
Abstract
Objective:
The purpose of this single-blind, single-center clinical trial study was to compare the effect of a clear liquid diet versus mechanical bowel preparation (MBP) before surgery on surgical field visualization, postoperative pain, and postoperative symptoms in women undergoing benign gynecological laparoscopic surgeries.
Materials and Methods:
A total of 120 women scheduled for benign gynecological laparoscopic surgery were allocated to two groups. In group 1 from 24 hours before the surgery, the patient was on a clear liquid diet and should have been fasting 8 hours before the surgery (Diet group). Group 2 received four packets of polyethylene glycol powder in the evening before the operation and was fasting from midnight before the operation (MBP group). The outcomes included the comparison of intraoperative visualization of the surgical field, ease of bowel handling, postoperative pain, and gastrointestinal discomforts between the two groups.
Results:
The intraoperative visualization of the surgical field score (p = 0.06) and ease of small and large bowel handling rating were similar between the two groups (p = 0.19 and 0.59, respectively). Compared with the MBP group, patients in the Diet group experienced fewer complications including abdominal pain, vomiting, anal stimulation, hunger, and postoperative flatulence.
Conclusions:
Administration of clear liquid diet 24 hours before surgery seems to have comparable results with MBP in terms of surgical field of view and ease of bowel handling. However, fewer gastrointestinal discomforts were observed in the diet group.
Introduction
Since the 1970s, mechanical bowel preparation (MBP) has been used before laparoscopic surgery to reduce residual fecal matter in the bowel and reduce infection. 1 However, this issue has not been proven in patients undergoing laparotomy or laparoscopy. 2 However, despite the lack of supporting literature, MBP is mainly used in laparoscopic gynecological surgery. 1
In laparoscopic gynecological surgery, it is important to have a wide surgical field and easy bowel handling because the pelvis and intestine have limited space. 3 It is believed that MBP can obviate this problem. 3 Some studies have reported that MBP before laparoscopic surgery is associated with patient dissatisfaction,3–5 and it is no different from no bowel preparation in surgical field view and bowel handling. 6 However, an empty bowel before abdominal or pelvic surgery may be beneficial for improving the surgeon’s field of view and reducing peritoneal contamination in patients with intestinal damage. 7 Since diet has an important role in intestinal function, 8 a special diet to minimize colonic fecal content might help to increase the visibility of the surgeon without side effects of MBP (patient discomfort and dehydration). This study aimed to compare the effect of a clear liquid diet versus MBP before surgery on surgical field visualization, postoperative pain, and gastrointestinal discomforts in women undergoing benign gynecological laparoscopic surgeries.
Methods
This single-blind, single-center clinical trial study was conducted in Arash Women’s Hospital, Tehran, Iran, from August to October 2022, after approval from the Ethics Committee of Tehran University of Medical Sciences, Tehran, Iran. The study was registered in the Clinical Trial Registry of Iran (IRCT Id: IRCT20140111016161N9). An informed written consent was taken from all participants. This study adheres to the applicable CONSORT guidelines.
Study population
Women aged 18–65 years, who were scheduled for benign gynecological laparoscopic surgery (grades ΙΙ and IΙI) were recruited to this study.
Exclusion criteria consisted of women candidates for laparoscopic surgeries with grade I such as diagnostic laparoscopy, tubal ligation, and biopsy, as well candidates for laparoscopy with grade 4 such as lymphadenectomy, severe endometriosis, and presacral neurectomy, women with severe obesity (body mass index [BMI] above 35), inflammatory bowel disease and colitis, and history of multiple previous surgeries and severe adhesions.
Randomization and blinding
Participants were randomly divided into two groups: MBA and Diet groups. The block randomization method was carried out by using www.sealedenvelope.com. Group assignment was performed by sealed envelopes prepared by a clinic nurse. All surgery was performed by the same surgeon team.
The surgical team who was unaware of the type of intervention recorded the outcomes of the study. Also, a statistician who is separate from the study process analyzed the results. Due to the type of intervention, the participants were not blinded in this study.
