
Abstract
In the 20 years since its inception, robotic surgery has evolved greatly in its design and clinical use. Most recently, the approach to training and gaining proficiency in robotic surgery techniques has also matured. This article reviews the development of robotic surgery systems, the trajectory of their use for patients with benign and malignant gynecologic conditions, and the advances in novel technologies that are driving the applications of robotic surgery forward. (J GYNECOL SURG 39:204)
Introduction
Robotic and computer-assisted surgery in gynecology began in the early 2000s and has led to impactful developments in gynecologic surgery. 1 In retrospect, the first clinical iteration of the robotic system was a large and cumbersome unit, but it still represented a quantum leap forward in surgical technology. Since then, the robotic system has evolved in complexity and efficiency as a system with expanded clinical use across multiple surgical disciplines. Thus, training paradigms have adapted to teach physicians safe and optimal use of these robotic systems better. This article reviews the past, present, and future of robotic surgery with respect to the robotic systems themselves, their clinical applications, and the evolution of surgical training on robotic systems.
Robotic Systems
The history of robotic surgery is rooted in its proposed military use with telepresence surgery. Minimizing risks associated with moving critically wounded patients, as well as keeping surgeons far from the field of conflict, were the main potential benefits. However, the cost of telesurgery—particularly the telecommunications cost alone—proved to be too high. In addition, lag time across long distances were not suitable or safe for these telepresence surgeries.2,3 Thus, this application was all but abandoned for commercial purposes.
Active, semiactive, and master–slave robotic systems are all currently in clinical use. Active systems work autonomously but remain under control of the surgeon. Semiactive systems have preprogramming that complements surgeon control. Master–slave systems, in which the robot has no preprogramming and depends solely on surgeon control, is the focus of this current discussion, as these systems are used for the majority of gynecologic robotic surgeries.
The first robotic hysterectomy was performed more than 20 years ago with a Da Vinci® System (Standard; Intuitive, Sunnyville, CA, USA), which was approved by the U.S. Food and Drug Administration (FDA) in 2000. 4 This system entered the field when laparoscopy and vaginal surgery used for minimally invasive surgery (MIS). While offering clinical benefits over open surgery with reduced recovery time and decreased postoperative pain, laparoscopic surgery has shortcomings including 2-dimensional visualization, limited instrument articulation and range of motion (ROM), and the need for an individual to hold the camera steady. The first robotic system had a central 10-mm camera arm and 2 additional 8-mm robotic arms. Improvements over laparoscopy included magnified, binocular 3-dimensional (3D) vision; wristed instruments with increased ROM; and tremor filtration and motion scaling to help accuracy and precision. 5
While the first Da Vinci system represented an upgrade in minimally invasive surgery, there was also room for continued improvement. There was no energy integrated in the system; use of any energy instrument required setting up additional energy pedals outside of the console to activate the instrument. While 3D, the visualization was in standard-definition rather than in high-definition (HD). The camera shaft-length was significantly shorter compared to the current robotic system (∼ 38.4-cm Standard versus ∼52.6-cm Xi), which also has longer instruments. Docking the system also proved to be onerous, with arms that had to be screwed into ports placed inside patients. Yet, the system enabled performance of, in the words of Beste et al., “total laparoscopic hysterectomies robotically that otherwise would have required total abdominal hysterectomy.” 5
Since then, each successive generation of the Da Vinci robotic surgical system has evolved by adding a fourth arm; various types of electrosurgery; more instrumentation; HD vision with near-infrared visual capability; and more range and maneuverability for multiquadrant surgery with longer and sleeker scopes, instruments, and ports. An updated single-port robotic platform, introduced with wristed instruments and novel camera manipulation, is approved for various urologic and otolaryngologic indications at present in the United States and with additional applications internationally.
