
Abstract
Objective:
Hysterectomy is a widely performed major gynecologic surgery. However, few studies have examined the outcomes of vaginal natural orifice transluminal endoscopic surgery (vNOTES) and compared them with those of conventional laparoscopic hysterectomy. This study assessed if vNOTES hysterectomy is both safe and feasible for patients with noncancerous conditions of the uterus.
Materials and Methods:
This comparative retrospective study was conducted in the department of obstetrics and gynecology at Al-Karak Governmental Hospital, Karak, Jordan. Data on hysterectomy cases were collected from hospital records for operations between January 2018 and January 2023. There were 2 groups of patients: a total laparoscopic hysterectomy (TLH) group and a vNOTES group. Data from each group were obtained on patients' demographics, indications for surgery, and intraoperative and postoperative parameters.
Results:
After exclusions, the TLH group had 44 cases and the vNOTES group had 16 cases. Both groups had similar general characteristics with the most-common indication for hysterectomy being fibroid uteri: ∼ ½ of TLH cases, compared to ∼1/3 of vNOTES cases. Patients who had TLH had significantly shorter surgery durations (151.7 ± 50.4 minutes), compared to patients who had vNOTES (176.3 ± 36.9 minutes); p = 0.044. vNOTES resulted in significantly longer hospital stays (1.8 ± 0.5 days) than TLH (1.5 ± 0.5 days); p = 0.029.
Conclusions:
The vNOTES approach is a novel technique which showed comparable outcomes to conventional laparoscopy. (J GYNECOL SURG 40:132)
Introduction
Hysterectomy is a widely performed major gynecologic surgery. 1 It can be performed through various approaches depending on the indication and surgical experience, which includes laparotomy, laparoscopy, vaginal approach, and even robotic-assisted procedures. 2
The vaginal approach is the most-favorable route for hysterectomy but may be challenged by the limited field of vision—especially in patients with large uteri.3,4 Click or tap here to enter text.In contrast, vaginal natural orifice transluminal endoscopic surgery (vNOTES) presents a solution to these issues by combining the advantages of laparoscopy, in terms of improved visualization, with the safety of the vaginal route. 5
vNOTES hysterectomy is relatively new in the field of minimally invasive gynecologic surgery. vNOTES was first introduced in 2012 by Su et al., and they stated that hysterectomy via trans-vNOTES was feasible to perform but that further research was needed. 6
To date, only a limited number of studies have described the vNOTES surgical approach in detail and assessed its outcomes in comparison to conventional laparoscopic hysterectomy. A systematic review was published in 2020. The review covered 1 randomized-controlled trial and 5 retrospective cohort studies. 7
The aim of the current study was to evaluate the practicality and safety of performing vNOTES hysterectomy. The evaluation was made through a retrospective analysis, comparing vNOTES outcomes with those of total laparoscopic hysterectomy (TLH) in patients diagnosed with benign uterine conditions.
Materials and Methods
Ethical approval
This study was approved by the institutional review board (IRB) of Mu'tah University, Mu'tah, Karak Governorate, Jordan (reference no. 902022), based on this institution's ethical considerations and guidelines. Additionally, the necessity for informed consent was waived.
Study design
This study was conducted in the department of obstetrics and gynecology at the Al-Karak Governmental Hospital, Al-Karak, Karak, Jordan. Patients' records from January 2018 to January 2023 were accessed retrospectively. In addition, all hysterectomy cases with or without salpingo-oophorectomy in that timeframe were included. However, hysterectomies due to intractable uterine prolapse, advanced gynecologic malignancies, or complications of delivery were excluded. Each patient was offered to choose between the vaginal route or TLH. Both procedures were carried out by the same surgeon (A.N.U.).
Data collection
Hospital records were accessed to obtain data regarding parity, age, body mass index (BMI), previous pelvic surgeries, preoperative and postoperative hemoglobin (Hb) levels, weight of uterus after removal, indication for hysterectomy, duration of surgery (from the first incision to the last suture), estimated blood loss (EBL), intraoperative complications, hospital stay, wound-infection status, and the need for blood transfusion.
