
Abstract
Abstract
Objective:
The goal of this research was to determine the efficacy of fractionated carbon dioxide (CO2) laser therapy for reducing symptoms of vulvar lichen sclerosus (LS).
Materials and Methods:
This was a prospective case series. The study participants were 23 women with active vulvar LS, confirmed via biopsy, who were abstaining from topical and systemic treatments for at least 4 weeks before enrollment. Subjects received 3–5 treatments with the CO2 laser, based on symptom improvements. The primary endpoint was a reduction by >50%, as shown by a composite examination-based and symptom-based score at 6 months post-treatment. A secondary endpoint was changes in the Vulvar Quality of Life Questionnaire and patient-supplied Patient Global Impression of Improvement (PGI) scores. A t-test was used to contrast pre-treatment and post-treatment changes in symptoms
Results:
From 2015 to 2020, 23 women participated in the study. The primary endpoint of >50% reduction in the composite symptom score was not significant; p = 0.08, although a reduction was significant at that time point; p = < 0.01. At 12 months a >50% reduction was significant; p = 0.03. Secondary outcomes were remarkable for significant reductions in symptoms that did not meet the >50% threshold at 6 and at 12 months. Mean satisfaction was 2.47 ± 0.61 on a 3-point scale and significantly positive PGI scores through the post-treatment follow-up time point.
Conclusions:
Exploration of fractionated CO
Introduction
Lichen Sclerosus (LS) is a chronic, progressive inflammatory skin condition affecting both men and women. The etiology of this disorder is not clear but it appears to be an autoimmune condition. The mean age of onset is 45. 1 Genital LS symptoms include pruritus and dyspareunia. Skin changes can include thin paperlike skin, introital stenosis, labial resorption and fusion, epithelial erosions, and fissures. These symptoms can contribute to pain with or without sexual activity.1,2 Histologic changes associated with LS include epidermal atrophy and dermal hyalinization. 3 Rarely, progression to squamous-cell carcinoma may develop, with a reported incidence of 0.3%–4.9%. 1
There is no known cure for LS and lifelong treatment is anticipated in most cases. Conservative treatment approaches for LS include avoidance of irritants (such as urine, certain soaps, or detergents), use of moisturizers and emollients, and treating vulvar skin infections. 1 High-potency corticosteroids comprise the “gold standard” of care. High-potency corticosteroids are effective for providing symptomatic relief in upward of 70%–96% of cases.4,5
Although treatment with topical corticosteroids is effective, these medications can have local and systemic adverse effects, including dermal thinning, skin atrophy, superimposed infections, rebound dermatitis, adrenal insufficiency, and difficulty with long-term compliance. 6 Although these side-effects are uncommon, interest in alternative interventions exists. Fractionated carbon dioxide (CO2) laser use has been proposed to manage vulvar LS. This type of laser has a wavelength of 10,600 nm, inducing a superficial microablative effect in soft tissues, as well as a pulsed beam, which protects tissues from possible damage due to overheating. The laser beam is delivered to the tissue fractionally, creating small spots (150–200 μm) in alternating parts of tissue. 7
CO2 laser therapy has shown promise for treating LS.7–9 The theoretical benefits of CO2 laser treatment include potentials to stimulate protein synthesis, accelerate tissue reconstruction, and decrease lichenification. Furthermore, the clinical manifestations of LS, such as intense vulvar pruritus and burning, appeared to be reduced. A limitation of most prior studies—in which many have achieved these positive symptom reductions—was a lack of blinding or placebo control. However, there are 2 published randomized controlled trials (RCTs) that have examined CO2 laser for treatment LS.10,11
A 2021 study by Mitchell et al. 10 examined the use of fractionated CO2 laser as a monotherapy treatment for vulvar LS in a randomized, blinded, sham-controlled setting. The primary endpoint of that study was a 40% reduction in histologic signs of vulvar LS in patients undergoing 5 treatments at 4-week intervals with a follow-up of 8 weeks post-treatment. A secondary endpoint was a change in a composite score of physician/patient graded severity of LS. In the study's treatment arm, the power of the CO2 laser varied from 18 W to 26 W, the dwell time varied from 800 to 1000 μsecs, and the spacing of the laser varied from 1000 μm to 1200 μm. Both primary and secondary endpoints were nonsignificant in this study. However, the authors stated that it was powered to examine the primary endpoint, but did not mention powering the study to the secondary endpoint of symptom-based scores. Furthermore, these patients were only followed for 8 weeks post-treatment. 10
