
Abstract
Objective:
The aim of this research was to evaluate intraoperative visual detection of endometriosis compared to final histopathologic diagnosis based on lesion type.
Materials and Methods:
This prospective clinical study at a tertiary-care, academic medical center involved 77 patients who had surgery by high-volume endometriosis surgeons for suspected endometriosis. Pelvic peritonectomy was performed with documentation of visual presence or absence of endometriosis and lesion type. Powder burn lesions were defined as typical lesions. White scarring, clear vesicles, red flame, and peritoneal pockets were defined as atypical lesions.
Results:
Of 1069 peritoneal specimens, there was visual detection of endometriosis in 352 (32.93%). Endometriosis was confirmed on histopathologic evaluation of: powder-burn, 65.8%; white scarring, 51.6%; clear vesicles, 45.7%; red-flame, 39.1%; and peritoneal pockets, 28.9% (p = 0.003). Additionally, 11.3% of specimens with no visible endometriosis demonstrated a positive histopathologic diagnosis. Overall sensitivity was 68.36%; specificity was 78.15%; positive predictive value (PPV) was 49.72%; and negative predictive value was 88.66%. All lesions had high specificity (powder-burn, 96.20%; white scarring, 91.34%; clear vesicles; 92.54%; red-flame, 97.84%; and peritoneal pockets; 95.91%). PPV depended on lesion type (powder-burn, 65.75%; white scarring, 51.61 %; clear vesicles, 45.74%; red-flame, 39.13% peritoneal pockets, 28.95%).
Conclusions:
Visual detection of endometriosis during surgical evaluation is not reliable. The potential for atypical-lesion appearance and disease not macroscopically visible suggests a role for complete pelvic peritonectomy. (J GYNECOL SURG 39:235)
Introduction
Endometriosis—defined as the presence of endometrial-like glands and stroma outside of the uterus—is estimated to affect ∼10% of reproductive-age women. The presentation of endometriosis can be highly variable, but common symptoms include dysmenorrhea or pelvic pain, infertility, or the presence of an adnexal mass. A clinician may suspect a diagnosis of endometriosis based on the patient's symptoms, examination, or imaging findings, but the “gold standard” diagnosis requires histopathologic evaluation of an excised specimen, typically obtained via laparoscopy. 1
Superficial peritoneal endometriosis lesions can vary considerably in appearance, creating challenges to accurate visual detection during surgery. 2 The classic endometriosis lesion is described as a black, dark-brown, or bluish “powder-burn” lesion, while the remaining lesion types are considered atypical and include red-flame, clear vesicles, white scarring, and peritoneal pockets. 3 Red and white lesions, in particular, can have highly variable appearances and may be difficult to distinguish from normal peritoneum. 4 Additionally, normal-appearing peritoneum during surgery can ultimately result in pathologic findings consistent with endometriosis. 5
A prospective study by Walter et al. demonstrated a positive predictive value (PPV) of 45% for accurate visual detection of endometriosis; thus, lesions may go undetected by the surgeon's eye without proper histopathologic evaluation. 5 The purpose of this study was to evaluate visual diagnosis of superficial endometriosis during laparoscopy, compared to final histopathologic diagnosis based on lesion type. By better understanding the polymorphic appearance of endometriosis, it is possible to improve the diagnostic potential of visualization to facilitate adequate excision.
Materials and Methods
This was a prospective clinical study of female patients who underwent laparoscopic pelvic peritonectomy for suspected endometriosis at the Mayo Clinic in Arizona between November 2020 and August 2021. All surgeries were performed by high-volume subspecialists with expertise in endometriosis. Approval was obtained from the Mayo Clinic's institutional review board (approval #: 18-010875). Inclusion criteria included female patient >18 years old with symptoms suspicious for endometriosis and ability to provide informed consent. Exclusion criteria included evidence of deeply infiltrating endometriosis (DIE) on preoperative deep pelvic ultrasound or identified intraoperatively. Demographic information was collected. including age, race, body mass index (BMI), and parity. Patient-reported symptoms were also documented as well as if a patient had prior histopathologic diagnosis of endometriosis.
