
Abstract
Abstract
Objectives:
Many studies showed high rates of noncompliance with preoperative antibiotic prophylaxis (PAP) guidelines but a lack of data on reasons. This study assessed compliance with PAP guidelines, reasons for noncompliance, and its effect on infectious complications.
Materials and Methods:
This facility-based retrospective study was based on an audit of antimicrobial practices among surgeons after implementing the PAP guidelines. Details of surgery and antimicrobial prophylaxis for patients undergoing cesarean section/gynecologic surgeries were recorded on an Antibiotic Audit Form. Any deviation from guidelines was considered noncompliance, and its reason was assessed. After finding the rate of noncompliance the rate of postoperative infections was compared between patients who received recommended antibiotic prophylaxis and those who did not.
Results:
Per 532 Antibiotic Audit Forms (114 for gynecologic surgeries; 418 for cesarean sections), there were 196 cases of noncompliance (36.8%), using additional antibiotics. Most commonly, these were given for extensive adhesiolysis (29.7%) in gynecologic surgeries and prolonged rupture of membranes (14.2%) in cesarean sections. Surgical-site infection was more common in obstetric patients receiving additional antibiotics after cesareans.
Conclusions:
PAP compliance is good if guidelines are locally developed by consensus and are sustainable. An internal audit enhances compliance by exploring reasons for noncompliance, providing self-feedback. Surgeons tend to continue antibiotics for prolonged leakage, extensive adhesiolysis, and comorbidity. (J GYNECOL SURG 39:114)
Introduction
Surgical-site infection (SSI) is one of the most-feared complications of surgical procedures, with the reported incidence being 2%–20%.1,2 SSI rates have been shown to decline from 8.6% to 2.9% if preventive measures are followed as a bundle. 3 Preoperative antibiotic prophylaxis (PAP) is an essential component of the SSI Prevention Bundle, with a specific goal of reducing colonization pressure of microorganisms during surgery. This can be mostly achieved with a single dose of an antibiotic that is active against commonly encountered pathogens.4,5 For gynecologic and obstetric procedures (generally clean or clean-contaminated surgical wounds), a preoperative mono-antibiotic regimen with a first-generation cephalosporin is recommended.6,7 There have been numerous reports of indiscriminate and prolonged use of antibiotics.8–11 This practice not only harms patients 12 and adds to the cost of treatment, 13 but has also led to the emergence of resistant microbes.
Materials and Methods
In the Post Graduate Institute of Medical Education and Research (PGIMER), Sector 12, in Chandigarh, India, where this study was conducted, an Antimicrobial Stewardship Committee reviewed existing literature and guidelines on PAP and drafted an evidence-based preoperative antibiotic prophylaxis policy for obstetrics and gynecology. This policy was discussed extensively by the faculty members, revised according to their input, and adopted into clinical practice during 2015–2016. See Supplementary Table S1 (supplementary data are available online at www.liebertpub.com/gyn).
Many studies have shown a high incidence of noncompliance with PAP guidelines, but hardly any probes have been made into the factors that lead to noncompliance. At PGIMER, also, stepping down from the earlier practice of 7 days of broad-spectrum antibiotics to a single preoperative dose was surrounded by hesitancy.
Methodology
Three main strategies were adopted to ensure compliance. First, was dissemination of guidelines among resident doctors and nursing staff and the organization of orientation programs to foster awareness and encouragement to adopt the antibiotic policy. Second, a regular practice of audit of prophylactic antibiotic prescriptions was adopted to assess the incidence of noncompliance. Third, reasons for nonadherence were explored. For this, each operating surgeon was required to mention the reason for deviating from the policy on a special Antibiotic Audit Form (Fig. 1) . This step was taken based on the idea that good compliance could be expected only if exact situations were found that caused surgeons to deviate from the PAP guidelines.
