
Abstract
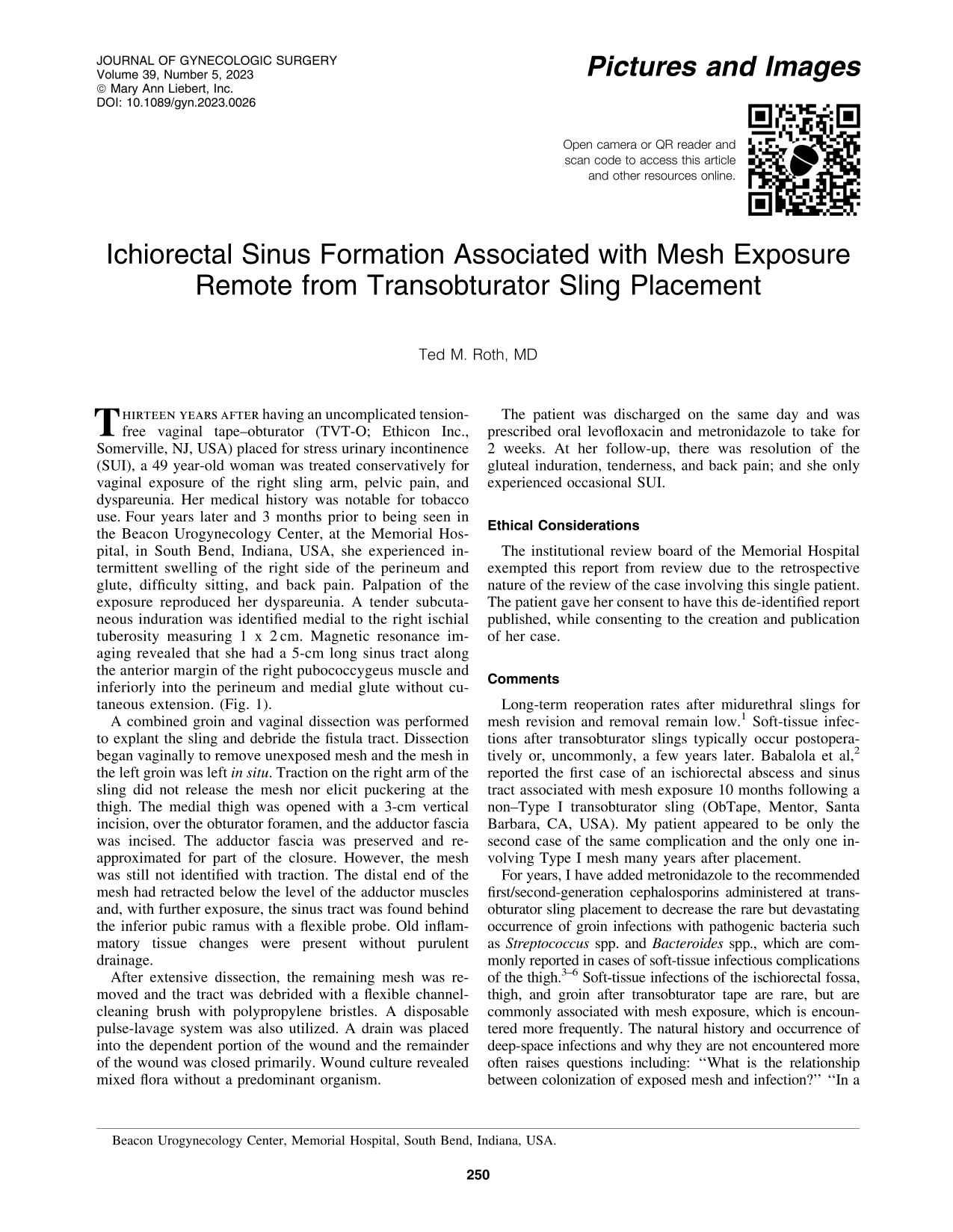
Thirteen years after having an uncomplicated tension-free vaginal tape–obturator (TVT-O; Ethicon Inc., Somerville, NJ, USA) placed for stress urinary incontinence (SUI), a 49 year-old woman was treated conservatively for vaginal exposure of the right sling arm, pelvic pain, and dyspareunia. Her medical history was notable for tobacco use. Four years later and 3 months prior to being seen in the Beacon Urogynecology Center, at the Memorial Hospital, in South Bend, Indiana, USA, she experienced intermittent swelling of the right side of the perineum and glute, difficulty sitting, and back pain. Palpation of the exposure reproduced her dyspareunia. A tender subcutaneous induration was identified medial to the right ischial tuberosity measuring 1 x 2 cm. Magnetic resonance imaging revealed that she had a 5-cm long sinus tract along the anterior margin of the right pubococcygeus muscle and inferiorly into the perineum and medial glute without cutaneous extension. (Fig. 1).

