
Abstract
Objective:
Shear-wave elastography (SWE) can be used to obtain quantitative information about tissue stiffness. This study compared SWE measurements of patients with adenomyosis, leiomyoma, and normal myometrium.
Materials and Methods:
This study included 56 women who were scheduled to undergo hysterectomy. Measurements of the uterine myometrium and leiomyomas, if any, of the patients were preoperatively collected through SWE. A total of 69 SWE measurements were included.
Postoperatively, the patients were categorized according to the results of histopathologic examinations: group 1 included patients with normal myometrium; group 2 included those with adenomyosis; and group 3 included those with leiomyomas. The Emean values of the kPa obtained from the SWE measurements were compared with the histopathologic results.
Results:
The SWE measurements of groups 2 and 3 were significantly higher than those of group 1. There were no significant differences between groups 2 and 3 in mean SWE measurements. The success rate of SWE in differentiating normal myometrium and adenomyosis was 92%, with a sensitivity of 93.1% and a specificity of 82.1%.
Conclusion:
This study revealed that using ultrasound elastography to diagnose adenomyosis is successful in distinguishing that condition from normal myometrium, but SWE is not useful for distinguishing adenomyosis leiomyoma. (J GYNECOL SURG 39:177)
Introduction
Adenomyosis is a uterine pathology characterized by the presence of endometriotic-tissue islets within the myometrium; the condition is difficult to diagnose and treat. 1 The prevalence of adenomyosis islets in the myometrium in hysterectomy series is between 5% and 70%. 2 The incidence of adenomyosis is 20%–48% among infertile women and 70% among those with chronic pelvic-pain syndrome. 3 When endometriotic tissue invades the entire myometrium, the condition is called diffuse adenomyosis; when the tissue occupies a localized area, it is called adenomyoma. An adenomyotic uterus is often accompanied by uterine leiomyomas. Differentiating between the 2 uterine pathologies can be difficult; ultrasonography (US) useful for their diagnosis. 1
In clinical practice, adenomyosis is usually diagnosed using US, magnetic resonance imaging (MRI), and hysteroscopy4,5; however, the final diagnosis of adenomyosis is confirmed through histopathologic analysis.
In 2015, the international Morphological Uterus Sonographic Assessment (MUSA) consensus article provided the terminology to be used for sonographic identification of myometrial lesions. Accordingly, adenomyosis may present in the uterus as globular growth, asymmetrical myometrial thickness, a myometrial cyst, echogenic subendometrial lines and buds, hyperechogenic islands, fan-shaped shadows, irregular and discontinuous junctional zones, and translesional vascularization seen on color Doppler ultrasound. 6
US elastography is a novel noninvasive imaging method used for in vivo evaluation of tissue flexibility and stiffness. This method can help detect lesions early and provide additional information on lesion characteristics through morphologic changes on seen on grayscale US. US elastography can also be used to learn some additional information, such as the progression severity of some diseases and to evaluate their responses to treatment. 7
There are two main methods of elastography. Strain elastography (SE) involves direct application of pressure to the tissue and estimating the resulting components of the strain tensor. In contrast, for shear-wave elastography (SWE) tissue is subjected to low-frequency (< 1 kHz) vibrations and the tissue's behavior is detected with ultrasonic or acoustic means. 8
SE has certain limitations, because it can be used to obtain qualitative or semiquantitative results by applying pressure to the probe. SWE is a way to obtain quantitative tissue-elasticity data during US examinations. The current study compared the values for normal myometrium, adenomyosis, and leiomyoma that were confirmed by histologic analysis using SWE.
Materials and Methods
This study was conducted after obtaining approval of the ethics committee of Firat University, Elazığ, Turkey (August 5, 2021). Written informed consent was obtained prior to the study from all participating patients. Patients examined and scheduled to undergo hysterectomy for various indications in the department of obstetrics and Gynecology of the Firat University Hospital's faculty of medicine between April 2021 and February 2022 were examined prospectively.
Patients with low SWE-image quality owing to deep localizations (several reasons, including large waist circumferences and retroverted uteri); patients with myometrial and endometrial malignancies; and patients undergoing hormone-replacement therapy were excluded from the study. Ultimately, 56 patients were included. One day prior to the surgery, each patient was examined with US and subjected to myometrial examination using elastography to collect preoperative measurements. Pressure was not applied when performing the examination. One more measurement was performed for leiomyomas in patients with simultaneous leiomyomas in their uteri. Localization of the areas where the measurements were made were noted. Lesions that were >8 cm deep were excluded.