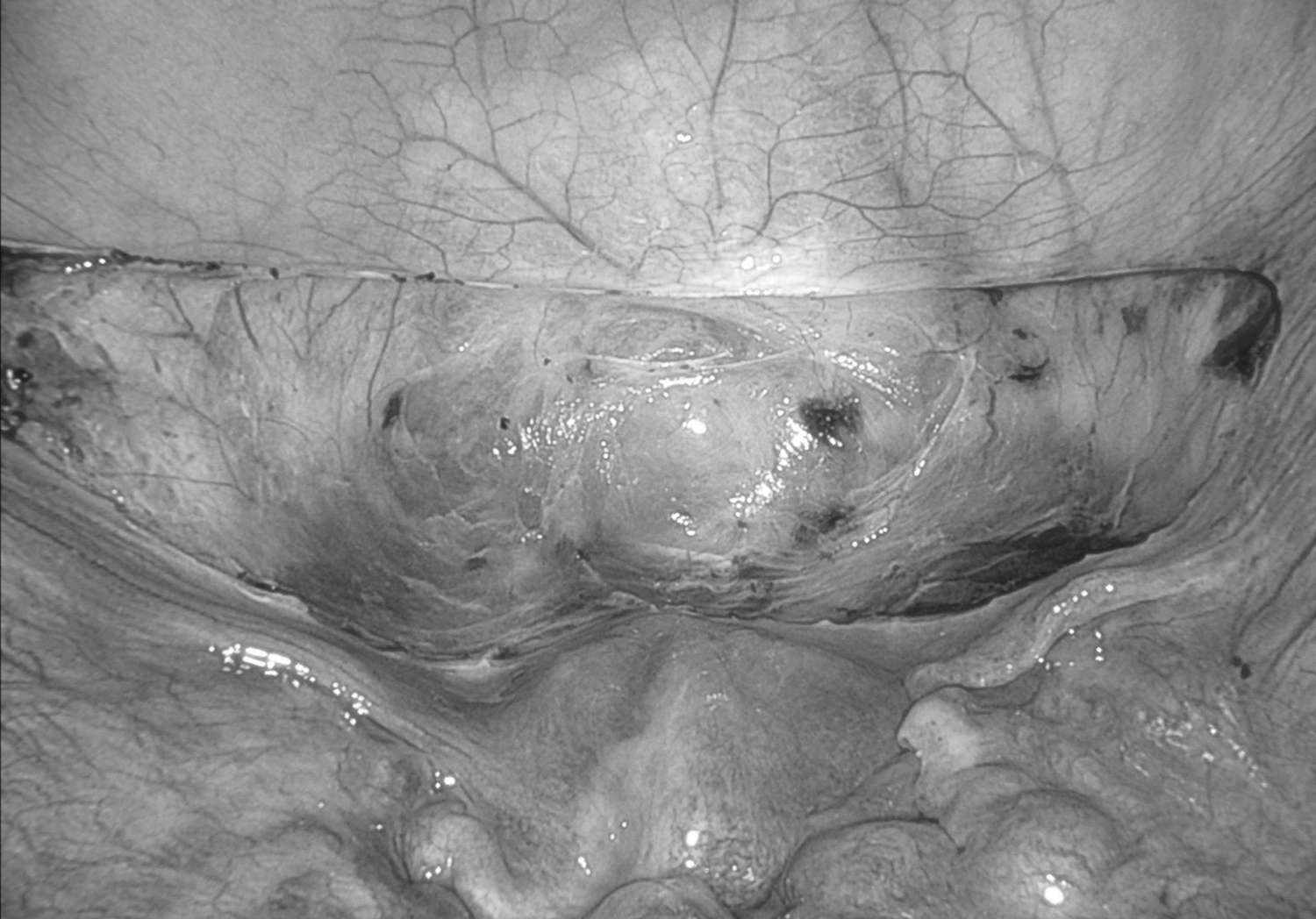
During surgery, a laparoscopic survey of the pelvis was performed to identify lesions suspicious for endometriosis. Data were collected regarding the anatomical sites and the types of lesions seen. Anatomical sites included the left and right pelvic sidewalls, left and right uterosacral ligaments, posterior cul-de-sac, and bladder (Figs. 1 and 2). The presence or absence of visual endometriosis was documented and, if present, each lesion was classified as powder burn, white scarring, red-flame, clear vesicles, or peritoneal defect. A complete peritonectomy of each anatomical site was then performed (Figs. 3 and 4), including removal of normal-appearing peritoneum to evaluate for microscopic disease. The specimens were evaluated by pathology in the standard fashion to assess for presence of endometrial glands and stroma, and the pathologists were blind to the classification of the biopsy. The data collected intraoperatively regarding visual detection of endometriosis were compared to the final histopathologic diagnoses.