TLH surgical approach
In TLH cases, the surgical approach was started by applying a Hohl uterine manipulator, followed by primary entry through the umbilicus using a Veress technique. However, in patients with previous midline surgeries, Palmer's point was used for primary entry. After achieving primary entry in a patient, 2 ancillary 5-mm trocars were inserted in the lateral left side. One trocar was inserted medial to the anterior superior iliac spine, and the other trocar was inserted at a fist width on the left lateral side of the umbilicus, after the inferior epigastric artery was identified. An additional 5-mm trocar was then inserted medial to the right anterior superior iliac spine. The abdomen was then insufflated with CO2 up to 20 mm Hg for primary entry and up to 15 mm Hg during the operation. The procedure involved sealing and cutting the round ligaments (developing a bladder flap), uterine arteries, and cardinal ligaments using laparoscopic-based advanced bipolar energy (5 mm) in a cranial to caudal direction. Afterward, the uterus and/or adnexa were removed through the vaginal opening and then the vaginal vault was sutured laparoscopically with polyglactin 910 sutures.
vNOTES surgical approach
After a patient was anesthetized, bimanual examination was performed to confirm the size and mobility of the uterus, in addition to the adnexa. The anterior and posterior lip of the cervix were grasped with 2 tenaculi, and the posterior vaginal wall was pushed down by the first assistant using a single-end Sims' speculum. Subsequently, the posterior vaginal wall bulged at the level of the cul-de-sac (Fig. 1).

Cul-de-sac level where the posterior vaginal wall bulges.
The bulge was grasped with an Allis clamp in a transverse fashion at the level of the uterosacral insertion. Then, the vaginal wall was cut between the cervix and the Allis clamp, using curved heavy-tissue scissors. After this step, the vaginal wall and the peritoneum opened. (Sometimes, the posterior peritoneum does not open, so it should be grasped again with an Allis clamp and cut.) After opening the posterior colpotomy, a Heaney retractor was inserted. Then, the tenaculum holding the cervix was pulled downward, so that the surgeon could identify the junction between the vaginal rugae and the smooth cervical epithelium. Following that, the vaginal wall was cut at this level, using the curved heavy-tissue scissors, and was grasped upward using 2 long Allis clamps (Fig. 2). Next, using the same scissors, the supravaginal septum was opened. Next, dissection was continued upward against the cervix until the vesicouterine peritoneal fold appeared, and then it was grasped with artery forceps and cut to accomplish an anterior colpotomy.