More robotic surgical systems are entering the market with a variety of user-interfaces, different visualization technologies, and differing approaches and applications. The Hugotm robotic-assisted surgery (RAS) system by Medtronic (Minneapolis, MN, USA) features an open console, a modular multiquadrant platform, and integration of artificial intelligence (AI) for data analytics. 6 The first procedures using this system have already been performed in Latin America, Asia, and Europe. 6 The Versius surgical robot by CMR Surgical (Cambridge, U.K.) has lightweight, single-arm patient carts and a separate open surgeon console with 3D glasses, which is approved for use in Europe, Australia, India, and Brazil, and Hong Kong. 7 Johnson & Johnson Services, Inc. (New Brunswick, NJ, USA), continues to develop its Ottava RAS system, which will have 6 arms, offering more control and flexibility, and integration into the operating table. 8 Anticipated integration of AI as well as machine learning (ML) will enable unprecedented opportunities for data analysis and identification of surgical workflow and entropy, which could improve both safe and efficient use. 9
Clinical Applications
The Da Vinci robotic system was FDA-approved for gynecologic surgery in 2005. One of the earliest series of patients undergoing robotic hysterectomies included 16 patients, wherein the average operating time was 242 minutes, the average blood loss was 96 mL, and the mean uterine weight was 131 g. 10 An article on another early series specific to the treatment of gynecologic cancers described robotic surgery for 7 patients with cancers of the endometrium, ovary, or fallopian tube. 11 Each patient underwent total hysterectomy, bilateral salpingo-oophorectomy, pelvic and para-aortic lymphadenectomy, and omentectomy, with a mean operating time of 257 minutes but with low estimated blood loss of an average 50 mL. The average hospital stay was 2 days, less than that for an open procedure.
Robotic surgery has seen both increased use and improved ease of use since its inception. In U.S. hospitals between 2008 and 2015, RAS for total hysterectomy for treating endometrial cancer increased from 9% to 57%, while open surgery decreased from 70% to 28% (Fig. 1). 12 There was a similar trend in the rates of robotic hysterectomy, compared to open abdominal hysterectomy for benign indications. 13 As such, robotic gynecologic surgeries have become more efficient in terms of time and cost. The average operating time for benign hysterectomy has decreased from 242 minutes, as described by Reynolds et al., between 2001 and 2004, 10 to <120 minutes for experienced surgeons in the 2010s. 14 In particular, with the downstream benefits and improved throughput in hospitals, the cost of robotic surgery is less of a consideration when choosing a route of surgery from an institutional perspective, as RAS is now comparable to conventional laparoscopy. 15
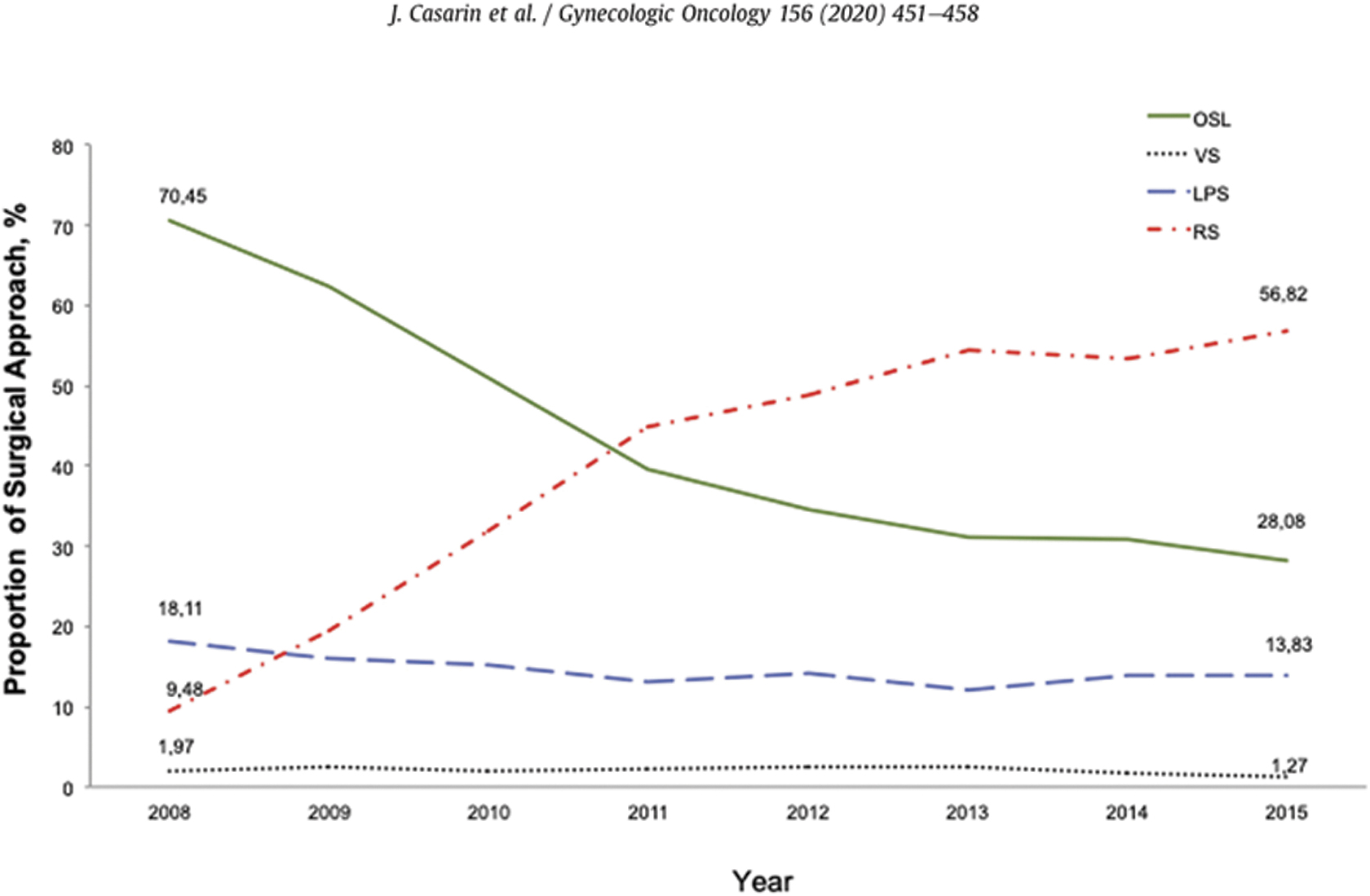
Trends in surgical approach for total hysterectomy for endometrial cancer. 12 OSL, open surgery through laparotomy; VS, vaginal surgery; LPS, laparoscopic surgery; RS, robotic-assisted surgery.
