
Abstract
Objectives:
Identifying and resecting gynecologic lymph-node metastases can be challenging. Augmented reality (AR) may improve localization of such lesions and adjacent structures.
Materials and Methods:
For this prospective case series of women who had lymphadenectomy for gynecologic malignancies at a tertiary-care center, a 3-dimensional targeted lesions model was created. It was based on preoperative axial imaging (computed tomography [CT] or positron emission tomography [PET]) of the lesions, which were evaluated by the surgical team preoperatively. The surgeon wore an AR wireless headset, enabling real-time use of the model to assist lymph-node resection.
Results:
This pilot study included 7 patients: 4 had lymphadenectomy with hysterectomy and bilateral salpingo-oophorectomy; 2 had lymphadenectomy; and 1 had lymphadenectomy during pelvic exenteration. Median age was 53 (34–70) and mean body mass index was 28.3 (± 6.5). Mean operating room time was 223 (± 130.9) minutes, mean blood loss was 398.5 (± 600.1) mL, and 1 patient needed a blood transfusion. Overall, there were no significant differences between the preoperative assessments of the sizes and locations of the lesions with AR, compared to axial imaging. Surgeons' evaluations of the model revealed that 7 (50%) indicated that the AR model was superior to axial imaging; 4 (28.6%) noted that the AR model prompted them to change their surgical approaches. AR modeling changed the surgical approaches in 2 cases and improved surgical accuracy, disease characteristics, or intra- and postoperative outcomes.
Conclusions:
Preoperative evaluation with AR was meaningful, compared to conventional methods in 25%–50% of cases. The effect of AR should be investigated further in a larger study. (J GYNECOL SURG 39:289)
Introduction
Gynecologica malignancies are among the leading causes of morbidity and mortality in female patients. 1 Current management includes surgical resection and staging, and then radiation therapy and systemic therapy based on the tumor type, disease stage and patient characteristics. One of the most common paths of spread in gynecologic neoplasms is through the lymphatic system, in particular, to the pelvic and para-aortic lymph nodes.2–4 During surgical resection, whether for primary disease or recurrence, removal of suspected lymph nodes has a therapeutic goal with a potential impact on survival.5–11 Lymph-node dissection (LND) can also be part of surgical staging to define the extent of disease and thus guide optimal adjuvant treatment.12–14
Surgical complications in patients undergoing LND are multifactorial.15–19 The incidence of major organ and vessel injury associated with lymphadenectomy is low.20,21 However, complications impacting lymphatic drainage that are specific to LND are more common.22–24 One of the most-challenging aspects of this procedure is exact localization of the target lymph node and its position in relation to adjacent structures, such as vascular structures, nerves, and ureters. The affected lymph node may not always be enlarged or visualized easily, resulting in a more-complex and wider surgical dissection that increases the risk of surgical morbidity and damage to uninvolved structures. Yet another risk is leaving a metastatic lymph node behind.25–27
Augmented reality (AR) is attracting growing popularity for health technology applications. Projecting preoperatively obtained radiologic images onto the operating field during surgery can allow surgeons to gain a better understanding of the anatomical relationship between pathologic tissue and healthy organs. 28 AR has decreased operative time and improved accuracy during surgical procedures.29,30 Three-dimensional (3-D) imaging enables advanced preoperative planning of the surgical approach and reduces the risk of in-situ trial and error, therefore minimizing potential injuries. 31 For lymphadenectomies, AR can contribute to navigation and to locating a node and its position relative to anatomical structures. Several studies have shown that AR can contribute to better fibroid mapping and lead to a significant improvement in myoma-detection rates. 28 The current study was designed to evaluate the value of AR to preoperative planning of gynecologic oncology surgery.
Materials and Methods
This study protocol was approved by the institutional ethics committee (IEC; Helsinki Committee) of the Sheba Medical Center, Sheba Medical Center, Tel Hashomer, Israel, and all patients provided written, informed consent.
Patient selection and inclusion criteria
This prospective case series included women with gynecologic malignancies who underwent lymphadenectomy at the Sheba Medical Center. Patients were recruited from August 2021 to August 2022. Patients with primary gynecologic malignancies who had suspected lymph-node involvement, based on their preoperative imaging, and who gave their informed consent were included (n = 7). All patients underwent preoperative computed tomography/positron-emission tomography (CT/PET) or CT scans of the abdomen and pelvis. Cases were reviewed at a multidisciplinary meeting and patients were scheduled for surgical resection of the lymph nodes with or without surgery for the primary tumors and other metastases.