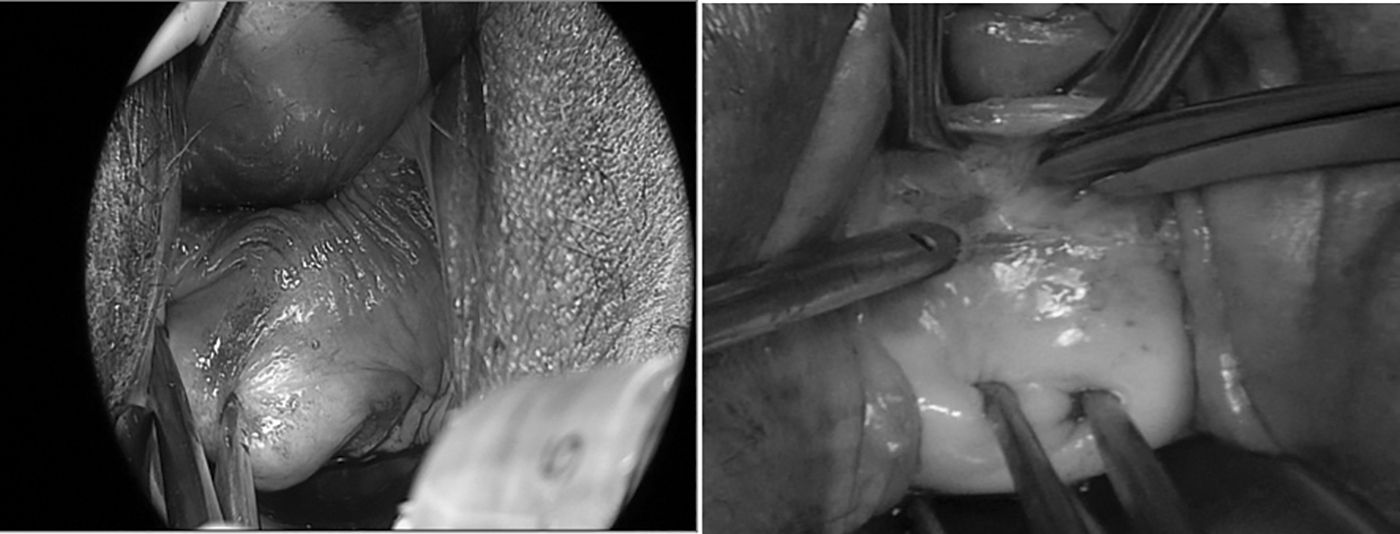
Cutting through the vaginal wall using the curved heavy-tissue scissors (2 views).
However, it is sometimes difficult to identify this fold, so it is acceptable to dissect the vaginal wall, and the anterior peritoneum can be cut after endoscopic identification later in the operation.
Following, the anterior and posterior colpotomies, the paracolpium was cut at each side. This was performed by applying 2 Heaney retractors on the anterior and the posterior sides. To identify the paracolpium clearly, the second assistant had to pull both Heaney retractors in an oblique fashion and the first assistant had to pull the cervix with the applied tenaculum in a transverse fashion (Fig. 3). For example, the first assistant pulled the cervix to a 9 o'clock position, the second assistant pulled the anterior retractor toward a 2 o'clock position and the posterior retractor to a 5 o'clock position. Then, using heavy cured tissue scissors, the surgeon cut the vaginal wall and the paracolpium tissue along with the anterior and posterior colpotomy incisions. At this this stage, the uterosacral and the cardinal ligament was clamped clearly and cut, respectively, as in a vaginal hysterectomy or could be cut with an advanced bipolar energy device.

Identifying the paraclopium.
Then, the surgeon could use a ready-made port—which is the same as ports used for single-port surgery. However, a homemade port was used, which consisted of a small Alex's retractor and medium-sized sterile gloves containing 2 10-mm and 1 5-mm disposable ports. The green ring of the Alex's retractor was squeezed by the surgeon's left hand into an oval shape and pushed into the vagina with the right index finger above the level of the posterior vaginal wall, and then anteriorly at the level of the symphysis pubis above the edge of the anterior vaginal wall. Then the retractor spread on the pelvic-floor muscle spontaneously (Fig. 4). (It is not uncommon that the ring does not spread over the pelvic floor. This is mainly because the cardinal ligament is partially cut, and this prevents the ring from spreading laterally. If this occurs, at this step, the surgeon must remove the retractor and then clamp, cut, and ligate the remaining cardinals on both sides.) After applying the green ring, the glove port was applied over the white ring and the ring was rolled outward until it was applied over the vulva.
