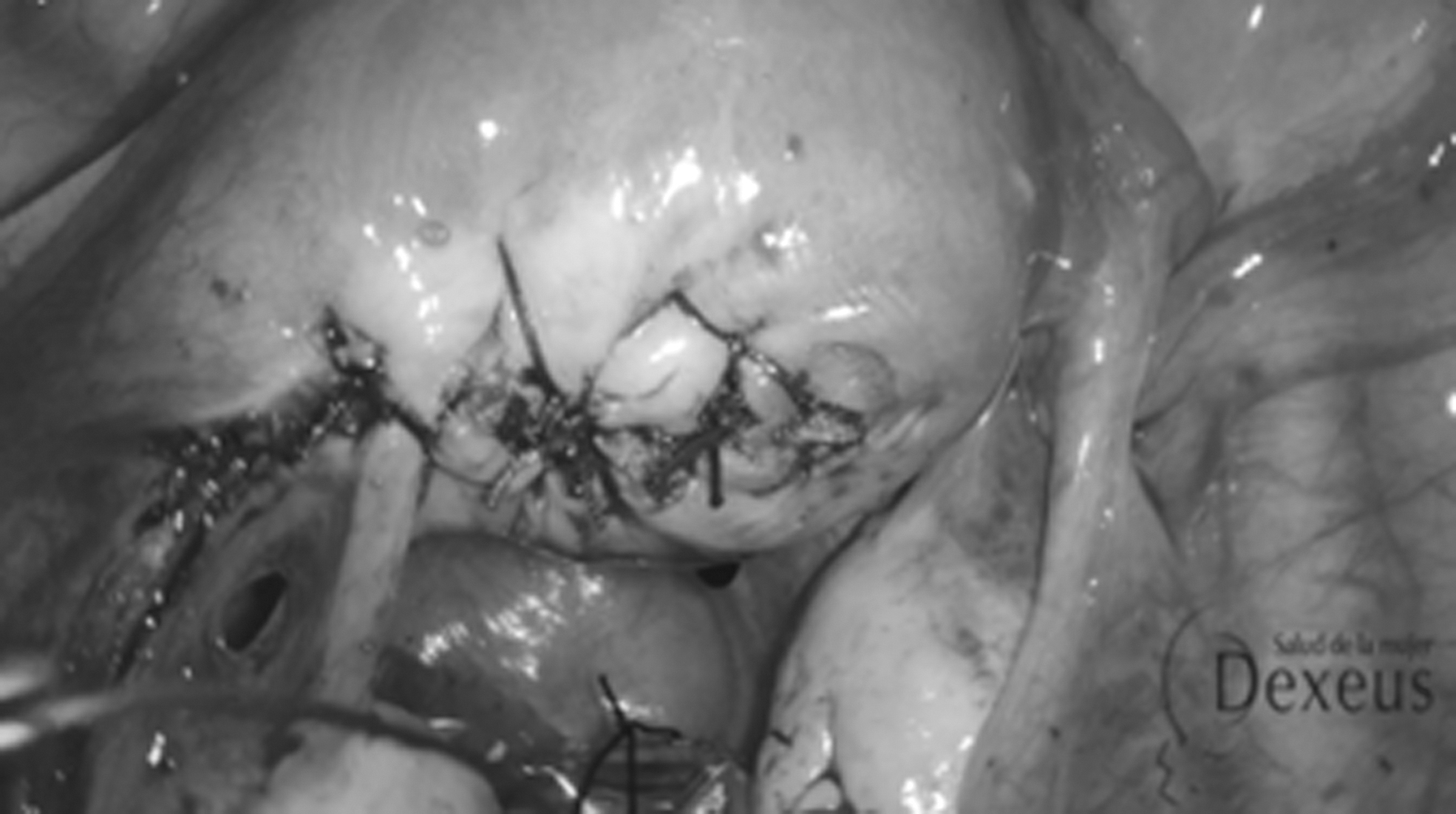
Uterine incision repair.
Video footage of the surgical technique is available online in Supplementary video S1.