A 2021 study by Burkett et al. 11 was an unblinded RCT of clobetasol versus CO2 laser use with stratification by prior clobetasol use. There was no variation in laser parameters in this study with a CO2 laser power of 30 W, a dwell time of 1000 μsecs, and a spacing of 1000 μm within the CO2 laser arm. The primary outcome was a change in a composite symptom-based score at 6 months, and a secondary outcome included changes in a visual analogue scale pain score, a Vulvovaginal Symptoms Questionnaire, and a Patient Global Impression of Improvement (PGI) score. Subjects were followed for 6 months. There was greater improvement in the composite symptom-based score in the laser arm, compared to the steroid arm. Although subjects were significantly more satisfied with laser treatment, compared to steroid treatment, but when stratified for previous steroid use, a significant change in a composite symptom-based score was only seen in patients previously exposed to clobetasol. 11
Although similar, these 2 studies had several differences including using different scoring systems and laser settings. Both studies used multiple providers to perform examination-based testing, a concern given that interobserver reliability of this kind of assessment is variable for LS. 12 The current study—a prospective case series in which patient symptoms and physical examination findings were examined by 1 provider and in which laser settings were uniform—was conducted to delve further into the effects of CO2 laser treatment.
Materials and Methods
Women were recruited from a clinic of The Christ Hospital, Cincinnati, Ohio, USA, from 2015 to 2020. Inclusion criteria included females, 18 years or older with biopsy-proven LS, who had not had procedures performed in the perineal or vulvar areas in the past 6 months before treatment and who had not used topical corticosteroids in the preceding 4 weeks before enrollment. Exclusion criteria were current genital infection (e.g., herpes genitalis, vulvovaginal candidiasis, bacterial vaginosis, or trichomoniasis) along with a history of any prior herpes genitalis diagnoses. Further exclusion criteria included evidence of active vaginal disease (e.g., ulcerations or abnormal erythema in association with tissues inside of the hymen) and current use of photosensitive medications (such as quinolones, tetracyclines, antimalarial medications, parenteral chemotherapy, isotretinoin, and tricyclic antidepressants).
The primary study outcome was a 50% reduction in signs and symptoms of LS at 6 months after treatment with a CO2 laser; each patient was evaluated via a composite examination-based and symptom-based score (Supplementary Appendix 1; supplementary data are available online at: www.liebertonline/GYN). Secondary outcomes were validated with tools used to determine the effects of disease on a patient's quality of life (QoL). One secondary outcome was the differential effect of treatment with CO2 laser on general health-related QoL using the Vulvar Quality of Life Questionnaire (Supplementary Appendix 2). Another secondary outcome was the differential rate of treatment satisfaction among subjects, evaluated via the the Patient Global Impression of Improvement (PGI) survey (Supplementary Appendix 3) and an overall satisfaction questionnaire (Supplementary Appendix SA4).
Subjects underwent the primary outcome assessment and completed the Vulvar Quality of Life survey before the first treatment; with each laser treatment; and post-treatment at 6 weeks, 3 months, 6 months, and 12 months. Subjects completed the PGI survey before the second laser treatment through 12 months of follow-up. To assess discomfort with the treatment itself, patients also completed an Iowa Pain Scale after each laser treatment (Supplementary Appendix 5). Finally, patients completed an overall satisfaction rating at 6 weeks post-treatment.
The subjects completed an informed consent form before any study procedures were performed. Subjects first presented to the study clinic for a screening visit to determine eligibility and enrollment. Surveys were performed as above. Treatment was performed with a SmartXide 2 -V 2 LR CO2 (MonaLisa Touch®) laser with the power set at 26 W, the dwell time set at 800 μsecs, a dot spacing of 800 μm, and a smartstack of 1 for all treatments. The procedure was performed in the outpatient clinic. A laser treatment cycle included 3–5 sessions 4- 6 weeks apart (± 1 week). Before treatment, Emla cream was applied to the affected vulvar areas and left on for 5 minutes to induce analgesia. The cream was then wiped off, and the area then treated with 1 pass of the laser.
