
Abstract

Dear Editor:
The umbilicus is the optimal and most-used primary laparoscopic entry site because of its central position, lack of subcutaneous fat or muscles, and maximal proximity of the skin to the peritoneum; this site also bleeds less when operated on. In exceptional situations, whenever a surgical site was inaccessible or risky, open laparoscopy or alternative entry sites have been suggested. Open laparoscopy still carries a risk of visceral or vascular injury. 1 The left upper abdomen (i.e., Palmer's point or the ninth intercostal space), the middle upper abdomen (i.e., Lee–Huang's point), or the right upper abdomen (i.e., Latif's point) access points (shown in Fig. 1) require certain precautions. These include ascertaining the absence of upper abdominal organomegaly and stomach emptying. Yet, there are still some risks of vital-organ injuries. 2
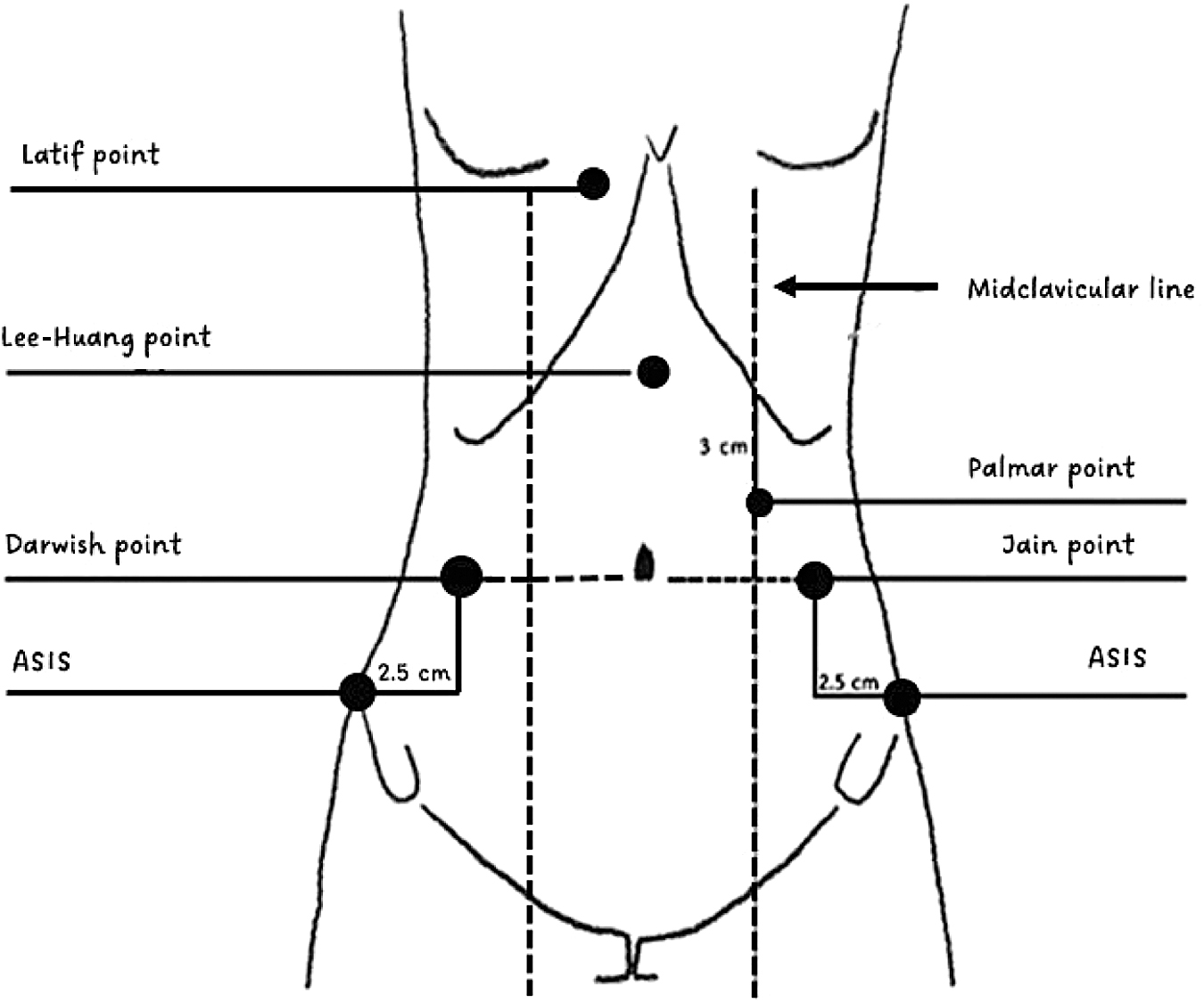
Diagrammatic presentation of some alternative laparoscopic entry sites. ASIS, anterior superior iliac spine.
A left lumbar region point (Jain's point) was suggested by a team of researchers. 3 This entry point was overused in more than 7802 cases, omitting the established superiority of umbilical-port entry without clear indications for this. An alternate entry site is recommended when umbilical placement of a primary trocar is deemed hazardous. However, these researchers reported minor complications in 265 cases and 1 colonic injury. Moreover, the researchers reported subcutaneous and omental emphysema caused by an occasional undershoot or overshoot of a Veress needle, simply because the spring-safety part of the needle was lost as the surgeon's index finger was placed on the shaft of the needle.
The, Darwish point is a right-sided mirror image of the Jain point (Fig 1). A Veress needle is inserted into a point on the right side at the meeting point of the transverse plane at the level of the umbilicus and an imaginary vertical line 2.5 cm medial to the anterior superior iliac spine. The patient is positioned horizontally without gastric deflation of air or fluid, as the Darwish point is right-sided. A naso- or orogastric tube is invasive and is associated with some complications. When utilizing the Darwish point, there need not be elevation of the anterior abdominal wall to place a Veress needle, as this elevation increases the risks of failed entry and confers no advantage for avoiding vascular or visceral complications. 4 Unlike when accessing Jain's point, when accessing Darwish's point, the needle is grasped at the housing to allow easy and safe passage of the spring-loaded stylet when it is inserted into the abdomen. Moreover, a saline aspiration test is essential to ensure free intraperitoneal insertion. The point being right sided is more ergonomic, as it enables easy perpendicular insertion of the needle by a right-handed surgeon.
We used this point in a patient with umbilical endometriosis with many prior incisions in the upper-abdominal, left-lumbar, and suprapubic regions. This patient had signed consent to publish information about her case with complete anonymity. The Darwish point was used successfully to access the abdomen in a safe way and was advantageous over a left-sided entry. This is a promising safe entry site that should be evaluated in further studies.