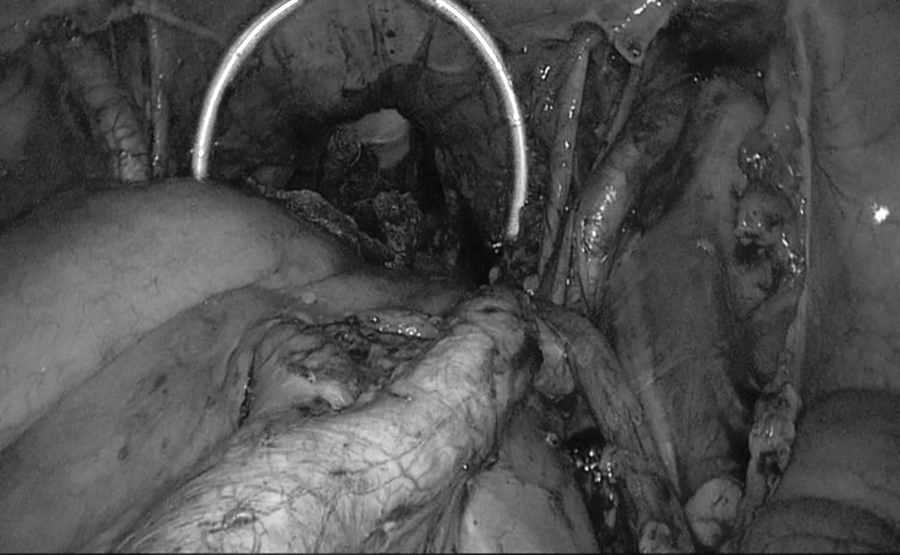
This laparoscopic view showing the end of the retractor (shown as a white arc) spread over the pelvic floor.
The gas tube was then connected and the abdomen was insufflated up to 15 mm Hg. Then, the head was tilted down 15°, which helped move the bowel up. (Both 10-mm 30° or 0° scopes could be used depending on the surgeon preference. If the anterior vesicouterine peritoneal fold is not opened yet, it should be opened by grasping the cervix using a single-tooth tenaculum and pushing the cervix in and backward to stretch the peritoneal fold and then the peritoneum can cut using scissors [Fig. 5]. Sometimes, the peritoneal fold is still difficult to identify. So, the surgeon can ask the second assistant to press gently on the abdominal wall during this maneuver, so that the peritoneum bulging becomes noticeable.)

Vesicouterine peritoneal fold.
The next step was coagulating and cutting the uterine artery at the level of its insertion to the uterus, which is at the same level the vesicouterine fold. The uterine artery was identified by pushing the cervix opposite to the working side, a using single-tooth tenaculum to grasp the anterior and posterior lips of the cervix firmly and pushed them to either side in a transverse fashion (Fig. 6). (If the surgeon is working on the left side, then the cervix should be pushed to the right and vice versa.)

Identifying the uterine artery.
Following uterine devascularization, the broad ligament and the round ligament were coagulated and divided along the uterine body. The plane of cutting was exposed by grasping the uterine side wall 2 cm below the cutting plain and pushing it to the opposite side using a single-tooth tenaculum. When the surgeon reaches the level of the ovarian ligament, he or she should divide it after multiple treatment with the advanced bipolar device to preserve the ovaries. Then, the broad ligament should be cut along the fallopian tube and the plain of cutting is exposed by grasping the tube with a 5-mm smooth grasper and pushing it to the opposite side. The last step in this phase is to divide the fimbrial end from its attachment to the ovary. However, if the ovaries are to be removed, they should remain attached to the uterus and the anterior and the posterior leaf of the broad ligament, and should be separated after the division of the round ligament, and then cut separately above the level of the pelvic brim. To identify the infundibulopelvic ligament, the surgeon should grasp the ovary with a smooth grasper and push it to the opposite side and skeletonize the infundibulopelvic ligament before coagulating and cutting it. The surgeon must identify the sigmoid colon before cutting the left infundibulopelvic ligament. Following dividing both sides, the surgeon grasps the cervix and pulls it through the vagina after releasing the 3-channel port.
Usually, the uterus needs to be cut. Following the removal of the specimen the port is applied again to check hemostasis and then the retractor is released and the vaginal vault is closed as in a vaginal hysterectomy.
Statistical analysis
Categorical data were expressed in frequencies and percentages, and continuous data were expressed as means ± standard deviation. A Mann–Whitney-U test and Fisher's exact test were used were applicable. A p-value of ≤0.05 was considered significant. Data were analyzed using IBM SPSS version 25.0 (SPSS, Inc., Chicago, USA).