Integration of robotic surgery into treating gynecologic malignancies varies by disease site. MIS, including robotic surgery, has become standard-of-care for treating early stage endometrial cancer, due to improved surgical outcomes and similar oncologic outcomes. The Gynecologic Oncology Group (GOG) LAP2 Study was a randomized controlled trial (RCT) of surgical staging of endometrial cancer via laparoscopy, compared to laparotomy.16.17 The researchers achieved improved short-term postoperative outcomes, such as reduced complications and lengths of hospital stays, and, importantly, found no clinically significant differences in 3-year recurrence rates or 5-year overall survival.16,17 While there have been no randomized trials comparing laparoscopic surgery to robotic surgery for treating endometrial cancer, retrospective data, including a systematic review and a meta-analysis, have not shown differences in survival or recurrence among laparoscopic, robotic, and open approaches.18,19
Robotic surgery for treating early stage cervical cancer is controversial. A large body of retrospective data has suggested similar oncologic outcomes for MIS, compared to laparotomy. 20
The Laparoscopic Approach to Cervical Cancer trial was thus conducted as a noninferiority study of patients with high-risk stage IA1, IA2, or IB1 cervical cancer, who were randomized to MIS (only 15% robotic with the remainder laparoscopic) or open radical hysterectomy with lymph-node assessment. There was significantly lower disease-free survival at 4.5 years with MIS, compared to open surgery (86% versus 96.5%, respectively; hazard ratio [HR]: 3.74; 95% confidence interval [CI]: 1.63, 8.58), and decreased overall survival at 3 years (93.8% versus 99%, respectively; HR: 6.0; 95% CI: 1.77,20.3). 21
A large retrospective cohort study was published at the same time using data from the National Cancer Database and included patients with Stage IA2 and IB1 disease who underwent MIS (90% robotic) or open surgery. This trial also demonstrated a significant increased risk of death associated with MIS surgery, compared to laparotomy (9.1% versus 5.3%, respectively; HR: 1.65; 95% CI: 1.22, 2.22). 22
Subsequent retrospective series have suggested that the increased risk of death may be linked to MIS surgery for larger tumors, as oncologic outcomes were not affected adversely in patients with tumors <2 cm who underwent MIS surgery (Cusimano et al., Doo et al., and Kim et al., all published in 2019).23–25
The ROCC [Robotic Versus Open Hysterectomy Surgery in Cervix Cancer] trial, which is currently ongoing, randomizes patients with early stage cervical cancer to robotic or open radical hysterectomy, may provide further insight on the future of robotic surgery for this indication. *
Minimally invasive approaches have become commonplace in surgical management of adnexal masses, given MIs' well-established improvement in perioperative outcomes. Robotic surgery, in particular, may provide the opportunity for MIS for patients who are not otherwise ideal candidates, such as morbidly obese patients in whom inadequate triangulation and suboptimal surgeon ergonomics can be obstacles to successful completion of a minimally invasive procedure. Although data has indicated longer operative times for adnexectomy with a robotic approach, compared to conventional laparoscopy, this difference did not persist among obese patients with body mass indices >30. 26 The 3D visualization and capacity for magnification unique to robotic surgery can be particularly useful when severe adhesive disease is anticipated, such as in patients with complex surgical histories or patients with suspected endometriosis. In addition, the robotic platform enables a single surgeon to operate with multiple instruments and decreased reliance on a second surgeon or surgical assistant, compared to conventional laparoscopy.