After hysterectomy, the areas of measurement was marked on the uteri specimens and sent for pathologic analysis. The patients were categorized according to the results of their histologic analyses of the marked areas as: group 1, normal myometrium; group 2, adenomyosis; and group 3, leiomyoma. Tissue stiffness was examined with reference to these histologic results. In addition, each patient's age; parity; and symptoms, such as pelvic pain and dysfunctional uterine bleeding, were recorded; and their association with tissue stiffness was examined.
SWE
SWE was performed by a radiologist with 21 years of experience in radiology and with 7 years of experience in SWE and gynecologic US. Preoperatively, all patients were allowed to rest for 5 minutes and then each patient was examined in a supine position using a digital US device with SWE software (GE Logic S8 xdCLEAR 2.0, Korea) in the radiology department of Fırat University Hospital. SWE examination was performed after B-mode US examination using a 2–5 MHz convex probe. During the evaluation, grayscale and elastography images were recorded digitally.
Notably, SWE is a dynamic sonoelastography technique that did not require manual compression. The patients were asked to hold their breath to ensure image stability during the examination. The field of view (FOV) was determined by centralizing the uterine myometrium, and stiffness was visualized as a color scale within this area.
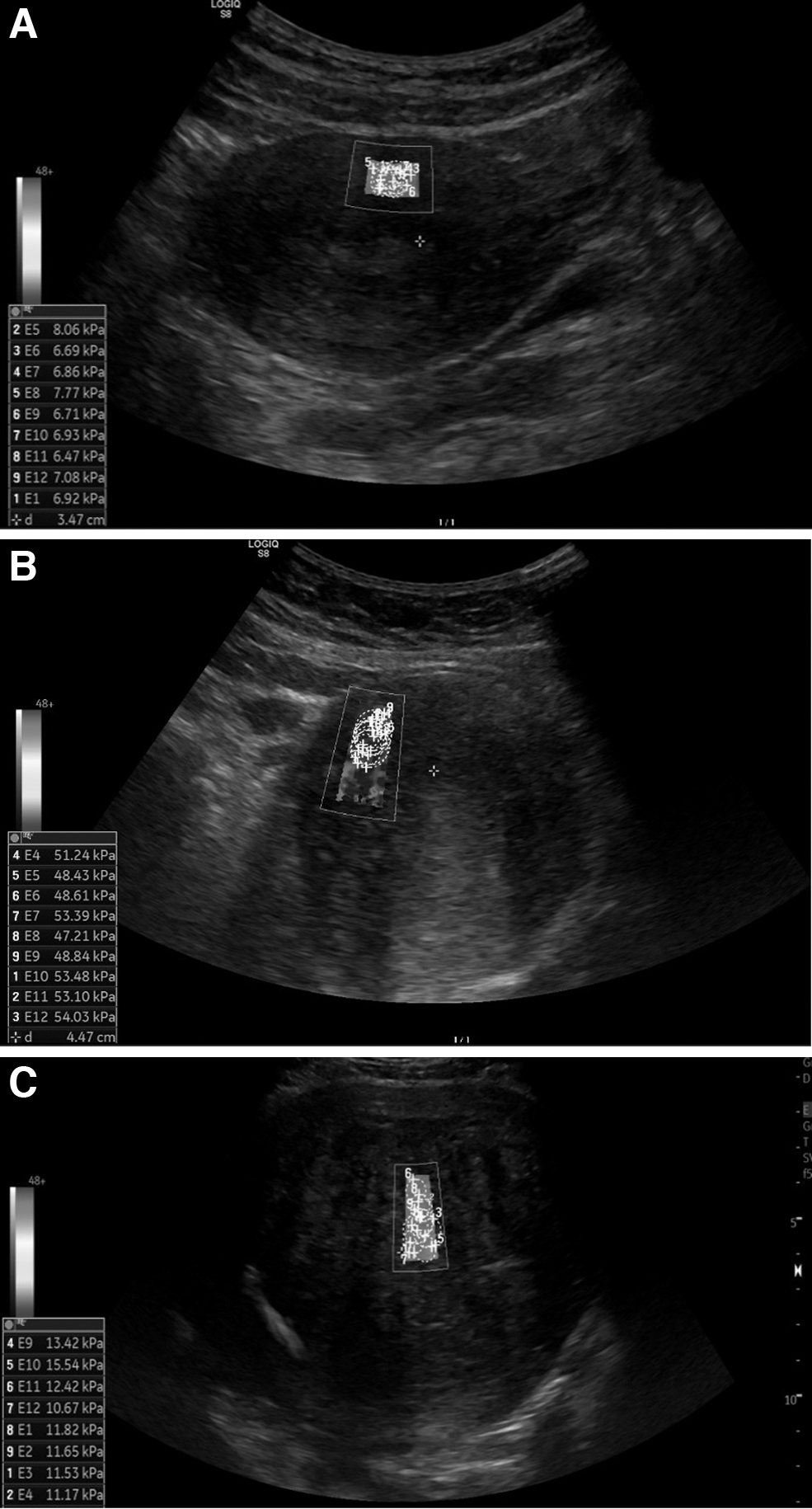
Moreover, if adenomyotic foci, myoma uteri, etc., were present, they were also centralized, and corresponding B-mode imaging was conducted to visualize the margins of the tissues. In the FOV, the region of interest (ROI) cursor was placed on the stiffest part of the lesion according to the color scale, and shear-wave velocity was measured with the ROIs placed to fill the stiff part. Most of the lesions were measured with a single ROI after noting that there was no significant difference in the measurements of a single ROI conducted at least 3 times. This procedure was repeated 10 times and the median values were determined (Fig 1). The mean MQL/R [monitoring query language/reference] value was 15,7 %. The shear-wave velocity of the lesions was converted to Emean values of kiloPascals (kPa) and recorded. Images and measurements were recorded digitally. When the lesions were >8 cm deep, the lesions were noted but no measurements were performed.
Histopathologic examination
Postoperatively, the extracted uterine specimens were placed in 10% formaldehyde solution and sent to the pathology department for analysis. The specimens were cut into sections and examined after hematoxylin–eosin staining.
Statistical analyses