Illustrative Case
A 36-year-old woman, with a diagnosis of a septate uterus and an obstetric history of a spontaneous twin pregnancy, that was monochorionic monoamniotic in one hemicavity and had a single gestational sac in the other hemicavity. She reported that the twin pregnancy was spontaneously interrupted in the first trimester. At 20 weeks' gestation, she was admitted to an outer center for premature membrane rupture due to an unknown cause, and received antibiotic therapy. Anhydramnios was found, so she decided to legally terminate the pregnancy. Remains evacuation curettage was performed. Subsequently, multiple intracavitary adhesions were visualized by gynecologic US and confirmed in a diagnostic hysteroscopy. Adhesiolysis of uterine synechiae was performed by surgical hysteroscopy. Another hysteroscopy was performed to perform a partial septoplasty.
After a diagnosis of ectopic interstitial gestation from an outer center in January 2019, she came to our center, stable and asymptomatic, in May 2019. She provided reports that described 2 curettages with US controls in which no gestational sac located in the area that had been reached. A posterior hysteroscopy was performed, in which a septal uterus and Asherman's syndrome were found. Adhesiolysis was performed without reaching the gestational sac. Due to this patient's clinical and hemodynamic stability—and a laboratory analysis showing a ß–human chorionic gonadotropin (ß-hCG) level of 127 mIU/mL—medical treatment with intramuscular methotrexate (MTX) was administered; this required 2 doses to reduce her ß-hCG level of 24 mIU/mL successfully was verified.
Gynecologic US was performed in our center, and visualization of the gestational sac remained in the vascularized left horn in its periphery (Fig. 4).
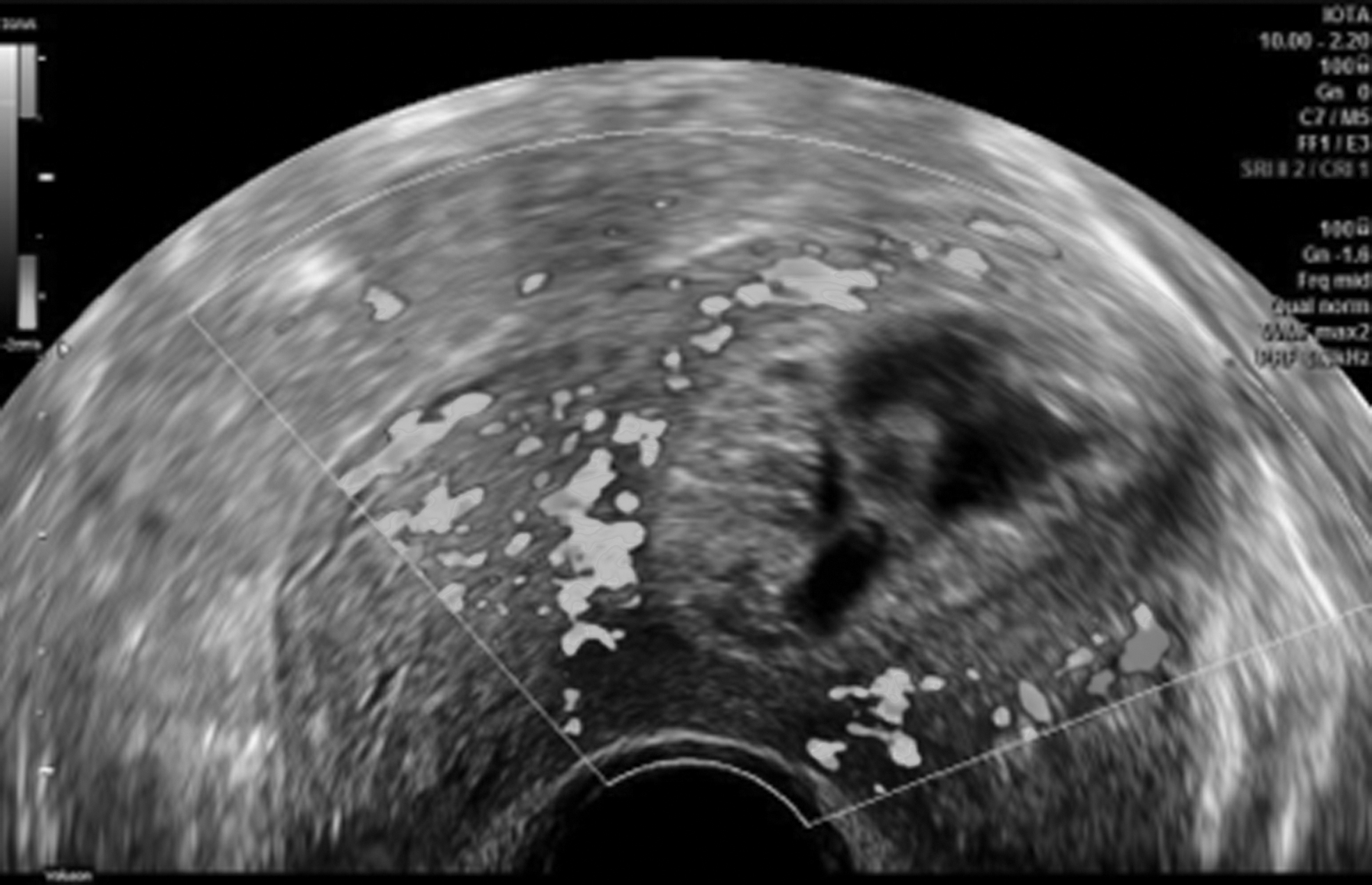
Nodular image in the left horn compatible with vascularized blood material.
An analytical control visualization was performed, resulting in a hemogram and coagulation tests compatible with normality and negative ß -hCG.
A surgical approach was agreed on to lessen the risk of uterine rupture in future pregnancies. She underwent laparoscopic left cornual resection.
Her The postoperative period was uneventful. The histopathologic report confirmed the products of gestation.