Each subject received a minimum of 3 laser treatments; any patient who still had symptoms received a fourth or fifth treatment. The subjects returned to the clinical site for follow-up evaluations at 6 weeks, 3 months, 6 months, and 12 months after the last laser treatment. Study outcomes were analyzed with JMP® pro 15 software. Two-sample paired t-tests for means were used to show changes in questionnaire scores with scores at specific time points contrasted with the pretreatment scores.
This research had been approved by the institutional review board (IRB) of The Christ Hospital IRB number: 15-27; IRB approved on July 14, 2015). Subjects were not charged for participation in this study as a grant from The Foundation for Female Health Awareness had supported this work.
Results
A total of 23 women were enrolled in the trial from June 2016 through January 2020. The mean age of the subjects was 61 ± 9.6 years. The patients' mean body mass index was 30.82 ± 8.1. All subjects were white. The number of treatments varied, as noted above, with 4, 4, and 15 subjects undergoing 3, 4, and 5 treatments, respectively, with the CO2 laser. Each subject was to receive a maximum of 3 laser treatments; patients who were still symptomatic but improved were given a fourth or a fourth and a fifth treatment. Compliance with follow-up decreased with time, decreasing from 19 subjects presenting to a 6-week follow-up to 9 presenting to a 12-month follow-up. See Figure 1 for the study's flow diagram.
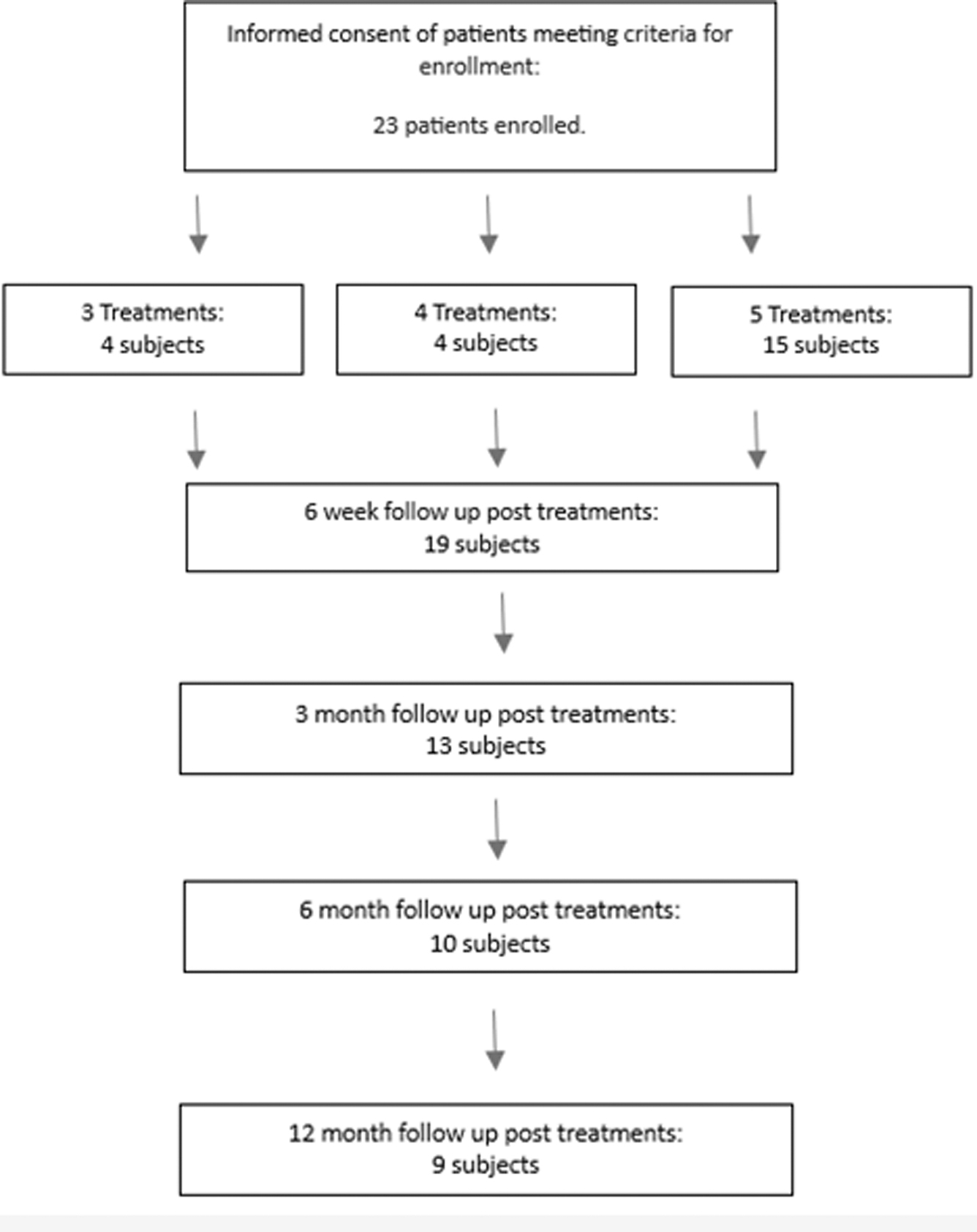
Enrollment, treatment, and follow-up flow diagram for the study.