Coronal magnetic resonance image of the patient's pelvis. The triangle indicates the rectum. The arrow shows the sinus tract that extends posteroinferiorly to the right gluteus maximus muscles.
A combined groin and vaginal dissection was performed to explant the sling and debride the fistula tract. Dissection began vaginally to remove unexposed mesh and the mesh in the left groin was left in situ. Traction on the right arm of the sling did not release the mesh nor elicit puckering at the thigh. The medial thigh was opened with a 3-cm vertical incision, over the obturator foramen, and the adductor fascia was incised. The adductor fascia was preserved and reapproximated for part of the closure. However, the mesh was still not identified with traction. The distal end of the mesh had retracted below the level of the adductor muscles and, with further exposure, the sinus tract was found behind the inferior pubic ramus with a flexible probe. Old inflammatory tissue changes were present without purulent drainage.
After extensive dissection, the remaining mesh was removed and the tract was debrided with a flexible channel-cleaning brush with polypropylene bristles. A disposable pulse-lavage system was also utilized. A drain was placed into the dependent portion of the wound and the remainder of the wound was closed primarily. Wound culture revealed mixed flora without a predominant organism.
The patient was discharged on the same day and was prescribed oral levofloxacin and metronidazole to take for 2 weeks. At her follow-up, there was resolution of the gluteal induration, tenderness, and back pain; and she only experienced occasional SUI.
Ethical Considerations
The institutional review board of the Memorial Hospital exempted this report from review due to the retrospective nature of the review of the case involving this single patient. The patient gave her consent to have this de-identified report published, while consenting to the creation and publication of her case.
Comments
Long-term reoperation rates after midurethral slings for mesh revision and removal remain low. 1 Soft-tissue infections after transobturator slings typically occur postoperatively or, uncommonly, a few years later. Babalola et al, 2 reported the first case of an ischiorectal abscess and sinus tract associated with mesh exposure 10 months following a non–Type I transobturator sling (ObTape, Mentor, Santa Barbara, CA, USA). My patient appeared to be only the second case of the same complication and the only one involving Type I mesh many years after placement.
For years, I have added metronidazole to the recommended first/second-generation cephalosporins administered at transobturator sling placement to decrease the rare but devastating occurrence of groin infections with pathogenic bacteria such as Streptococcus spp. and Bacteroides spp., which are commonly reported in cases of soft-tissue infectious complications of the thigh.3–6 Soft-tissue infections of the ischiorectal fossa, thigh, and groin after transobturator tape are rare, but are commonly associated with mesh exposure, which is encountered more frequently. The natural history and occurrence of deep-space infections and why they are not encountered more often raises questions including: “What is the relationship between colonization of exposed mesh and infection?” “In a long-enough timeline does colonization uniformly lead to infection?” “Does bacterial virulence play a deciding factor?” 6
In my patient, the location and the time course of the exposure as well as weak bacterial virulence may have led to the migration of the distal end of the mesh arm favoring the development of the ischiorectal fossa sinus tract (as well as her nonacute presentation) rather than the more-commonly reported groin abscess.
Footnotes
Author's Contribution
Dr. Roth cared for the patient and wrote this article.
Author Disclosure Statement
No competing financial conflicts of interest exist. Note that the author is a preceptor for Ethicon and is a testifying expert witness in that company's mesh litigation.
Funding Information
No funding was received for the production of this article.