Regardless of which minimally invasive approach is utilized, it is critical to triage patients appropriately to a gynecologist versus a gynecologic oncologist, based on the level of suspicion for malignancy, using criteria such as those offered by the American College of Obstetricians and Gynecologists, and to use techniques that minimize the risk of intraoperative spillage and thus upstaging if there is malignancy. 27 Patients with ovarian cancer whose surgery was performed by a gynecologic oncologist were more likely to have guideline-adherent care and improved survival, especially elderly women. 28
With increasing use of neoadjuvant chemotherapy for advanced-stage epithelial ovarian cancer, particularly among elderly and frail patients, MIS interval debulking after a radiographic response to treatment has become more common. A retrospective National Cancer Database study of more than 3000 women demonstrated similar 3-year survival between patients undergoing laparoscopy and laparotomy (47.5% versus 52.6%, respectively; adjusted HR: 1.09, 95% CI: 0.93,1.28), with similar perioperative outcomes and decreased length of stay with an MIS approach. 29 Specific to robotic interval-debulking surgery, retrospective data suggested favorable oncologic outcomes, with most patients undergoing complete (R0) cytoreduction and median overall survival of ∼40 months in 2 small series.30,31 The LANCE (Laparoscopic cytoreduction After Neoadjuvant ChEmotherapy) trial is ongoing and is designed to determine if a MIS approach is noninferior to laparotomy with respect to disease-free survival in patients with advanced-stage epithelial ovarian cancer following neoadjuvant chemotherapy. †
Surgical Training
Conventional surgical teaching has mimicked an apprenticeship model, whereby a trainee observes a procedure, then begins to perform the procedure under supervision with increasing independence or graded autonomy. With the advent of MIS, additional modalities—including didactics, dry laboratory, wet laboratory, and virtual reality—use standardized exercises, such as needle manipulation, and have been increasingly used to ensure familiarity with the tools and technology prior to live surgery. High-fidelity procedural-based simulation has also been created to assist surgical training. However, there have been no direct comparisons among these teaching methods to determine the most-effective approach. 32 Evaluation is typically subjective or semiquantitative—such as the Likert scale—and it can be challenging to measure progress objectively. It is also yet to be seen if performances on training exercises used in simulations directly correlate with improved performance of specific procedures in live surgeries. The complexity of the robotic system, in particular, tasks learners with simultaneous learning curves for mastering use of the robot as well as the steps of the procedure at for which the robot is being used. This dual tasking can affect the rate at which each task is grasped. 33 Thus, it is imperative to optimize a safe and efficient approach to training residents and fellows.