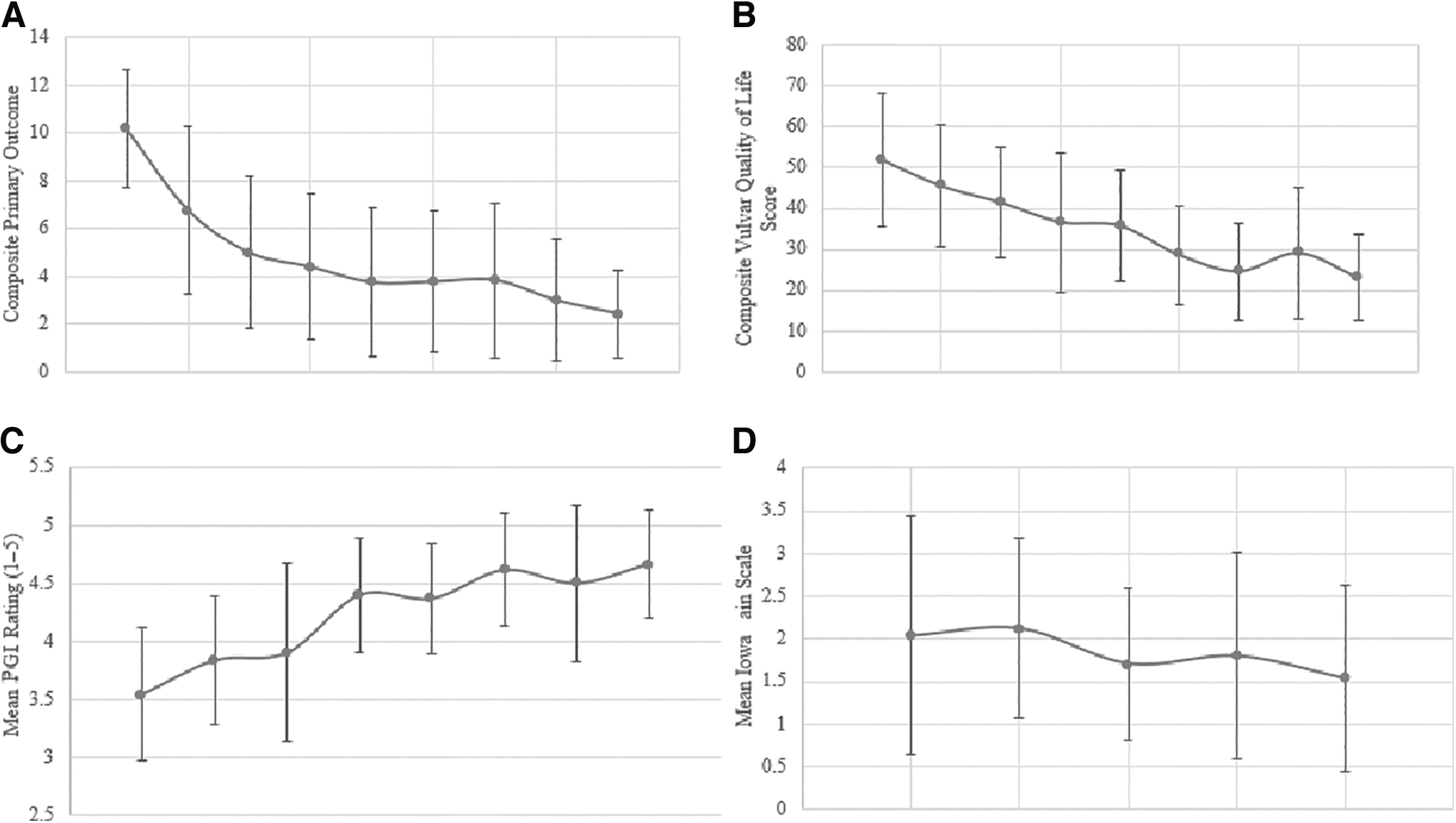
Results of the composite primary outcome, Vulvar Quality of Life, PGI, and Iowa Pain Scale questionnaire responses are shown in Figure 2. As previously stated, the primary outcome was a >50% reduction in pain at 6 months. A 2-sample paired t-test for means was used to display this reduction in symptoms. A 2-sample paired t-test for means at 6 months post treatment was significant with a reduction from a pretreatment symptom score of 10.2 ± 2.5 to a 12-month post-treatment score of 2.4 ± 1.8 (p < 0.001). A 2-sample paired t-test for means at 6 months for >50% reduction in composite symptom score was not significant with p = 0.08. However, a 2-sample paired t-test for means at 12 months for >50% reduction was significant with p = 0.03.