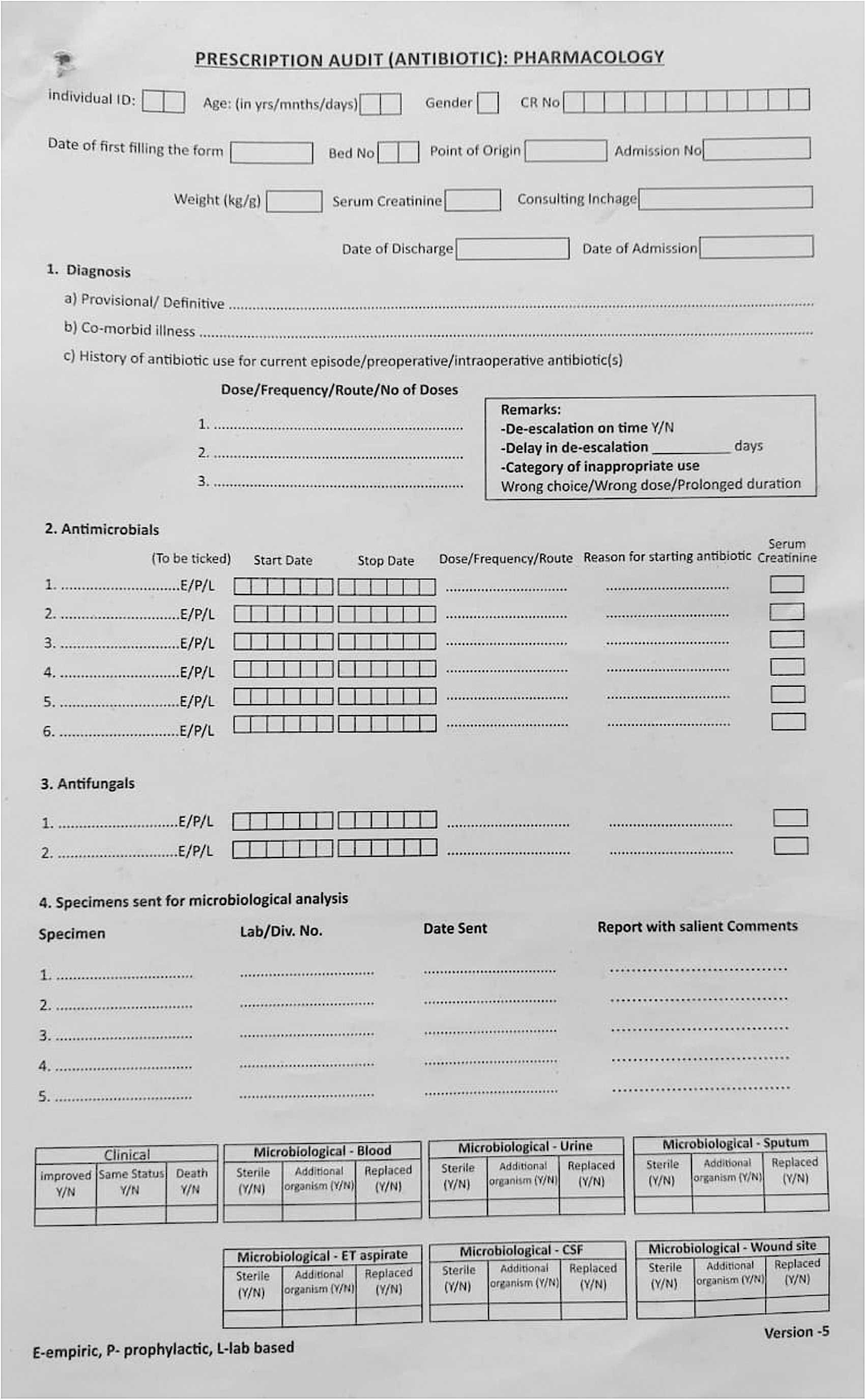
Antibiotic Audit Form.
This retrospective study was based on analysis of audit forms that met the inclusion criteria. Information related to surgical procedures, antibiotics used, duration of antibiotics, and postoperative infections were extracted. The rate of compliance with PAP guidelines and reasons for noncompliance were analyzed. Furthermore, the incidence of infections was compared between patients who received antibiotics according to PAP guidelines and patients who did not.