Data collection and follow-up
The analysis covered patient demographics and clinical information, including age, body mass index (BMI), American Society of Anesthesiology (ASA) score, and comorbid conditions (hypertension, diabetes, chronic heart disease, respiratory or renal dysfunction; Table 1). Intraoperative parameters were also collected, including the operating time, estimated blood loss (EBL), and number of packed red blood cells (PC) administered (Table 2).
Patients and Disease Characteristics
BMI, body mass index; DM, diabetes mellitus; HTN, hypertension; OSA, obstructive sleep apnea; ASA, American Society of Anesthesiology; op, operative; CT, computed tomography; PET-CT, positron-emission tomography–computed tomography.
Surgical and Perioperative Data
Total = number and % of complications.
EBL, estimated blood loss; SD, standard deviation; PC, packed cells; min, minutes; CD, TAH,
total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy; CD, Clavien–Dindo classification; SSI, surgical-site infection; DVT, deep vein thrombosis.
The extent of surgery was divided into 3 groups: (1) lymphadenectomy alone (removal of suspicious lymph nodes alone); (2) lymphadenectomy with total hysterectomy and bilateral salpingo-oophorectomy (TAH/TLH+SBO); and (3) major debulking (removal of suspicious lymph nodes with another major resection, such as pelvic exenteration, nephrectomy, bowel resection, or other major organ resection). Intra- and postoperative complications were recorded prospectively and were classified according to the Clavien–Dindo classification system.
Study protocol
Generating the AR model
For each patient, a CT scan, or PET-CT, scan of the abdomen and pelvis was performed prior to surgery. The CT scan was loaded as DICOM [Digital Imaging and Communications in Medicine] files on D2P® software (3D Systems Inc., Littleton, CO, USA) for tissue segmentation and 3-D model preparation. The segmentation included the abdomen and pelvis with each enlarged or suspicious lymph node. Adjacent vessels and other important structures were also highlighted and added to the model. The study team participating in the model design was comprised of an AR specialist, a radiologist, and a surgeon.
Model assessment by the surgical team
In addition to the preoperative evaluation in the multidisciplinary meeting, the surgical team evaluated the AR prior to surgery. The 3-D models were viewed in a virtual environment prior to the procedure by the operators using a Vive system, (HTC, San Francisco, CA, USA). For AR visualization, a wireless HoloLens® First Generation (HL1) Head Mounted Unit (HMU) was worn by the surgeons (Microsoft Corporation, Redmond, WA, USA).