An IBM SPSS Statistics, version 25.0, package program was used for all statistical analyses of the data. Median, minimum, and maximum values were used to express continuous variables. Categorical data were expressed as percentages. The normality of the continuous variables of each group was analyzed using Kolmogorov–Smirnov and Shapiro–Wilk tests, and Spearman correlation analysis was used for the nonnormally distributed variables. A Mann–Whitney-U test was used to compare the 2 groups, and a χ 2 test was used to compare categorical data.
Receiver operating characteristic (ROC) curves were drawn to assess the diagnostic values of ultrasonic elastography and pathology results. A p-value of <0.05 was considered statistically significant for all analyses.
Results
A total of 69 measurements were conducted for 56 patients scheduled for hysterectomy. According to the pathologic results for the patients, 28 had normal myometrium, 28 had adenomyosis, 1 had an adenomyoma, and 12 had leiomyomas. The ages of the patients ranged from 35 to 76 years. There were no statistical differences between the patients with normal myometrium and those with adenomyosis in terms of age, parity, presence of abnormal uterine bleeding (AUB), and menopausal status. In dual measurements, 9 patients in the normal-myometrium group had concomitant leiomyoma, while, in the adenomyosis group, 3 patients had leiomyoma and 1 patient had adenomyoma (Fig. 2). Demographic data are shown in Table 1.

Flow chart of the study design. 2D, 2-dimensional, G, group.
Demographic Data
Data are presented as median (minimum–maximum).
The Emean values of US elastography ranged from 1.87 to 139 kPa. When the elastography measurement values in Emedian were compared among the histologic diagnosis groups, significant differences were noted among the adenomyosis, myoma, and normal-myometrium groups (p < 0.01). The SWE measurement values of the adenomyosis and leiomyoma groups were significantly higher than those of the normal-myometrium group. There was no significant difference between the adenomyosis and leiomyoma groups in terms of mean SWE values (Table 2).
Mean Shear-Wave Elastography of Normal Myometrium (G1), Adenomyosis (G2), and Leiomyoma (G3)
G1–G2, p < 0.01; G1–G3, p = 0.038; G2–G3, p = 0.25.
Statistical insignificance.
G, group; kPa, kiloPascals.
According to the histopathology results, the ROC analysis of the elastography Emean value could be used to distinguish between normal myometrium and adenomyosis with a 92% success rate, a 10.9% cutoff value, 93.1% sensitivity, and 82.1% specificity (Fig. 3).

Area under the receiver operating characteristic curve graph of 0.920 (p < 0.01; cutoff: 10.9; 95% confidence interval: 77.2−99.2). AUC, area under the curve.
The correlations among elastography measurements and age, parity, and AUB was investigated. Although no correlations were found among SWE, age, and AUB, a positive significant correlation was found between SWE and parity (p = 0.015).