PAP policy
After the implementation of PAP guidelines in the department of obstetrics and gynecology, surgical procedures for which antibiotics would/ would not be given were identified. A single dose of cefazolin (2 g, 30–60 minutes before surgery) was recommended for most procedures. A repeat dose was allowed if the duration of surgery exceeded 3 hours or if blood loss exceeded 1500 mL. A maximum of 3 doses of cefazolin 8 hours apart were permitted if the surgeon desired to continue antibiotics after the operation. For patients who were allergic to cephalosporins, a combination of clindamycin and gentamicin was recommended.
Antibiotic Audit Form
The structured Antibiotic Audit Form (Fig. 1) was prepared by the faculty members from the clinical pharmacology department. From then onward, this became an integral part of the inpatient records for all patients and had to be furnished for any inpatient who was prescribed antibiotics. For each patient undergoing surgery, the form was duly completed by a member of the surgical team and sent to the antibiotic audit team.
For this retrospective study, all the audit forms gathered over a timeperiod of 5 months were scrutinized critically for completion.
Inclusion criteria
All cases of patients undergoing cesarean sections and gynecologic surgeries were eligible for this analysis if the Antibiotic Audit Forms were completed.
Exclusion criteria
Cases of patients who had been receiving therapeutic antibiotics for other reasons were excluded as were those cases for which there were incomplete Antibiotic Audit Forms.
Use of the form
The information collected through this form included diagnosis, indication for surgery, comorbid illness(es), and details on antibiotic prescription. Data were also captured on postoperative infections until 30 days postsurgery, management of infections, and the need for therapeutic antibiotics. Any deviation from the provisions of the PAP policy was considered noncompliance. In case of noncompliance, details of noncompliance, such as wrong timing, wrong choice of prophylactic antibiotic, or additional antibiotics in the postoperative timeperiod, were noted. The reason for deviation from policy, as documented by the surgical team, was noted. Diagnosis of, and classification of SSI, were established according to U.S. Centers for Disease Control and Prevention criteria. 14 Clinical and microbiologic details of SSIs were recorded.
Outcome measures:
The rate of compliance with the PAP policy was sought as were reasons for noncompliance to the PAP policy. The rate of postoperative infections was compared between patients who received recommended antibiotics and patients for whom the surgeons deviated from the policy.
Ethics
This study was based on the data provided on the Antibiotic Audit Forms that were furnished regularly to the surgeons and staff for all the cases of patients undergoing surgical interventions. As the form was a part of the inpatient records of all the patients, per hospital policy, separate formal consent from patients was not considered. This retrospective study was approved by the Institute's Ethics Committee.
Results
Baseline data
There were 532 Antibiotic Audit forms eligible for analysis. Of these, 114 forms were for gynecologic procedures, and 418 were for cesarean sections. The median age of the patients who underwent gynecologic surgeries was 42 (interquartile range [IQR]: 35–52 years) and that of obstetric patients was 28 (IQR: 25–31 years). Of 114 gynecologic patients, 49 (42.9%) were operated on for malignant tumors and the rest of the patients for benign conditions. The most-common procedure was staging laparotomy (with total abdominal hysterectomy [TAH] with bilateral salpingo-oophorectomy with omentectomy; 26.3%), followed by TAH with or without salpingo-oophorectomy for benign disorders (17.5%). See Table 1. Common indications for cesarean sections were prior cesarean section (24%) and fetal indications (fetal distress, poor biophysical profile). See Table 1. Of 418 cesarean sections, 327 (78.2%) were performed in emergency situations.
Details of Gynecological Surgeries and Caesarean Sections
Other gynecologic procedures include colpoperineorrhaphy, vaginoplasty, excision of rudimentary horn, salpingectomy/salpingo-oophorectomy, sacrospinous fixation, tubal recanalization, and utero–vaginal anastomosis.
Complications of labor include deep transverse arrest, nonprogress of labor, obstructed labor, and suspected scar dehiscence.