A variety of robotic virtual-reality simulators have been studied, with several demonstrating face, construct, and content validity. 34 However, these simulators typically focus on completion time of the task or simulated surgery, without focused feedback. Certainly, the metrics of the earliest robotic-surgery simulations also had arbitrary scoring systems without clinical input from surgeon experts. These early simulators were scarce, and they were predominantly used for trade shows and conferences rather than for surgical training. However, as robotic-surgery platforms evolved, so, too, did corresponding simulators with improved graphics, accuracy, and metrics, thus, expanding the simulators' applications for surgical training. Rather than giving generalized feedback, the ability to report objective, individual progress in several different domains of procedural competency can potentially help a trainee identify specific areas for improvement to refine skills or improve efficiency. 35 The direct transfer of skills acquired from virtual-reality training has yet to be validated in robotic-gynecologic surgery; however, results of an RCT conducted in robotic-cardiac surgery demonstrated a benefit of virtual-reality training similar to that of a wet laboratory. 36
A recent single institution study of obstetrics and gynecology residents included individual one-on-one 30-minute sessions with the same faculty member every 4 months over the course of an academic year, utilizing a high-fidelity robotic-hysterectomy simulator (Intuitive Da Vinci Xi Simulator backpack) with a focus on practice-based and systems-based learning. 37 All movements were recorded, and quantitative learning curves were constructed regarding accuracy and economy of motion. Over time, more residents were able to complete an entire hysterectomy within 30 minutes, with only 16% (3/19) at session 1, compared to 94% (29/31) at session 4. Importantly, accuracy and proficiency were improved, with fewer instrument collisions, clutches, and overall movements in the latter sessions while still completing the hysterectomy (Fig. 2), signifying improved surgical efficiency.

Examples of objective, quantifiable surgical metrics for obstetrics/gynecology residents completing a robotic hysterectomy simulation.
With an understanding of educational theory and improved instructional design to leverage and optimize novel technologies, it is possible to obtain more-insightful information on progress through training. Figures 3 and 4 demonstrate simulation performances (under the guise of a multispecialty “Simulation Olympics”) of various residents across multiple surgical specialties (including general surgery, obstetrics and gynecology, thoracic surgery, urology, and otorhinolaryngology) and reproduced at 2 high-volume training centers with separate residency programs with monthly assigned exercises over the course of 1 year.