The AR model was projected on the patient's body outlines, yielding an estimated localization of the suspicious lymph node and enabling manipulation of the projected image to clarify lymph-node location and the adjacent anatomy (Fig. 1). After the surgical team had evaluated the model and completed the surgery, the surgeons filled in a questionnaire, based on previous publications in the field, 32 to assess whether the AR model had contributed to, or changed, the surgical approach to these cases, compared use of current standard modalities (CT or PET-CT). The questionnaires were then collected and analyzed (Supplementary Box B1; supplementary data are available at: www.liebertonline.com/GYN).
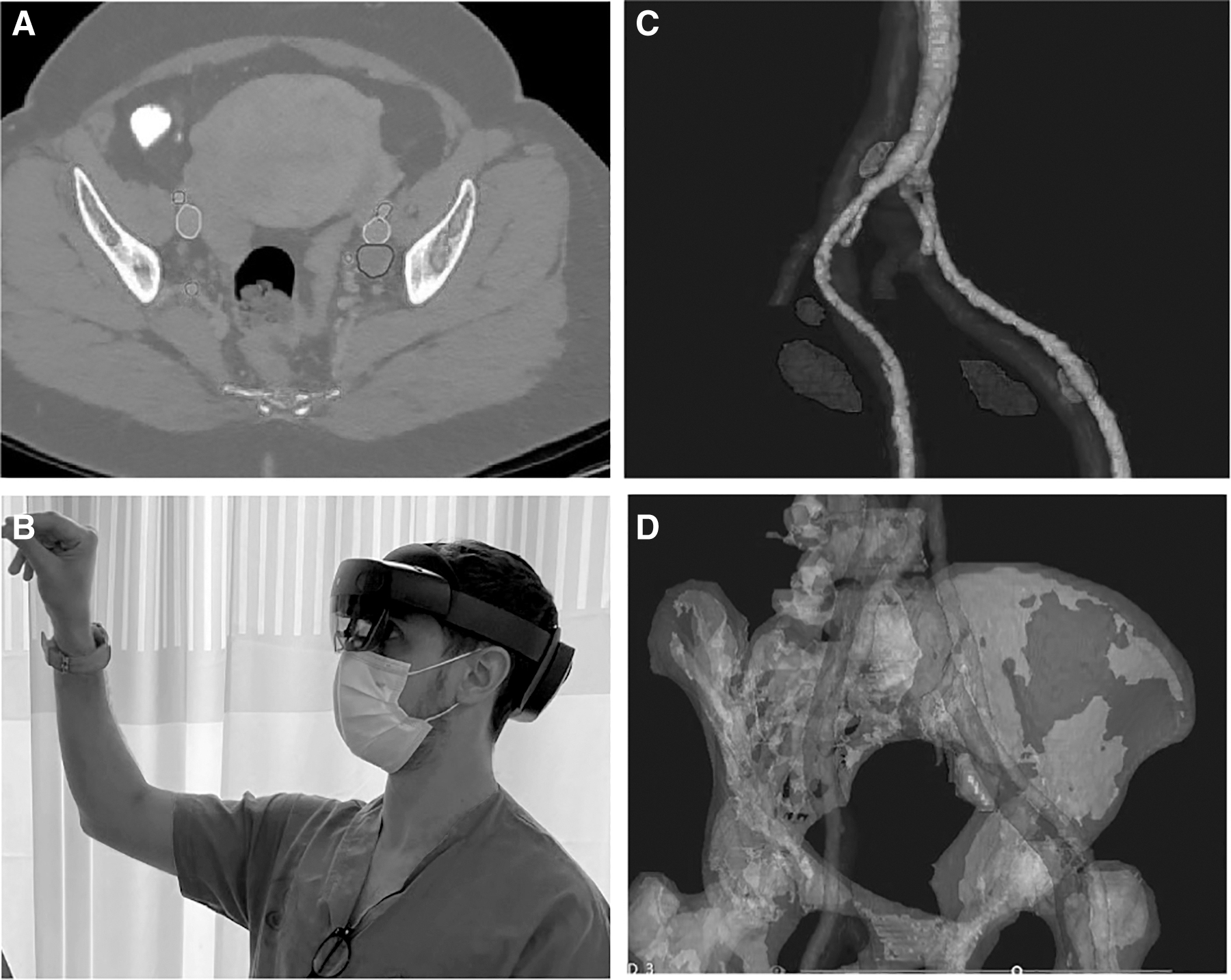
Augmented reality mode.
Statistical analysis
The data analysis was performed, using SPSS, version 25 (Armonk, NY, USA), software. The descriptive statistics used prevalence and percentage values for categorical variables. Continuous variables were used with their means and standard deviations (SDs) for variables with normal distribution, or medians and ranges for variables with skewed distributions. Categorical variables were compared with χ 2 tests, and continuous variables were compared with a t-test at a 2-tailed significance level of 0.05. Surgeon questionnaires were collected and submitted for analysis, focusing on the AR model user's experience and its contribution to the chosen surgical approach.
Results
A total of 7 women who underwent LND for suspected metastases related to gynecologic malignancies met the inclusion criteria and were included in this study. Seventeen women who underwent lymphadenectomy at the Sheba Medical Center between 2018 and 2022 were included in the retrospective cohort.
Patients and tumor characteristics
Table 1 shows the patients' and their tumor characteristics. The median age was 53 (range: 34–70) and the mean BMI was 28.3 (range: 18.3–36.9). Three (42.8%) of the patients had comorbidities. Four (57.1%) patients had an ASA of 3.
The primary malignancies in 3 patients were uterine cancers (42.8%), cervical cancers in 2 patients (28.5%), and an ovarian cancer in 1 patient (14.3%); 1 patient (14.3%) with suspected endometrial cancer had a benign diagnosis upon final surgical pathology. Five patients (71.4%) had primary diagnoses of cancer, whereas 2 (28.5%) had surgery for recurrent disease. Two (28.5%) patients had histories of previous chemotherapy, whereas 1 (14.3%) patient received preoperative radiotherapy. The preoperative imaging showing suspected lymph-node involvement were CT scans in 2 cases and PET-CT scans in the other 5 cases.
Operative and perioperative outcomes
Table 2 shows the outcomes. The mean duration of surgery was 223 minutes (± 130.9). The EBL was 398.5 mL (± 600), with 1 patient requiring a PC transfusion. Two patients (28.5%) had lymphadenectomy alone, 4 (57.1%) had lymphadenectomy with TAH+BSO, and 1 patient (14.25%) underwent a lymphadenectomy with a pelvic exenteration.
The median duration of admission was 3 days (range: 2–32) with no need for intensive care unit admission for any of the patients.