Other indications for cesarean section include in-vitro fertilization conception, cord prolapse, cephalopelvic disproportion, dilated cardiomyopathy, triplets, macrosomia, preeclampsia with pulmonary edema, and repair of urethra–vaginal fistula.
MSL, meconium-stained liquor; REDF; reverse end diastolic flow.
Of 114 patients, 27 (23.7%) who underwent gynecologic surgeries, and of 418 obstetric patients, 133 (31.8%) had medical comorbidities. The most-common medical condition among patients undergoing cesarean section was chronic hypertension; other conditions were diabetes, thyroid disorders, anemia, epilepsy, heart disease, chronic kidney disease, neurologic disorders, musculoskeletal disorders, liver disorders, and thrombocytopenia. Comorbidities suffered by patients undergoing gynecologic surgeries included hypertension, diabetes, anemia, chronic obstructive pulmonary disease, congenital adrenal hyperplasia, and psoriasis. The majority of patients had multiple comorbidities.
The median hospital stays were 6 days (IQR: 5–8 days) for gynecologic patients and 8 days (IQR: 6–12 days) for patients undergoing cesarean section. The main reason for a prolonged postoperative stay after a cesarean section was prolonged stay of the newborn in the nursery, mostly due to prematurity and low birth weight. It is the hospital's policy to discharge the mother and baby together.
Antimicrobial prophylaxis
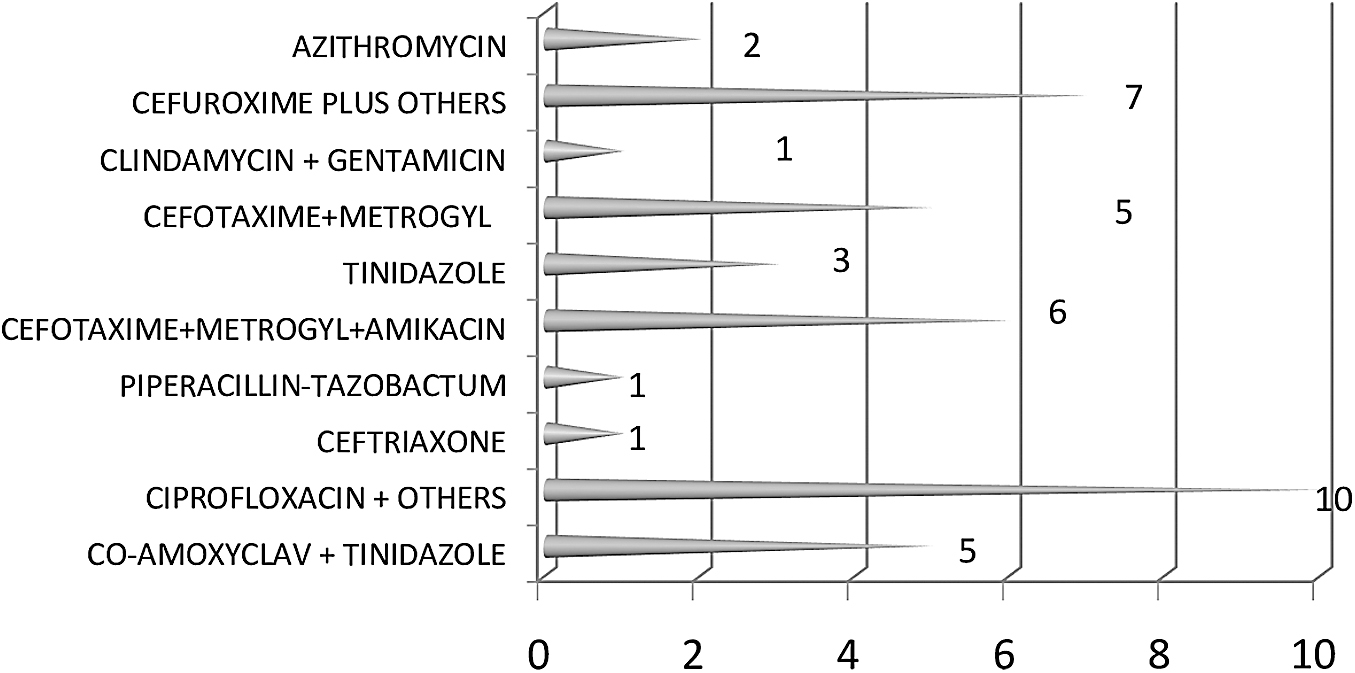
Surgeons were compliant with the choice and timing of preoperative antibiotic prophylaxis. In 30 of 114 patients (26.3%) operated for gynecologic indications, and in 5.5% of patients undergoing cesarean section, additional doses of cefazolin were given in the postoperative timeperiod (median number: 3; IQR: 2–3). Forty-one of 114 patients (35.7%) who underwent gynecologic surgeries and 155 of 418 patients (37.08%) who underwent cesarean sections received additional antibiotics, resulting in an overall noncompliance rate of 36.8%. The choice of antibiotics was highly variable (as shown in Figs. 2 and 3). Mostly multiple antibiotics were prescribed. Reasons cited by the surgeons for additional antibiotics were prolonged labor or leakage; the need for extensive adhesiolysis; and associated comorbidities such as anemia, postchemotherapy status, and diabetes (Table 2). Additional antibiotics were continued for a median of 2 days (IQR: 2–3 days).