Intervention
Two days before the surgery, all participants completed a questionnaire providing information on age, weight, BMI, gravidity, history of gastrointestinal disorders, and history of previous abdominal surgery. Diet group: From 24 hours before the surgery, the participants were on a clear liquid diet, including light-colored fruit juices without pulp, tea, or coffee (which could be sweet), water, honey, compote water without fruit pieces, filtered soup, and strained meat or chicken water. The participants were instructed to avoid consuming solid foods, milk, buttermilk, alcoholic beverages, soft drinks, and smoking. The patients should have been fasting 8 hours before the scheduled surgery.
The MBP group received four packets of polyethylene glycol (PEG) powder in the evening before the operation and was fasting from midnight before the operation. The participants were asked not to have any other diet.
Then the patients underwent laparoscopic surgery, during which relevant information, such as the duration of the surgery, and complications, such as damage to visceral tissues, were recorded. The patients were followed up after the surgery, and postsurgery hemoglobin was recorded.
After surgery, the surgeon, who was blinded to the study, was immediately questioned regarding pelvic visualization and bowel handling according to the following 5-point visual analog scale (VAS) (the number 0 means the bad condition and the number 5 indicates the best condition).
A questionnaire was completed by the patients on the morning of the day of surgery and immediately following the administration of the diet postsurgery regarding digestive discomforts, such as nausea, vomiting, flatulence, and chest pain. This was carried out by interviewing and examining the patients and completing a questionnaire based on a 4-point scale (score 0: no symptoms, score 1: mild, score 2: moderate, and score 3: severe symptoms). The severity of pain, flatulence, and nausea after the operation were evaluated by using the VAS score in all participants.
Outcome measures
The outcomes were comparing the visualization of the surgical field, bowel handling, and patient’s digestive discomforts after surgery between two groups.
Statistical analysis
Intention-to-treat analysis was used to maintain the random allocation process. Student’s t-test, Mann–Whitney U test, and chi-square test were used to compare outcomes as appropriate. p values less than 0.05 were considered significant.
Results
A total of 120 women who were scheduled for benign gynecological laparoscopic surgery were consecutively assigned into two groups: 60 patients in the Diet group and 60 patients in the MBP group (Fig. 1).
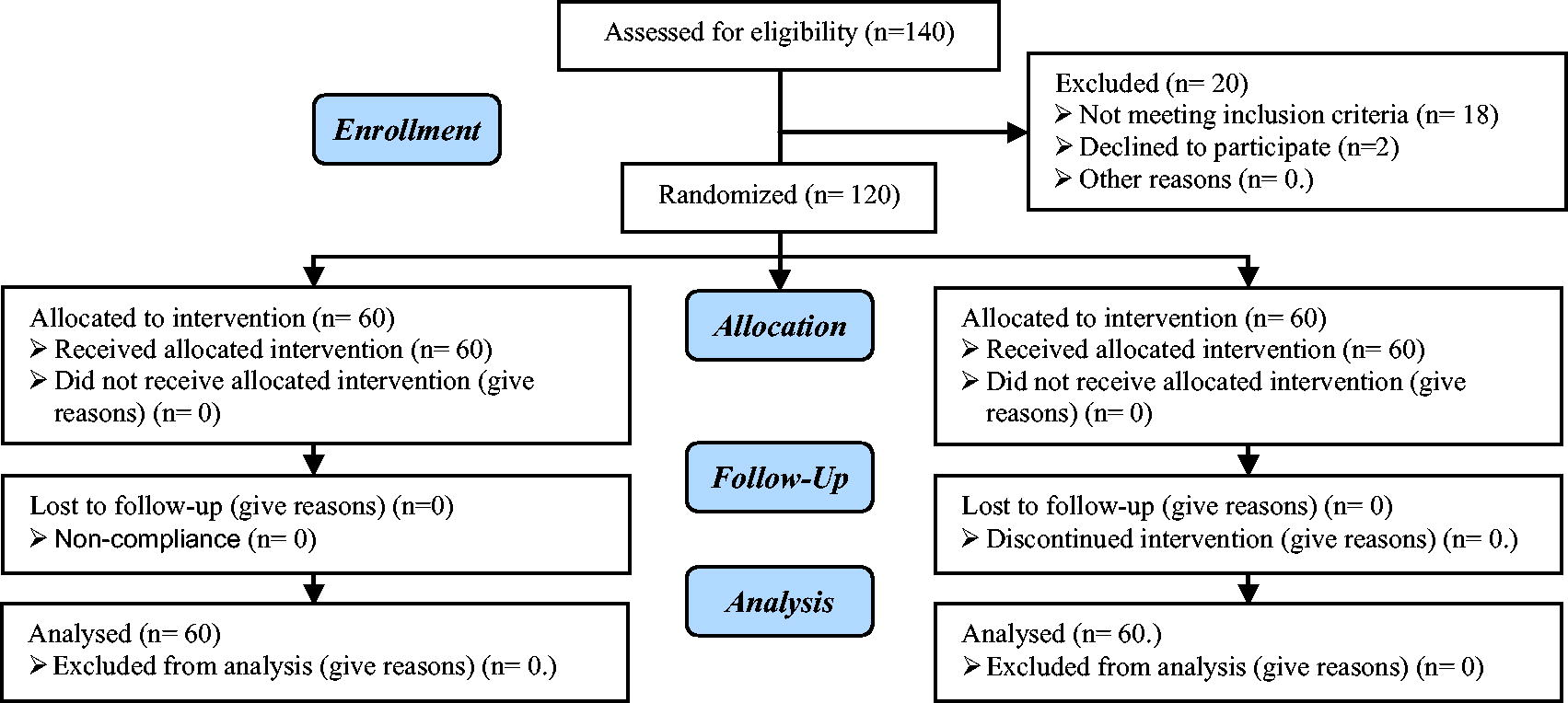
Summary of patients flow.