At 3 months, an US control was performed, without observing a gestational sac or adhesions. The patient was informed about the risk of uterine rupture in a next pregnancy, as well as the need to end it by elective caesarean section.
Discussion
Despite the fact that interstitial pregnancy is one of the most lethal types of ectopic pregnancy, there is no agreement about its management due to its rarity. Conservative treatment of these cases includes MTX injection, administered systemically or locally in the uterus. 4 Cornual-wedge resection is the most commonly used surgical intervention for interstitial pregnancy. The main disadvantage of this treatment is that it disrupts the myometrial lining, which reduces fertility potential. 4 Newer, less-invasive, surgical procedures, such as hysteroscopy with US assistance and uterine evacuation under laparoscopic supervision, have been shown to be both safe and effective. These novel techniques minimize blood loss during surgery while maintaining the uterine lining for potential future pregnancies. 4
Occluding both uterine arteries with surgical clips also has the potential to reduce intraoperative blood loss. In a recent case-controlled study, this procedure reduced average blood loss by ∼50% during laparoscopic myomectomy. 5
In the future, the eventual recurrence rate, pregnancy rate, and pregnancy complications should be investigated.
Conclusions
In patients who want to preserve their fertility, laparoscopic corneal resection appears to be an effective treatment for interstitial pregnancy. Temporary occlusion of bilateral uterine arteries with surgical clips is a safe and effective blood-sparing intraoperative technique.
Footnotes
Authors' Contributions
Drs. Sánchez-Prieto, Barbany, and Barri-Soldevila conceptualized the project. Drs. Barbany and Barri-Soldevila worked on clinical interpretation. Drs. Sánchez-Prieto, Barbany, and Platón performed video editing. Drs. Sánchez-Prieto and Platón wrote the original draft of the article. Both of them, together with Drs. Barbany and Barri-Soldevila, wrote, reviewed, and edited the final version. All of the authors read and agreed to that version.
Author Disclosure Statement
No conflicts of interest exist.
Funding Information
The authors did not receive financial support for the research, authorship, and publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.