Additional prophylactic antibiotics administered in the postoperative timeperiod following cesarean sections. PIPTAZ, piperacillin–tazobactum; CLINDA, clindamycin; AMOXYCLAV, amoxicillin/clavulanate; METROGYL, brand (®) of metronidazole.
Additional prophylactic antibiotics administered in the postoperative timeperiod following gynecologic procedures. METROGYL, brand (®) of metronidazole; AMOXYCLAV, amoxicillin/clavulanate.
Indications for Additional Antibiotics Cited by the Surgeons
Patients on therapeutic antibiotics for chorioamnionitis were not included; noncompliance was in the form of prescribing additional antibiotics in the postoperative timeperiod.
Other indications for continuing antibiotics after cesarean section include cord prolapse, second-stage cesarean, postpartum hemorrhage, heart disease, and manual removal of placenta.
Other indications for continuing antibiotics after gynecologic surgery include postchemotherapy status, bowel injury during surgery, and common cold.
PTPROM, preterm premature rupture of membranes.
Postoperative infections
Postoperative infections were noted in 4.5% of postcesarean section patients and in 12.3% of patients who underwent gynecologic surgeries (Table 3). Overall, 2.9% of obstetric patients and 11.4% of gynecologic patients developed SSIs. All SSIs were superficial. Postoperative infections required therapeutic antibiotics for a median of 7 days (IQR: 5–7 days); this occurred in 3 of 14 gynecologic patients, and in 14 of 19 obstetric patients (Table 3).
Details of Postoperative Infections
SSI, surgical-site infection; PPH, postpartum hemorrhage; UTI, urinary-tract infection; co-amoxyclav, co- amoxicillin/clavulanate.
The incidence of postoperative infections was similar among patients who received additional antibiotics and patients who received antibiotics according to the protocol. The rate of SSIs was found to be rather higher among obstetric patients who received additional antibiotics (Table 4). There was no significant difference in SSIs among patients with associated medical disorders, irrespective of whether or not they received additional antibiotics.
Comparison of Postoperative Infections Between per Protocol Antibiotic Group and Additional Antibiotics Group
SSIs, surgical-site infections.