Discussion
This study compared the SWE measurement values of patients with adenomyosis, leiomyoma, and normal myometrium. The results indicated that the mean SWE value for adenomyosis was significantly higher than that for normal myometrium. Although not statistically significant, the mean value for adenomyosis was higher than that for myoma. Adenomyosis can be differentiated from normal myometrium by using SWE during diagnosis because of the high sensitivity and specificity of this method. However, elastography could not distinguish between adenomyosis and fibroids successfully.
Transvaginal US (TVUS) and MRI are most commonly used for diagnosing uterine pathologies, such as adenomyosis. TVUS is superior to MRI because TVUS is noninvasive, easily tolerated, inexpensive, and easily accessible, making it the first-choice diagnostic tool. Moreover, a recent meta-analysis revealed that the sensitivity of MRI and TVUS for diagnosing adenomyosis was 78% similarly, whereas their specificities were 88% and 78%, respectively. 9
The diagnostic accuracy of conventional US for adenomyosis depends on the operator's expertise and the US image characteristics of the myometrium. The literature indicates that there is a wide range of sensitivity and specificity for diagnosing adenomyosis using US in the range of 80%–90% and 60%–80%, respectively. 10
Among the diagnostic criteria for US-based adenomyosis, image characteristics, such as myometrial echo heterogeneity, offer high sensitivity (80.8%) but moderate specificity (61.4%), whereas endometrial echogenic linear lines have a high specificity (95.5%) and an unacceptably low sensitivity (30.8%). In addition, globular growth and a disproportionate uterine wall enable only moderate levels of sensitivity and specificity (70%). 7 However, a small number of women presenting with early stage adenomyosis have typical US characteristics for adenomyosis. In those cases, conventional US may indicate a normal uterine appearance or an only slightly enlarged uterus.
Elastography integrated with ultrasonic technology can be used to measure the stiffness of tissues. SE and SWE are the commonly used elastography methods. In SE, external pressure is applied to the target organ, resulting in deformation, which is defined as strain in the tissue. Using specific software, tissue deformation can be visualized in the form of a color variation on US. The stiffness of the tissue is observed on a red–blue scale, with red indicating the softest regions, green indicating regions of moderate stiffness, and blue indicating the stiffest regions. Stiffness of a specific tissue must be compared with that of the surrounding tissue to create a color change. In SE, evaluations can be qualitative and semiquantitative. In the qualitative evaluation, colored maps are obtained that represent the degrees of stiffness of the lesions. Different scoring systems have been developed for objective evaluation of these maps. In the semiquantitative method, evaluation is performed by calculating the strain ratio, which is determined by dividing the strain value of a reference point around the lesion to the strain value of the lesion itself.
SWE is a sonoelastography method that measures tissue elasticity without the need for external pressure. The elasticity of tissue is expressed in kPa or in velocity (meter per second [m/s]). Lesion stiffness can be measured by the velocity of the wave obtained from the tissue in the form of objective quantitative data. 11 However, the most common elastographic technique found in the literature to differentiate between uterine pathologies was SE.12,13
In a study that used SE elastography and performed histologic and MRI confirmation of the diagnoses in 69 patients, Stoelinga et al. described the differences in the color patterns for myoma and adenomyosis. 14 These researchers reported that elastography was compatible with MRI and histology for diagnosing myoma and adenomyosis. However, the researchers only included 7 patients with pathologically confirmed adenomyosis, which was a major limitation in their study. 14
In a study by Liu et al., tissue stiffness was measured using SE in patients with adenomyosis and myoma and a control group. 15 Reportedly, the highest tissue stiffness was noted in the patients with adenomyosis. However, in that study, 82% of the patients were diagnosed based on TVUS without histologic or MRI confirmation. 15 However, it is not feasible to compare these studies, given that both qualitative and semiquantitative measures were used to evaluate the results. So far, no standardized measurement has been established for these techniques. However, the results from most of these studies indicate that SE could distinguish myoma from adenomyosis and normal myometrium; this is not consistent with the results of studies on SWE, including the current study.