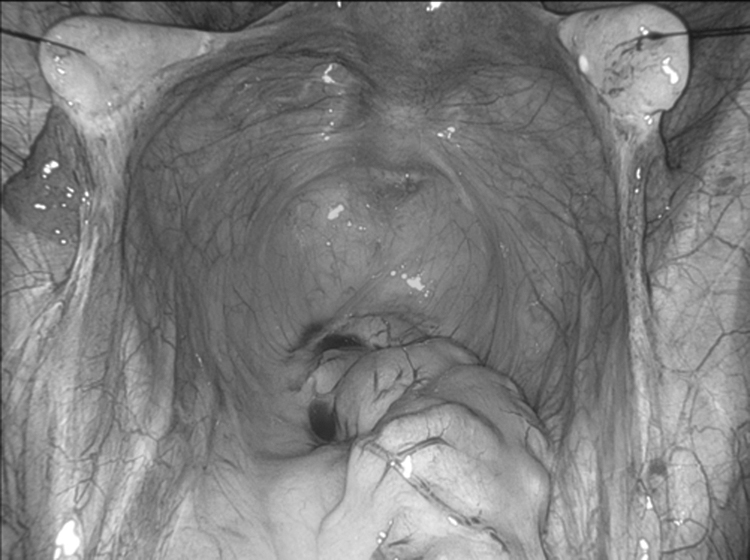
Anatomical sites evaluated for endometriosis include left and right pelvic sidewalls, left and right uterosacral ligaments, and posterior cul-de-sac.

Bladder peritoneum evaluated for endometriosis.

Appearance of left and right pelvic sidewalls, left and right uterosacral ligaments, and posterior cul-de-sac following peritonectomy.
Appearance of bladder following peritonectomy.
A sample size of 15 for each lesion type, for a total of 75, achieved 80% power to detect a prevalence rate of 20%. Descriptive statistics were used to summarize demographic data along with responses for visual and histologic diagnosis of endometriosis. Means, standard deviations, and ranges were used to summarize continuous variables, while counts and percentages were used for categorical data. Group comparison of final histopathologic diagnosis of endometriosis versus no endometriosis was compared for lesion type using a χ 2 test. Visual characteristics and histopathologic diagnoses were organized by sensitivity, specificity, PPV, and negative predictive value (NPV). Data were captured via REDCap [Research Electronic Data Capture]. A p-value <0.05 was considered statistically significant. Statistical analysis was performed, using R version 4.0.3.
Results
Ninety-three patients were enrolled in the study. Sixteen patients were excluded secondary to 1 patient with evidence of DIE on preoperative imaging, 12 patients with evidence of DIE intraoperatively, and 3 patients ultimately not undergoing complete peritonectomy. A total of 77 patients who underwent laparoscopic pelvic peritonectomy were included in the final analysis. The mean age was 30, and 26% of participants had prior confirmed histopathologic diagnoses of endometriosis (Table 1). Patient-reported symptoms included 84.4% with pelvic pain, 42.9% with dysmenorrhea, 29.9% with dyspareunia, 7.8% with dyschezia, 2.6% with dysuria, and 2.6% with infertility (Table 1). Additional patient demographics are in Table 1.
Patients' Demographics
yrs, years; SD, standard deviation, BMI, body mass index.
A total of 1066 peritoneal specimens underwent histopathologic evaluation. Visual endometriosis was reported for 352 specimens (32.93%). The final histopathologic diagnoses by lesion types is summarized in Table 2. Endometriosis was confirmed on histopathologic evaluation in 65.8% of powder-burn lesions, 51.6% of white-scarring lesions, 45.7% of clear vesicles, 39.1% of red-flame lesions, and 28.9% of peritoneal pockets (p = 0.003). White scarring was the most-common lesion type, comprising 36.6% of specimens with a final histopathologic diagnosis of endometriosis, while red-flame was the least-common lesion, comprising 5.1% of the sample. Powder-burn lesions comprised 27.4% of all specimens with a final histopathologic diagnosis of endometriosis. Additionally, 11.3% of specimens with no visible endometriosis had a positive histopathologic diagnosis of endometriosis.
Final histopathologic Diagnosis by Lesion Type (p = 0.003)
The sensitivity, specificity, PPV, and NPV by lesion type are summarized in Table 3. Overall, the sensitivity, specificity, PPV, and NPV for visual detection of endometriosis were 68.36%, 78.15%, 49.72%, and 88.66%, respectively. White scarring was the lesion type with the highest sensitivity at 44.14%, while the lowest sensitivity was for red-flame lesions at 10.0%. All lesion types had high specificity while their PPV varied depending on lesion type.
Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value by Lesion Type
PPV, positive predictive value; NPV, negative predictive value.
Discussion
This study evaluated intraoperative visual detection of endometriosis by lesion type, compared to the final histopathologic diagnoses. Despite new technologies and improvements in magnification of the laparoscope, identification of superficial peritoneal endometriosis remains a challenge.6,7 A systematic review performed by Wykes et al. found that a visually positive laparoscopy is of limited value for diagnosing endometriosis without histologic confirmation. 8 Lesions can vary in size, shape, and color, often leading to subtle changes in the peritoneum, and reliance on the surgeon's eye may lead to incomplete evaluation and misdiagnosis for endometriosis.