Discussion
There was fair compliance of 63.2% with the PAP policy. This compliance was better than that reported in previous studies, which included patients with “clean” or “clean-contaminated” wounds. 15 Nonadherence was only in the form of extending prophylaxis to the postoperative period with additional antibiotics. In previous investigations on compliance, antibiotics had been continued for an extended duration in 62%–100% of patients.8,9,16,17 In a large study from Australia, including 9351 surgeries and 15,395 prescriptions, the most-common reason for inappropriate postprocedural prophylaxis was continuation for more than 24 hours, as occurred in 54.3% of cases. 18
There was a highly variable choice of antibiotics in the postoperative timeperiod. The most commonly used alternative antibiotics were cefotaxime plus metronidazole with or without amikacin in 54.6% of cases of noncompliance. Other studies have also reported using a wide variety of antibiotics postoperatively, such as cephamycins, amoxicillin/clavulanate, and second-generation cephalosporins. 11 One study reported use of 25 different parenteral antibiotic regimens in the majority of the patients in that study. 9
In order to reduce use of postoperative antibiotics, it is important to understand surgeons' perspectives. In the current study, the surgeons were encouraged to document on the Antibiotic Audit Form the reasons for continuing antibiotics. Common reasons cited for continuing antibiotics after cesarean section were prolonged rupture of membranes or diabetes, while, following gynecologic surgeries, surgeons preferred to give postoperative antibiotics if the surgical procedure was prolonged (irrespective of intraoperative re-dosing) or required extensive adhesiolysis (Table 2).
Existing guidelines, including the PAP guidelines, do have provisions for additional intraoperative re-dosing in cases of excessive blood loss or prolonged duration of surgeries. Patients with preterm rupture of membranes are prescribed prophylactic antibiotics for latency, but, in the absence of chorioamnionitis, these patients do not need additional antibiotics. Yet, surgeons preferred to give additional antibiotics to prevent infections. On the contrary, Moges et al. reported a higher risk of SSI among patients who received antibiotics for more than 24 hours, compared to patients who received them for a lesser duration (odds ratio [OR] = 3.5; 95% confidence interval [CI]: 1.22–10.17; p = 0.02). 19 In another study, 97% of patients who developed SSIs had received postoperative antibiotics, and, in 78% of cases, these antibiotics were continued for more than 24 hours. 20
In the current study, there was no significant difference in composite infectious morbidity between patients who received antibiotics per the protocol and patients who received additional antibiotics. The rate of SSIs among the gynecologic patients who received additional antibiotics was similar to patients who received recommended antibiotics, but among patients undergoing cesarean section, the incidence of SSIs was higher among patients who received additional antibiotics (6.5%), compared to patients who did not (0.8%). Among the 12 obstetric patients who had SSIs, patients who underwent emergency cesarean sections (n = 7) and cesarean hysterectomies (n = 3) received additional antibiotics, while patients who had elective cesarean sections (n = 2) received antibiotics per protocol.
Being a multispecialty tertiary-care center, the PGIMER receives most of the emergency referrals from neighboring states. Hence, more than 75% of cesarean sections in this Institute are performed on an emergency basis. Emergency cesarean sections have a higher baseline risk of SSIs than elective cesarean sections. Additional antibiotics do not offer any advantage in terms of preventing SSIs. One large prospective study on 12,299 patients did not find an increase in SSIs (2% versus 2.1%; p = 0.67) after switching from a 24-hour regimen to a 1-dose antibiotic regime for elective surgeries, 21 while another study found a moderate reduction in the risk of superficial SSI after decreasing use of postoperative antibiotics. 22
Certain factors—such as medical diseases (OR: 5.76), American Society of Anesthesia score >3 (OR: 12.8), and concurrent surgical procedures (OR: 3.26)—have been identified as risk factors for SSI, 23 but prescribing extra antibiotics in the postoperative timeperiod does not reduce SSI risk in such patients because the rationale for giving antimicrobial prophylaxis remains the same (i.e., to maintain an appropriate concentration of antibiotics in serum and tissues during the course of surgery). Being a tertiary-care referral center, the PGIMER also receives most of the patients with malignancies and medical comorbidities from surrounding states. Nearly 24% of gynecologic patients and 32% of patients undergoing cesarean section in the current study had one or another medical disorder. There was no difference in SSI among the subset of patients with medical disorders whether or not they received additional antibiotics (Table 4).