Grade 3 or higher postoperative complications were seen in 2 (28.5%) patients: 1 (14.2%) had a stoma separation requiring surgical reintervention and 1 had a ureteral injury requiring a stent insertion under general anesthesia. The ureteral injury was recognized in the postoperative time, after the patient was discharged from the hospital and had returned with an intra-abdominal collection.
AR impact and evaluation
Two surgeons completed the evaluation questionnaire in each case, for a total of 14. Seven surgeons (50%) indicated that the AR model was superior to current imaging (CT or PET-CT), 6 (42.8%) found that AR was similar to standard imaging, and only 1 (7.1%) found that AR was inferior to standard imaging. One (7.1%) surgeon noted that the AR model could be used to assess the size of a lesion better than standard imaging, 12 (85.7%) found that AR was similar to standard imaging in terms of lesion-size assessment, and 1 (7.1%) found that AR was inferior to standard imaging. Four (28.6%) surgeons noted that the AR model had prompted them to change their surgical approaches.
Discussion
These findings point to the potential value of using an AR model in preoperative settings for tumor visualization and enhancement of surgical planning. This article reported on 7 patients with different gynecologic malignancies who underwent different forms of surgical resection that included lymph-node resections ranging from single lymph-node excisions to extensive debulking and exenteration. Each patient had a tailor-made AR model designed by the study team based on preoperative imaging. The surgical team had access to the AR model prior to surgery and could manipulate the model to explore different angles and pinpoint the location of the suspected lesion and its relation to adjacent structures in order to plan the optimal surgical approach. These results suggest that an AR model can enhance surgical planning in challenging procedures and anatomically complex surgical fields. In their evaluations, most of the surgeons found that the AR model was not inferior to current standard imaging, and more than half found that the model enhanced their planning. Four stated that it led to modifications in their surgical approaches.
Several studies investigated the use of AR technology in operative settings. Bourdel et al. described the contribution of AR to laparoscopic resection of adenomyomas. These researchers reported that AR promoted rapid detection, in real time, of both anatomical structures and lesions, thus facilitating the surgical approach. 33 In another study, similar conclusions were drawn about resection of gynecologic leiomyomas. 34 Akladios et al. used an advanced AR model to identify the ureters in porcine models. 35 The researchers asked 58 surgeons to analyze a surgical visualization and noted a significantly faster identification of the ureters when AR was used. The difference was even more striking when an animal with a previous surgical history was used. 35 Lecointre et al. reported the value of AR in identifying important anatomical structures during surgery in porcine models. 36 He generated an AR model that contained lymph nodes and their surrounding structures. In a questionnaire completed by both experienced surgeons and trainees, AR was ranked significantly higher than direct visualization. 36
The importance of lymph-node resection for gynecologic malignancies and association with survival was described in several trials.5–7 One of the major drawbacks of the procedure is the risk of postoperative complications, such as bleeding, ureteral damage, or long-term lymphedema.15,17,22,24 Although the rate of these complications in experienced medical centers is low, the ability to identify a lesion and its surrounding anatomy clearly is crucial and may not always be straightforward. The current study described the rate of postoperative complications; however, due to the small number of patients in this study, a comparison to the a control group or to an acceptable rate described in the literature, would be difficult and underpowered. Future studies should investigate the use of an AR model and its contribution to shorter operative times, the postoperative course, and better oncologic outcomes.
This study had several limitations. It only involved a small sample and a short-term follow-up that limited the conclusions about perioperative and oncologic outcomes. Assessment of the surgeons' experience and the value of the AR model was subjective and difficult to quantify. Furthermore, the sample was comprised of patients with a wide range of gynecologic malignancies, clinical presentations, and disease burdens that were challenging to control for, particularly with that small sample size.
Conclusions
Overall, an imaging-based AR model may contribute to planning and executing challenging procedures such as lymphadenectomy for gynecologic malignancies. The model can be implemented in the surgical environment and may enhance the surgical approach in patients with complex anatomies. AR's generalizability, intraoperative applications, and impact on both short- and long-term outcomes should be investigated further.
Footnotes
Authors' Contributions
Drs. Mor-Hadar, Mor, and Tejman-Yarden were handled the study's protocol/project development, assisted by Drs. Nagar, Vazhgovsky, Saukhat, Felder, Hochstein, and Korach. Drs. Mor-Hadar and Tejman-Yarden were responsible for data collection and/or management, while Drs. Mor, Devidson, and Cohen conducted the data analysis. Drs. Mor-Hadar, Mor, Helpman, and Korach wrote and edited this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was provided for this project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.