Results of the
Secondary outcomes were also examined. For the Vulvar Quality of Life questionnaire, a higher score indicated increased vulvar symptoms with a negative impact on QoL. A decrease in these symptoms was seen in patients, with a 2-sample paired t-test for means at 6 months post-treatment being significant at p = < 0.01; however, a >50% reduction in symptoms was not shown, p = 0.31.
Regarding subjective improvement, Mean satisfaction was 2.47 ± 0.61 on the 3-point scale shown in Supplementary Appendix 4 indicative of “moderate” to “quite a bit” on the improvement scale. Of note, no subject in this study had a lower than moderate—or 2—on satisfaction at 6 weeks post-treatment. PGI scores were significant with a t-test of <0.01 at 6 and at 12 weeks (Fig. 3).
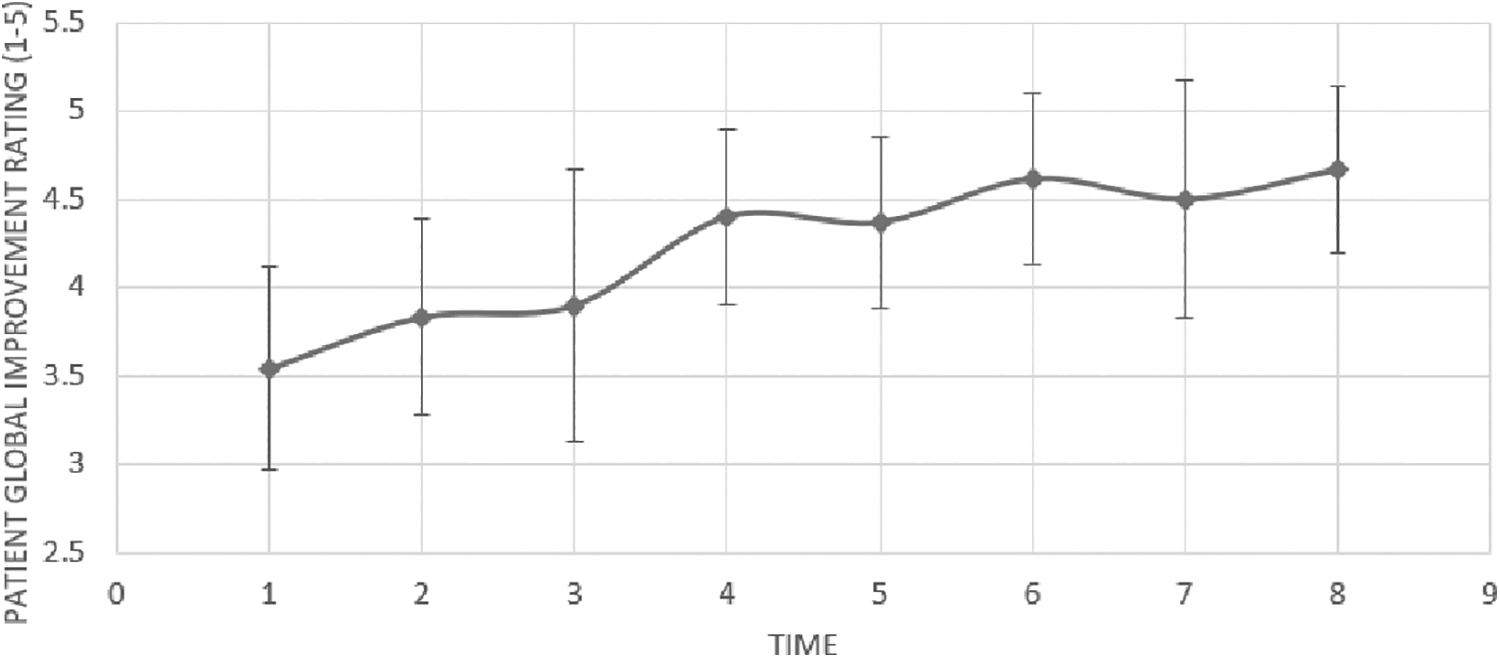
Mean Patient Global Impression of Improvement scores over time.
