
Abstract

This article reports on the history of a 62-year-old (gravida 2, para 3) female, never-smoker, who presented with a large, retroperitoneal pelvic mass ascending from the cervical stump. Her past surgical history included a cesarean section in her youth and a supracervical hysterectomy (SCH) for a uterine leiomyomata 11 years ago.
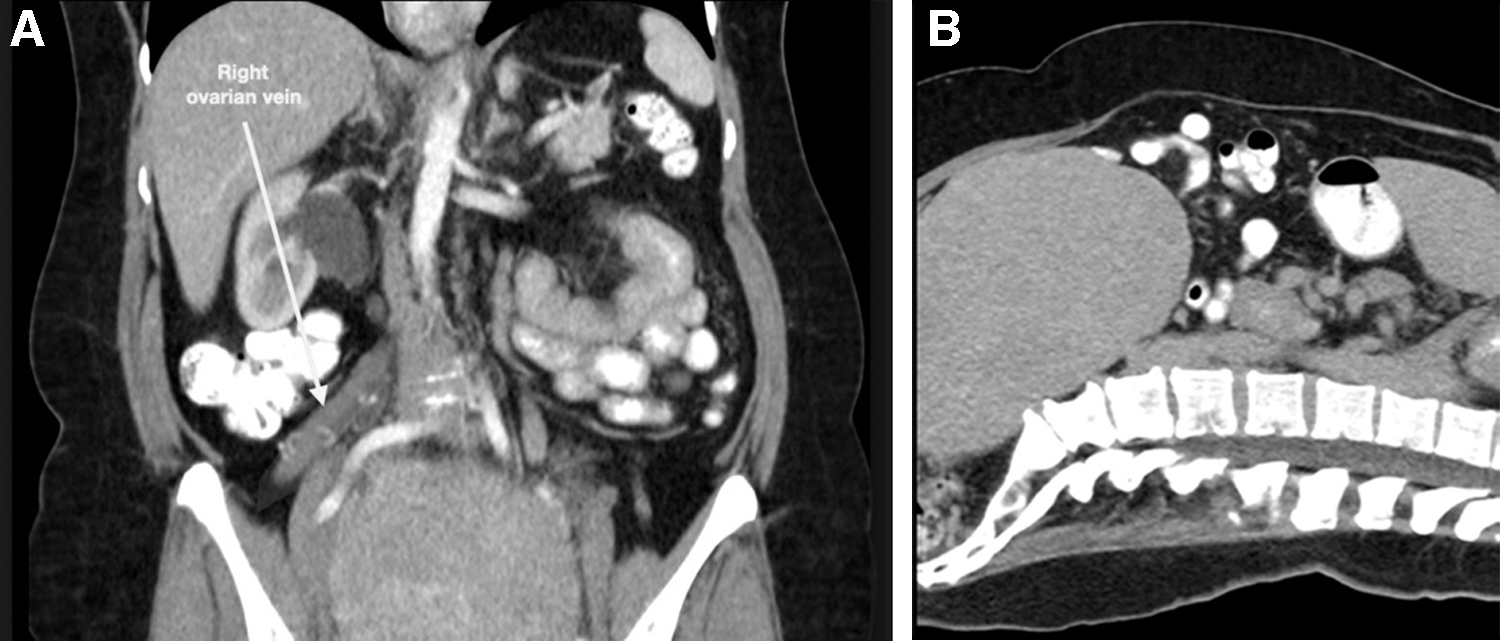
A preoperative computed tomogram revealed a 13 × 15 × 19–cm mass, compressing the right ureter with moderate right hydronephrosis. The uterus was surgically absent. The right ovarian vein was enlarged (Fig. 1). Despite the patient's history of a SCH, the cervix was not visualized radiographically; the preoperative diagnosis was a right ovarian fibroma.
The patient underwent a laparoscopic operation, confirming that she had a right retroperitoneal mass. The ureter's location was not initially prioritized per the assumption that the ureter would always be posterior to an ovarian mass. The mass was enucleated from the retroperitoneum laterally and anteriorly. The densely adherent bladder was dissected off the mass with an incidental 5-mm cystotomy and culdotomy, enabling the mass to be removed. Pelvic assessment for hemostasis of the exposed retroperitoneum did not reveal the ureter. Proximal transection of the ureter was identified at the pelvic brim, and the distal transection of the ureter was 1 cm from the ureterovesical junction. An examination of the mass revealed a 6-cm adherent portion of the ureter (Fig. 2).

The massive leiomyoma, with a 6-cm segment of ureter and no identifiable cervical tissue.
Final pathology revealed a 1600-g, 17.0 × 14.0 × 12.5–cm cellular leiomyoma with a 6-cm segment of ureter, that was negative for malignancy. Nuclear radiographic evaluation of the right kidney revealed significant loss of function, ascribed to chronic hydronephrosis. The patient's postoperative creatinine level was high at 1.2, suggesting persistent accommodation from chronic hydronephrosis. Follow-up nuclear imaging corroborated the inauspicious renal function. Consequently, there was a discussion on treatment alternatives to preserve the kidney, but an elective right nephrectomy was performed 6 weeks postoperatively.
An intraperitoneal leiomyoma arising from a cervical stump is highly unusual; from 1927 to 2012, there were only 3 reported cases of recurrent myoma following SCH. 1 Another noteworthy aspect of this case is that the patient's ureter was initially thought to be posterior to the ovarian fibroma. Differential diagnosis of pelvic masses by computed tomography or magnetic resonance imaging can be suggested by assessment of the mass's anatomy and vascularity. 2 However, given that preoperative imaging of mass's pelvic tumors can be imprecise— especially when the ureter is not initially delineated within the pelvis—the definitive location should not be assumed. In the present case, the preoperative imaging was unsuccessful at identifying the exact location of the ureter in the pelvis (i.e., a few cm beyond the kidney), and this was not pursued further. Conversely, a computed tomographic urogram would have depicted the anterior deviation of the ureter.
The current clinical scenario exemplifies the combination of multiple rare features that were adverse and unpredictable, confounding accurate diagnosis. Ultimately, when a massive tumor obscures identification of the ureter's route preoperatively, additional radiographic investigation and surgical identification of the ureter should be prioritized.
Ethics
No institutional review board (IRB) approval was sought as this was not required per IRB regulations. According to the Western Institutional Review Board, retrospective analysis of a single patient's experience with standard treatment does not meet the IRB's definition of research and does not require review or exemption by the IRB. Although using protected health information to prepare this article did not require IRB review, the authors of this case report complied fully with the Health Insurance Portability and Accountability Act of 1996 guidelines. Written patient consent was obtained prior to the initiation and development of this article.
Footnotes
Acknowledgments
This project was supported by the Women's Cancer Research Foundation, and by Joan and Len Rullo, in memory of Elizabeth Johnson.
Authors' Contributions
Drs. Rettenmaier and Micha conceived the idea, developed, and wrote the article and, together with Dr. Goldstein, reviewed the clinical data and performed the final editing. Drs. Bohart and Goldstein evaluated the imaging and clinical data, reviewed the article's content, participated in draft preparation, and conducted the final review.
Author Disclosure Statement
No financial conflicts of interest exist.