Prior studies have evaluated visual detection of endometriosis; however, the current study differed in that complete pelvic peritonectomy was performed, even in the setting of normal-appearing tissue. The overall NPV for visual detection of endometriosis in the current study was 88.66%. Stegmann et al. found a NPV of 88%. 2 This finding suggests that surgeons are fairly accurate in identifying tissue without disease based on visual inspection. However, in the current study, 11.3% of specimens with no visible endometriosis were found to have histopathologic disease; thus, normal peritoneum does not always equate to absence of disease.
Walter et al. previously found just 2 out of 380 biopsy specimens with microscopic endometriosis in visually normal peritoneum; these were random peritoneal biopsies. 5 The current authors propose that biopsy, as opposed to full peritonectomy, may result in sampling error and additional microscopic disease may be present on normal-appearing tissue that was not removed. Postoperative recurrence is thought to be due to incomplete resection of disease, and one or more negative biopsies cannot confirm the absence of endometriosis. 9 By performing a complete peritonectomy, the risk of incomplete excision is likely reduced.
Powder-burn lesions are considered typical or classic endometriosis lesions, while the remaining lesion types are considered atypical, including red-flame, clear vesicles, and white scarring areas of fibrosis. Powder-burn lesions had the highest PPV of all lesions types at 65.75%, indicating that surgeons have the most familiarity with identifying this lesion type. However, powder-burn comprised just 27.4% of confirmed endometriosis lesions. Thus the majority of endometriosis lesions were atypical in appearance. White scarring was the most-common lesion type, comprising 36.6%, while red-flame was the least-common at 5.1%. Stegmann et al. had similar findings with 28% of endometriosis lesions defined as black and the remainder representing atypical endometriosis lesions. 2 Stratton et al. also found that white lesions and mixed-color lesions were more likely to be confirmed endometriosis, compared to black lesions. 10 While surgeons may be well-equipped to identify the classic powder-burn lesion, it is important to realize that the majority of endometriosis does not have this appearance.
The overall PPV for visual detection of endometriosis was 49.72%, indicating that the surgeon's eye can identify endometriosis accurately about half of the time. Walter et al. had similar findings with a PPV of 45%. 5 With respect to specific lesion types, typical and atypical lesions have similar sensitivity, specificity, and PPV for accurate visual detection of endometriosis in the eye of endometriosis specialists. These values are less useful for interpretation in the setting of complete peritonectomy, as the increased amount of normal tissue removed leads to higher false–negative and true–negative rates with resultant decreases in sensitivity and specificity.
Strengths of the current study included the prospective evaluation and large number of specimens obtained due to complete peritonectomy. The majority of patients did not have prior histologic diagnoses of endometriosis; thus, the sample was representative of a population with chronic pelvic pain. Additionally, the pathologists who evaluated the specimens in this study are subspecialized in gynecologic pathology, enabling improved identification of disease.
There were limitations in this study. First, the endometriosis evaluated was only pelvic superficial peritoneal disease. This does not take into consideration endometriosis in atypical locations or lesions that are deeply infiltrating. Additionally, the surgeons who performed the visual evaluation are high-volume endometriosis surgeons with expertise in detecting atypical lesions; this may have limited the generalizability of the study to all surgeons who perform endometriosis surgery.
Conclusions
Despite the use of high-volume endometriosis surgeons, this study found poor reliability for visual detection of endometriosis during surgery. Significant reliance is placed upon the surgeon's ability to visually detect endometriosis intraoperatively, and missing disease could lead to continued symptoms that are often interpreted as postoperative recurrences or delayed diagnoses. Complete peritonectomy nearly eliminates the possibility of missing disease and decreases reliance on the surgeon's eye. Peritonectomy also yields larger specimens, compared with random biopsies, likely leading to increased detection of disease. The potential for atypical appearance and disease not visualized intraoperatively suggests a role for complete pelvic peritonectomy. Future directions include understanding the clinical significance of microscopic endometriosis and evaluating symptomatology following resection of normal-appearing tissue.
Footnotes
Authors' Contributions
Dr. Wasson was responsible for conceptualizing the study; curating the data with Dr. McKee; and administering and supervising the project. Dr. McKee conducted the investigation. Dr. Girardo visualized the study and performed the formal analysis. Dr. McKee wrote the original draft of this article, and, together with Dr. Wasson, reviewed and edited its content.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
There was no financial support for this study.