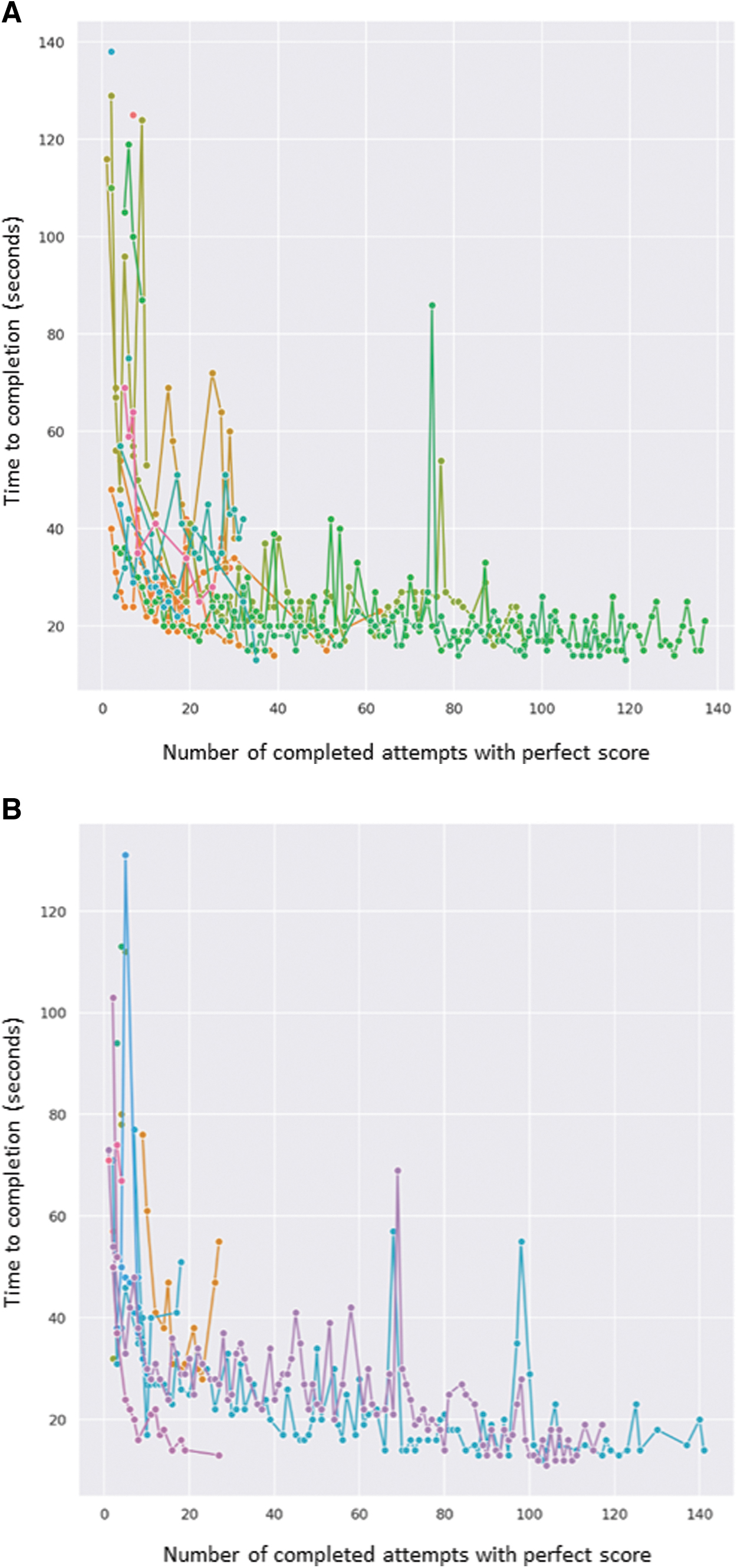
Number of attempts with a perfect score plotted against duration of exercise (seconds) for Vessel Energy Dissection Exercise among obstetrics/gynecology residents at the
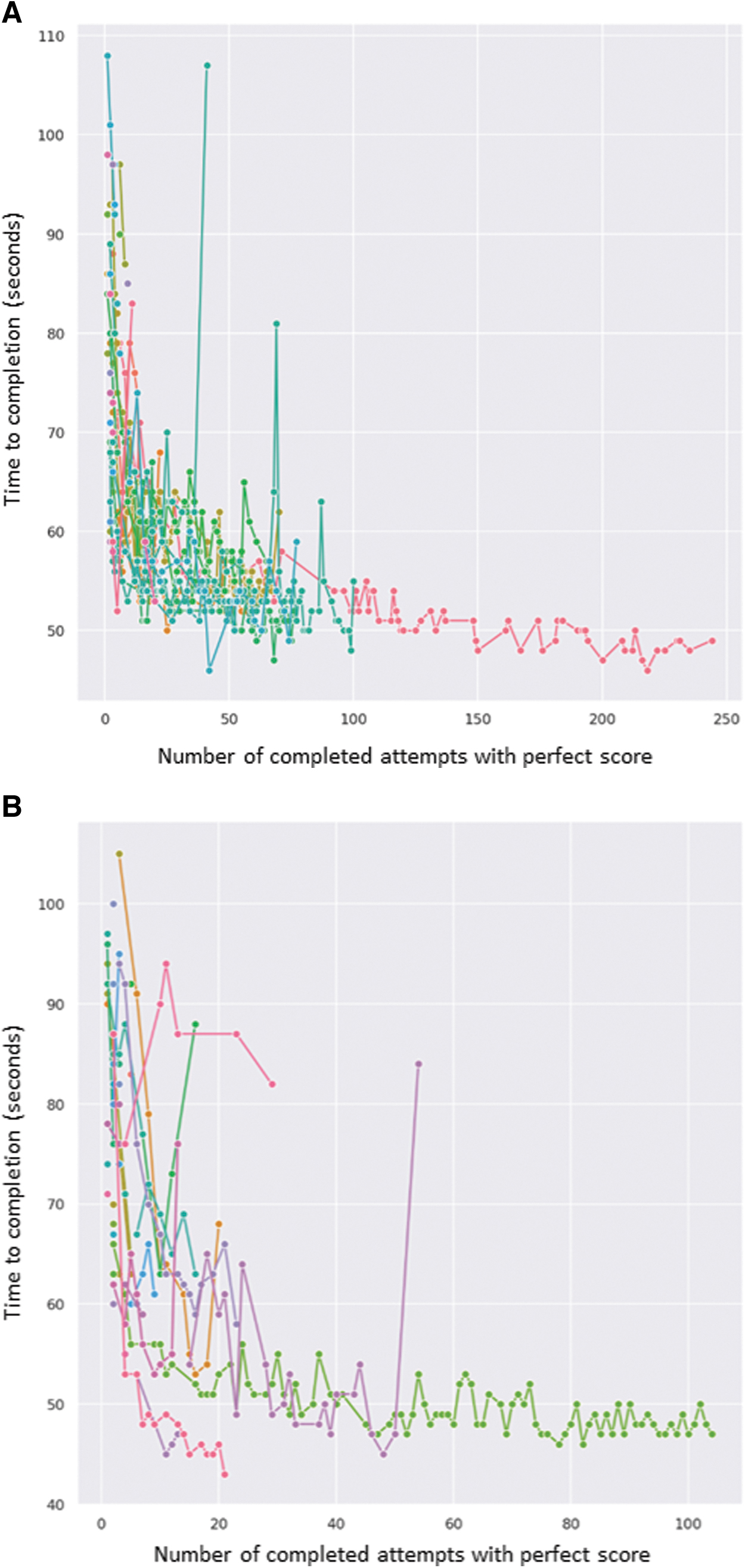
Number of attempts with a perfect score plotted against duration of exercise (seconds) for Energy Pedals 1 Exercise among obstetrics/gynecology residents at the
With sound instructional design, hundreds of attempts at numerous exercises were noted. For each trainee in each exercise, when the number of completed attempts with a perfect score was mapped against the total time-to-completion in seconds, an inflection curve was observed for each individual. This inflection curve was remarkably reproduced across multiple surgical specialties at 2 high-volume institutions. The initial steep portion of the curve represents the rapid learning and improvement occurring during the early learning curve. The horizontal flattened portion of each curve represents when competency was attained—when there was minimal deviation in time-to-completion over multiple completions of a given exercise without sacrificing a perfect score.