Results
This study included a total of 62 hysterectomy cases from January 2018 to January 2023. Patients were divided into 2 groups; the first group included 46 TLH cases and the second group included 16 vNOTES cases. Out of the 46 TLH cases, 1 case was converted to total abdominal hysterectomy, and 1 procedure was performed for an intractable uterine prolapse. Therefore, these 2 cases were excluded from the final analysis.
Table 1 shows that both groups were similar in terms of age, parities, BMIs, preoperative Hb, weight of uteri, and frequency of previous pelvic surgeries.
Demographics and Clinical Characteristics of Included Patients
Mann–Whitney-U test.
†Fisher's exact test.
TLH, total laparoscopic hysterectomy; vNOTES, vaginal natural orifice transluminal endoscopic surgery; yrs, years; SD, standard deviation; BMI, body mass index, Hb, hemoglobin.
The most-common indication for hysterectomy in the TLH group was fibroid uterus (52.3%), followed by abnormal uterine bleeding (15.9%) and endometrial hyperplasia (15.9%). In the vNOTES group, the most-common indication was also fibroid uterus (37.5%), followed by adenomyosis (25.0%). See Table 2.
Indications for Hysterectomy
TLH, total laparoscopic hysterectomy; vNOTES, vaginal natural orifice transluminal endoscopic surgery; AUB, abnormal uterine bleeding.
Both groups were similar in terms of intraoperative complications. However, the duration of surgery in the TLH group (151.7 ± 50.4 minutes) was significantly less, compared to the vNOTES group (176.3 ± 36.9 minutes); p = 0.044. However, the TLH group had higher EBL (309.9 ± 153.7 mL), compared to the vNOTES group (250.0 ± 70.7 mL), although the difference was not statistically significant; p = 0.311 (Table 3).
Intraoperative Parameters
Mann–Whitney-U test.
TLH, total laparoscopic hysterectomy; vNOTES, vaginal natural orifice transluminal endoscopic surgery; min, minutes; SD, standard deviation; EBL, estimated blood loss.
Finally, Table 4 shows that neither of the groups differed significantly regarding postoperative Hb, frequency of wound infection (none), and need for blood transfusion. However, the vNOTES group had significantly longer hospital stays (1.8 ± 0.5 days), compared to the TLH group (1.5 ± 0.5 days); p = 0.029.
Postoperative Parameters
Mann-Whitney U test.
†Fisher's exact test.
Bolding indicates significant result.
TLH, total laparoscopic hysterectomy; vNOTES, vaginal natural orifice transluminal endoscopic surgery; Hb, hemoglobin; SD, standard deviation; d. day(s); N/A, not applicable.
Data availability
Patients' data are available upon request, due to ethical considerations.
Discussion
In any comparative study of surgical procedures, the focus is on the important parameters, starting with operation time. As occurred in the study results, the operation time needed to complete the vNOTES hysterectomy was significantly longer, compared to the time needed to complete TLH (176.3 ± 36.9 minutes, 151.7 ± 50.4 minutes, respectively). This operation time was not consistent with the results of Kaya et al. showing that that their operation time for vNOTES hysterectomy was significantly shorter than their TLH time, which they considered a major advantage favoring vNOTES hysterectomy in that study. 8 This difference in results could be attributed to vNOTES hysterectomy being a new approach for the hospital in the current study and the staff being not familiar with this technique. In addition, vNOTES hysterectomy—as related thoroughly in the surgical description—is performed in 2 parts, (1) before applying the uterine port and (2) after applying the vaginal port.