Adverse events included 1 subject who had a 1-cm hematoma at her 6-week post-treatment visit (the hematoma resolved by her 3-month visit) and 1 subject who withdrew from the study after her first laser treatment because she could undergo further treatments due to work constraints.
Discussion
Improvements in examination and symptom-based scores, positive PGI responses, and high overall satisfaction scores occurred in this study. This study was different from the study by Mitchell et al., 10 because symptom-based scoring systems and questionnaires defined treatment success instead of histologic evaluations. In this way, the current study supported many of the findings in the study by Burkett et al. 11 by inducing benefit (symptom reduction) through vulvar laser use to treat LS. This difference in defining treatment success did not lessen the impact of histologic findings but did examine outcomes that could aid in patient counseling on the risks and benefits of vulvar laser treatment for LS. Data extending to 12 months post-treatment comprise a factor that added to the fund of knowledge on patient counseling. Figures 2 and 3 the symptoms associated with LS decreased steadily to the 12-month time point. The follow-up of only to 8 weeks post-treatment in the prior study was likely a reason for these differing data. The current study followed patients for 12 months' post-treatment, with continued improvements seen during this time, which was a significantly longer follow-up time, compared to the prior studies.10,11
The lasers used in the studies were also different with differing protocols used. The current study had set the laser power at 26 W—again similar to what Burkett et al. did 11 —whereas Mitchell et al., 10 only used that power at the fifth treatment. Spacing varied in Mitchell et al.'s study 10 as well as the current study's spacing and dwell time correlating with the closest and longest spaces and times from the prior study. 10 Perhaps these consistent and elevated parameters were needed for clinical effectiveness.
Strengths of this study included the long-term follow-up as well as the consistent and reproducible parameters aiding repetition and clinical success. Use of validated questionnaires was another strength as was no pretreatment and or cotreatment with clobetasol.
This study did have several limitations. One limitation was the study being a prospective case series with no nontreatment/placebo arm rather than being an RCT— a concern given the high placebo rates seen by Mitchell et al. 10 and Burkett et al. 11 All participants were white, thus the sample was homogenous which could have skewed the data. There was also a potential bias because the study was conducted and evaluated by the same practitioner. Moreover, the high dropout rate (with only 9 of 19 patients following up to the 12-month time-point) also limited interpretation of these study results. These limitations called the effectiveness shown in the current study into question, compared to the academic rigor displayed by prior studies.
Conclusions
The universal benefit seen in patient satisfaction and improvement in validated questionnaire response data is difficult to ignore. It is in the setting of this immensely positive satisfaction and symptom data that consideration should again be given to continuing research on the use of the CO2 laser, perhaps with an eye toward using this higher power and prolonged follow-up protocols. Overall, patient satisfaction and QoL should remain paramount concerns when treating vulvar LS, which should point to the use of CO2 laser to treat the condition.
Footnotes
Authors' Contributions
Both authors performed project administration and investigations, and wrote this article. Dr. Karram conceptualized the study and its methodology, acquired resources and funding, supervised the project, and validated its findings. Dr. Rothenberger curated the data.
Author Disclosure Statement
No financial conflicts of interest exist for Dr. Rothenberger. Dr. Karram is a speaker and consultant for InMode, Irvine, CA, USA.
Funding Information
This research received funding via a grant from the Foundation for Female Health Awareness, West Chester, OH.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.