These inflection curves differ slightly between surgical trainees, showing the ability to personalize targeted training as individual residents attain competency at differing rates over their number of attempts. This enables us to identify which trainees had faster learning curves, adopting new surgical techniques with fewer repetitions and, maybe more importantly, which trainees require additional training and repetitions to reach competency. Increased use of low-stakes exercises such as these can lead to these novel discoveries to help continue to define surgical competency.
With the emergence of AI and ML, it is now possible to identify and visualize trainee competency in ways that were never imagined previously. With emerging technology, it is possible to obtain surgical metrics from the live operating room (OR), nearly in real time. Figure 5 demonstrates the improvement in motion measured with the assistance of AI and ML in 3D-Cartesian coordinates of 2 different residents performing corresponding portions of a robotic hysterectomy in a live OR at roughly 4-month intervals. Both trainees used less motion over time to complete the hysterectomy, but differences in efficiency between the 2 residents were visualized. These data were broken down into the steps of the hysterectomy, each of which were video-reviewed comparatively with the surgical mentor to fine-tune each individual resident's surgical learning experience. In addition, as the residents returned for training at the specified intervals, the surgical mentor and resident had objective measures of what the resident completed from any previous sessions, enabling them to pick up where they left off, building upon the techniques and skills previously attained and documented. This not only improved training efficiency, but also enabled vastly improved surgical mentoring.

Quantitative Cartesian measurements while completing corresponding portions of a live hysterectomy at 4-month intervals for resident 1
Using these data, it is possible to work on surgical-motion efficiency in a targeted manner, quickening the learning curve for every trainee skill level. This now provides an opportunity to track improvements in surgical efficiency objectively and quantifiably in live surgery, beyond a simulated environment. Additionally, this enables evaluation of surgical entropy—an emerging field that examines how surgery is performed objectively, and shows which surgical steps are actually critical. The procedures are observed and measured over thousands of procedures performed by hundreds of surgeons. These data can then inform designers on how best to create future simulators for increasingly effective translation to the live OR. Moreover, master surgeons will have more tools to become even better surgical mentors.
In the current state of surgical training, students and residents are selected into surgical disciplines without any significant or measurable knowledge of their surgical skills or dexterity. This application could also be expanded to evaluation of residents seeking advanced (i.e., fellowship) training, or even earlier in the trainee timeline if the application enables students to be evaluated in such a manner prior to the matching process for surgical residencies. This technology could also potentially be leveraged as a part of the process for maintenance of certification and (robotic) surgical privileging at the institutional level—processes that are predominantly subjective in nature at this time. While the Da Vinci system currently remains the dominant platform for robotic surgery, these technologies will certainly evolve and expand as more surgical systems and corresponding AI, ML, and simulators come to the market in the near future. Further evaluations are necessary to determine if these are logical and appropriate applications of such emerging technologies.
Conclusions
After nearly 2 decades of robotic gynecologic surgery, existing robotic systems have evolved in sophistication. The entry of several new systems is on the horizon; these have the promise of improved haptics, image integration, and energy efficiency. Robotic surgery has become commonplace among gynecologic oncologists throughout the United States and abroad, with ongoing trials that will help inform the safety and feasibility for some indications. Robotic surgical training has become more specific and objective, with future opportunities for validation and optimization for live surgery. It is important to continue to learn from the lessons of the past, optimize performance in the present, and embrace the challenges of the future while assisting in directing the evolution of technology in the most appropriate manner for the benefit of surgeons as well as the patients we serve.
Authors' Contributions
Dr. Kim was involved in conception of the project, and its methodology, data curation, and formal analysis. Dr. Taylor performed the literature review and assisted with data analysis. Both authors wrote the article.
Footnotes
Author Disclosure Statement
No financial interests exist for Dr. Taylor. Dr. Kim has previously received educational grants from Intuitive and Johnson & Johnson/Ethicon.
Funding Information
There was no funding for this work.