Moreover, it was not clear in the other study 8 how those researchers calculated the operation times. This is also true for other studies—it is unclear how the durations of the operation were calculated.5,8–12
In addition, the mean hospital stay in the current study was significantly longer in the vNOTES group (1.8 ± 0.5 days) than in the TLH group (1.5 ± 0.5 days). Other similar studies have shown that patients undergoing vNOTES had shorter hospital stays, compared to patients undergoing laparoscopic surgery for hysterectomies.8–13 One of the results of other similar studies— in a study published in 2021 [e-published in 2020] by Kaya et al., 8 —was that the mean hospital stay was significantly shorter for patients who underwent vNOTES hysterectomy (48.33 ± 33.12 minutes) than for patients who underwent conventional laparoscopy (72.23 ± 43.63 minutes). Furthermore, a similar study by Basol et al., in 2021, 9 found that the mean hospital stay for vNOTES cases were significantly shorter, compared to single-port laparoscopic hysterectomy cases (31.15 hours and 43.85 hours, respectively). The contradictions between the current study's results and the aforementioned studies9–13 occurred because the current authors preferred to keep the patients longer in the hospital for observation and monitoring for any unexpected complications, thus hesitated to discharge patients on the first day.
However, with more experience with vNOTES, the current authors started to discharge the patients 1 day after their operations.
In the current study, EBL was less with vNOTES, compared to TLH (250.0 ± 70.7 and 309.9 ± 153.7, respectively). However, the difference was not statistically significant. Previous studies have reported significant differences in blood losses when comparing vNOTES to TLH. This difference was in favor of vNOTES over TLH.8–12 The primary reason for the reduction of blood loss in vNOTES is the early devascularization of the uterus. The vaginal approach is also considered advantageous as it enables easier access to the uterine artery, compared to laparoscopic procedures, which can be challenging to perform, particularly when patients have larger uteri.
In this study the specimen weight was heavier in the vNOTES group but this was not statistically significant; the mean weight was ∼338.8 g. In a similar study, vNOTES was confirmed to be feasible for patients with uterine weights >1000 g. 14 The current authors concur that, in vNOTES, uterine size is not a limiting factor in completing the procedure. In TLH large uteri make approaching the uterine artery—especially the right 1—difficult (the 1 opposite to the surgeon position), thus, in some cases, it is necessary to perform a subtotal hysterectomy, then remove the cervix.
Although BMI was similar in both groups of patients in the current study, the vaginal approach was not affected by a high BMI, whereas laparoscopic procedures were hindered by it. This is due to the larger omentum that usually occurs with a high BMI and that can make it difficult to move the bowel out of the way and expose the uterus during laparoscopic procedures. With vNOTES, there was no need for concern about bowel obstruction, making vNOTES a potentially superior option for patients with high BMIs.
Conclusions
vNOTES is a procedure that shows great potential, especially for patients with high BMI and large uteri. vNOTES has been proven to be safe and feasible not only in the current study but also in other published articles. However, the small size of the current study sample restricts the generalizability of these findings, and more-extensive research is needed. Nonetheless, the current authors believe that there is a need for a precise explanation of how to perform this procedure in the existing literature.
Footnotes
Authors' Contributions
Drs. Uwais, Mahmoud, Alkhanazreh, Abutouq, Albaqaeen, and Satari conceptualized, visualized and administered this project. Drs. Uwais, Jahameh, Al-Hawamdeh, Al-Abadleh, Altarawneh, Mahmoud, Alkhanazreh, Abutouq, Albaqaeen, and Satari were responsible for supervising the work and designing the methodology. Drs. Jahameh, Al-Hawamdeh, Al-Abadleh, Altarawneh, Mahmoud, Alkhanazreh, Abutouq, Albaqaeen, and Satari worked on obtaining resources and software. this group conducted the investigation, together with Dr. Uwais, and curated the data, performed the formal analysis. Joining together again with Dr. Uwais, they validated the results. Drs. Uwais, Mahmoud, Alkhanazreh, Abutouq, Albaqaeen, and Satari wrote the original draft of this article. Drs. Uwais reviewed the draft, edited it, and prepared article's the final version.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
This study did not receive any funding.