Despite implementation of PAP guidelines, antibiotics are being indiscriminately used for extended durations. Some investigators have even expressed a need for a local infection-control committee to ensure compliance with appropriate antibiotic prophylaxis.24,25 Lack of awareness and agreement among surgeons have been found to be important reasons for noncompliance.17,24 While formulating the antimicrobial policy at the PGIMIR, these factors were explicitly considered. For example, most guidelines do not recommend antibiotic prophylaxis for laparoscopic procedures. After extensive discussion among the faculty members, the consensus was in favor of giving mono-antibiotic prophylaxis for laparoscopic procedures. Hence, this was incorporated into the Institute's policy in order to ensure compliance.
Anticipated logistic barriers were also considered and resolved. For example, the PGIMER cesarean operating room (OR) is adjacent to the labor-ward complex. Thus, it was decided that antibiotic prophylaxis would be administered before shifting patients from the labor ward. However, transit from a patient's bed in the gynecology ward to the gynecology preoperative room takes ∼20 minutes, as the ward and OR are on different floors of the building. Some delay occurs due to anesthesia review and to allow some time to allay a patient's anxiety, especially among those with malignancies. Thus, it was decided that the antibiotic would be given after arrival in the OR. After giving antibiotics, some time would be utilized to complete the checklist, administer anesthesia medications, and prepare the surgical site, so that, between 30 and 60 minutes would elapse between antibiotic administration and first incision.
A regular orientation program was scheduled every 6 months. Hence, all the potential barriers—such as lack of consensus, lack of awareness, and logistic issues—were addressed carefully. Given that all possible internal logistic matters were resolved before implementing the policy, compliance with administering preoperative antibiotics and the timing of this administration were excellent. This was reinforced further by furnishing the checklist in the OR. However, in 1 retrospective study, only 69.90% of patients received preoperative antibiotic prophylaxis, 9 and in another study, there was very low compliance (23.8%) with the appropriate dose of antibiotic. 23 Some researchers have reported inappropriate timing as the major reason for noncompliance8,18 as observed in >44% of their patients. 18
In the current study, even when additional antibiotics were prescribed, they were given for 48–72 hours. Thus, along with a reduction in postoperative antibiotics from 100% to 36%, duration also was reduced from 7 days to 48–72 hours, which was fewer than the 5 days (range: 3–7 days) days as reported in another study. 17 In a 2021 retrospective study including 814 patients who underwent cesarean sections, 100% of patients received postoperative antibiotics for a mean duration of 6.75 ± 1.39 days. 9 The current study audit provided evidence for the lack of any benefit of additional postoperative antibiotics for preventing infections.
Strengths
This study had methodological strengths. Data were collected through a standardized form. Standard definitions were used for surveillance of SSIs and evaluations of deviation from antibiotic policy were made objectively. The reason for nonadherence to the protocol was an open-ended question. This brought to light indications that otherwise would not have been recognized, such as cough and common cold.
Limitations
To ensure full compliance with furnishing of the Antibiotic Audit Form, it was kept simple and included only the most relevant details. Hence, clinical data other than surgical details were not collected.
Conclusions
Compliance with PAP guidelines can be improved by adopting a locally agreeable and sustainable, evidence-based antibiotic policy and conducting an internal audit to generate self-evidence for within an institution. This self-feedback is important to bridge the gap between knowledge and clinical practice. Common reasons to continue antibiotics postoperatively are prolonged labor or leakage, the need for extensive adhesiolysis, and comorbidities. Additional antibiotics do not offer any advantage in terms of preventing postoperative infections.
Footnotes
Authors' Contributions
Dr. Singla conceptualized the study with support from Drs. Suri and Shafiq. Drs. Singla and Shafiq developed the methodology, while Drs. Suri and Shafiq were responsible for resources. The investigation and formal analysis were conducted by Drs. Singla and Veermalla, with Dr. Rohilla participating in the investigation. Drs. Suri and Kalra supervised the work. The original draft of the article was written by Dr. Singla with assistance of Dr. Veermalla. Dr. Suri was responsible for reviewing and editing the article's content with assistance from Drs. Shafiq, Rohilla, and Kalra. All of the authors approved the final version of the article and took responsibility for all aspects of the work.
Author Disclosure Statement
No financial conflicts of interests exist.
Funding Information
No funds, grants, or other forms of support were received during the preparation of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.