The mean (standard deviation [SD]) age of participants in the Diet group was 36.42 (3.2) and in the MBP group was 35.71 (4.17). The mean (SD) BMI of participants in the Diet and the MBP groups were 23.5 (4.21) and 24.3 (3.31), respectively. Both groups were comparable in terms of age and BMI (Table 1). The reasons for performing laparoscopic surgery in both groups are shown in Table 1. Hysterectomy was the most common reason for laparoscopy in both groups. There was no statistically significant difference between the two groups in terms of reasons for surgery (p = 0.82). During surgery the mean (SD) ease of small bowel handling in the Diet and MBP groups were 3.31 (0.38) and 3.16 (0.80), respectively.
Demographic and Surgical Information
Student’s t-test.
Chi-squared test, +Mann–Whitney U test.
BMI, body mass index; MBP, mechanical bowel preparation; SD, standard deviation.
As well the ease of large bowel handling rating was 3.84 (0.81) and 3.93 (0.82) in the Diet and MBP groups, respectively. There was no statistically significant difference regarding the ease of small and large bowel handling between the Diet and MBP groups (p = 019 and p = 0.59, respectively) (Table 2).
Surgeon Questionnaire Scores Evaluated by Using a 5-Point VAS
Mann–Whitney U test.
VAS, visual analog scale.
Patient’s Symptoms After Bowel Preparation Before Surgery in Both Groups by Using 4-Point Scale
Score 1, mild symptoms; score 2, moderate symptoms; score 3, severe symptoms.
Chi-squared test.
Severity of Patient Symptoms After Laparoscopic Surgery by Using a 5-Point VAS
Mann–Whitney U test.
Intraoperative visualization of the surgical field rating was 3.11 (0.58) and 3.31 (0.6) in the Diet and MBP groups, respectively, and was not statistically different (p = 0.06). No participants were involved in bowel resection.
The median (min–max) total operation time were 135 (35–175) and 123 (60–166) in the Diet and MBP groups, respectively (p = 0.3). The difference in hemoglobin levels before and after surgery was similar between the two groups with a p value of 0.15.
Compared with the MBP group, patients in the Diet group experienced significantly fewer gastrointestinal symptoms, including flatulence, vomiting, anal stimulation and hunger and abdominal pain on the morning of surgery (before surgery). There was no statistical difference in regard to thirst, nausea, fatigue, flatulence, tiredness, and chest pain on the morning of surgery between the two groups (Table 3). On the day after surgery, patients in the MBP group complained more about flatulence (p < 0.001). However, the postoperative pain and nausea score were not significant between the two groups (p = 0.41 and p = 0.18, respectively) (Table 4).
Discussion
This study aimed to compare the surgical field and patient outcomes in women with benign gynecology laparoscopy surgery receiving the two methods of bowel preparation (MBP or consuming a clear liquid diet) before undergoing laparoscopic surgery. The results showed that the extent of visualization of the surgical field and bowel handling after surgery were similar in the patients receiving either of the preparation methods. However, abdominal pain, vomiting, anal stimulation and hunger and postoperative flatulence were significantly more prevalent in the MBP group than in the clear liquid diet group.