Some studies, such as one by Hobson et al., report that adenomyosis has softer regions than normal myometrium. 16 Depending on the amount of pressure applied to the area being examined by the sonographer, a bias may occur during the examination when pressure is applied on the SE probe. Theoretically, SWE provides more-accurate results than SE because SWE records the expansion objectively and quantitatively after stimulation without the need to apply pressure on the probe. 16
In a study focusing on SWE, Acar et al. performed histologic analysis for a definitive diagnosis and found that tissue stiffness was higher in patients with adenomyosis than in a control group. 17 In another study, Zhang et al. used MRI for diagnosing adenomyosis and reported that the SW velocity measurements of adenomyosis and myoma groups were higher than that of the control group. 18
In a 2022 study involving transvaginal SWE, diagnoses were histologically confirmed using tissue biopsies; the results showed that the mean SWE value for adenomyosis was significantly higher than the value of normal myometrium. 19 This enabled a better differentiation of adenomyosis from normal myometrium. 19 In the current study, the mean SWE value for adenomyosis was significantly higher than that of normal myometrium, which was consistent with the studies using SWE. In addition, studies that also incorporated histology results have higher significance, as the definitive diagnosis of adenomyosis was confirmed histopathologically.
In the current study, the success of SWE in differentiating between normal myometrium and adenomyosis was 92.0%, while SWE also had a sensitivity of 93.1% and a specificity of 82.1%.
Pongpunprut et al. showed that SWE can be useful for diagnosing adenomyosis with sensitivity and specificity of up to 80% each. 19 Acar et al. found that, in the diagnosis of adenomyosis, the sensitivity and specificity of ultrasound SWE to be 89.7% and 92.9%, respectively. 17
The results obtained in the current study were consistent with those reported by Acar et al. 17 Adding elastography to other US diagnostic criteria, such as the MUSA criteria, will increase sensitivity.
Adenomyosis can be diagnosed differentially from normal myometrium by SWE because it has high sensitivity and specificity. However, in the current study, elastography had a slim success rate for differentiating the patients with adenomyosis from patients with fibroids. Adenomyosis stiffness measured with SWE was higher than that of the normal myometrium. When the adenomyosis and fibroid groups were compared, adenomyosis had higher stiffness than myoma did, but the difference was not statistically significant. These findings are consistent with those that Pongpunprut et al. 19 These results also indicated increased stiffness of uterine tissue in women with adenomyosis. Adenomyosis is the abnormal growth of glandular tissue into the myometrium. Although glandular tissue itself is soft, lesions in the myometrium, just like their endometrial counterparts, are in a cycle of tissue damage and repair. However, smooth-muscle transdifferentiation and smooth-muscle metaplasia cause the lesions to become increasingly fibrotic. This fibroticization also causes stiffness in the tissue.20–22
In the current study, a positive and significant correlation was demonstrated between elastography and parity. However, according to Liu et al., parity and elastography are not correlated at all. 15 The presence of tearing and fibrosis in the outer myometrium during labor contractions, and the elevated risk of adenomyosis as parity increases, may explain the correlation between parity and uterine stiffness.23,24
Most studies of elastography for diagnosing uterine pathologies used transvaginal elastosonography (TVESG). Acoustic stimuli can only reach up to 3 cm into the tissue when using the transvaginal US probe. Therefore, the pathologic lesion should be located in the area from the middle to the lower part of the uterus.25,26
Adenomyosis is a condition that, by nature, enlarges the uterus, and a depth of 3 cm is a limited study area for adenomyosis. The main limitation of previous studies is that the maximum depth at which the stiffness values of TVESG can be evaluated is 3 cm. In addition, this technique is not suitable for women who are contraindicated for transvaginal examination.17,19
Transabdominal SWE was used in the current study, which made it possible to measure up to 8-cm deep by using the convex probe. 27 This enabled examination of the uterus thoroughly from the fundus to the isthmus. However, this technique has certain technical limitations, including that the depth of the uterus increases due to its position, such as flexion–version, and that some patients have high abdominal-fat levels. Another limitation of the current study was the small sample size and the single-center nature. In contrast, the strength of this study was the pathology-based diagnoses.
Conclusions
This study showed that the degree of tissue stiffness in adenomyosis is significantly higher, compared with that of normal myometrium, as determined by using transabdominal SWE. This technique can be used to differentiate between adenomyosis and normal myometrium. However, the presence of leiomyomas may reduce the diagnostic accuracy of this method. Including elastography in the current US-based diagnostic criteria for adenomyosis will increase the success of distinguishing adenomyosis from other uterine pathologies.
Nonetheless, further multicenter studies with large populations and standardized techniques are warranted to identify the potential of SWE for diagnosing uterine pathologies.
Footnotes
Authors' Contributions
This study was compiled from the thesis of Dr. Kaya Narçiçeği, who designed the project with Drs. Aslan and Artaş; planned it with Drs. Yavuzkir, Yurt, and Özercan; conducted data analysis with Dr. Eryeşil; and wrote the article with Dr. Aslan.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.