Limited studies have evaluated the impacts of preoperative diet on surgical parameters and morbidity in patients undergoing gynecological laparoscopic surgery.
Mulayim et al. randomly divided 275 women with benign gynecological diseases, who were candidates for laparoscopy, into three groups, including receiving oral sodium phosphate (NaP) solution (n = 96), NaP enema (n = 92 people), and fasting (n = 90). The results showed no significant differences between the three groups in terms of the surgery visualization field, bowel handling feasibility, and the overall ease of surgery. These findings revealed no beneficial role for MBP in patients with high BMI undergoing hysterectomy or laparoscopy. 3 The method of this study is different from our study. In our study, in addition to fasting before surgery, we also used a liquid diet.
In another randomized clinical trial on 70 patients (excluding people with high BMI and grade 3 and 4 endometriosis), Lijoi et al. showed that MBP with oral NaP had no additional beneficial effects in improving the surgeon’s field of view and bowel handling compared with 1 week of a low-fiber diet. 9 Our study is in line with the study but the kind of diet is different.
In another study, 144 women who were candidates for laparoscopic surgery were randomly assigned to three groups, including treatment with a liquid diet on the day before surgery, MBP, and treatment with a minimal-fat diet for 3 days. The intraoperative visualization field and handling of the large and small intestines were less satisfactory in patients who received MBP than in other groups. In addition, preoperative discomfort was significantly higher in the MBP group. 1 Our study is in line with study.
In a clinical trial by Won et al., the effectiveness of three types of interventions, fasting only, 2-day minimal-residue diet, and 2-day minimal-residue diet plus MBP along with oral sodium picosulfate, was assessed in 308 women who were candidates for laparoscopic gynecological surgery. They showed that the minimal-residue diet and MBP delivered statistically significant improvements in the surgical field of view and bowel handling; however, based on the surgeon’s overall score, this improvement seemed to have small clinical significance. In addition, those receiving MBP plus the minimal-residue diet experienced digestive discomfort. 10 The most common MBP regimens include oral or rectal laxatives.2,11 NaP and PEG are more commonly used. The negative consequences of bowel preparation include discomfort for patients, such as postoperative pain, nausea, vomiting, abdominal distension, insomnia, fatigue, and metabolic disorders. 12 In our study, the patients undergoing MBP complained of vomiting, abdominal pain, anal stimulation, hunger, and postoperative fatigue, at a significantly higher rate than their counterparts receiving the clear liquid diet.
In our study, no case of intestinal damage occurred, so we could not assess the effect of bowel preparation on this phenomenon. Studies indicate that laparoscopic surgery is associated with a low rate of morbidities such as infection and intestinal injuries. In this regard, the total rate of morbidities and intestinal injuries for laparoscopic hysterectomy has been reported to be 9.4% and 0.4%, respectively. 12
As the strengths of this study, this was a randomized clinical trial enrolling patients who were candidates for grades 2 and 3 laparoscopic surgery. Addressing the study’s limitations, the average BMI of the subjects studied was in the normal range, and individuals with malignancies were excluded from the study.
Conclusion
The findings of this study showed that in women with benign gynecology diseases undergoing laparoscopic surgery, the two interventions of MBP and the administration of a clear liquid diet 1 day before the surgery resulted in comparable outcomes in terms of the extent of the surgical field of view and intestinal handling. Because no additional medication is imposed on the patient and less patient digestive symptoms, the clear liquid diet regimen performed considerably better; nevertheless, it is advisable to conduct more studies to investigate the efficacy of this preparation method in high-risk patients (e.g., obese, those with malignancies) undergoing laparoscopic surgery.
Footnotes
Authors’ Contributions
R.H. and P.G. contributed to design. R.H., P.G., M.R., and N.M. conducted the study. R.H. and P.G. prepared the article. M.R. analyzed the data. All authors read and approved the final article.
Availability of Data and Materials
The data sets used and/or analyzed during this study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
All authors confirm that their research is supported by the Tehran University of Medical Sciences that is primarily involved in education and research. This research received no external funding.