
Abstract
Objective:
Gynecology residents have self-reported deficits in preparation for surgical practice, particularly in robotic training. The primary source of surgical training is active participation in an operating room, which can be documented in a resident's case log. Educators and trainees may assume an institution's case volume reflects residents' participation, but there is no standard way to hold attending physicians accountable for surgical education, case-by-case. This study examined the percent of major gynecologic cases that allowed active trainee participation over 3 months at a major academic medical center.
Materials and Methods:
A baseline assessment of obstetrics/gynecology residents' participation in gynecologic surgical cases was conducted over 3 months at a large, urban academic medical center. All open and robotic gynecologic cases were recorded by the residency education team. Trainees were asked to document if a resident was present in a surgical case and that resident's level of participation in the procedure.
Results:
Of 324 open and robotic gynecologic surgeries, 74% were covered by residents. Of the 240 cases in which residents participated, 71% could be entered into clinical case logs, and 29% permitted minimal to no active participation. Thus, residents were only able to log active participation in 53% of all open and robotic gynecologic cases in the 3-month timeframe.
Conclusions:
Operative case volume at an academic medical center does not necessarily reflect resident participation and surgical training experience; there is a need to incorporate surgical-teaching skills into faculty-development programs and to emphasize the importance of active participation, case by case, in residency training further. (J GYNECOL SURG 20XX:000)
Introduction
Residents' participation in surgical cases is a widely discussed topic in the literature.1,2 To graduate from a surgical-residency program, trainees are required to cover a minimum volume of operative cases in which these residents perform as the primary surgeon. In obstetrics and gynecology training programs, a primary surgeon generally must complete at least 50% of a surgical case with minimal assistance. Operative case logs are mandated by the Accreditation Council for Graduate Medical Education (ACGME) and are tracked regularly by residency-education leadership teams. However, there are wide variations in clinical volumes and surgical participation across and within institutions. 3 Consequently, residents in many specialties have self-reported deficits in preparation for practice, particularly in surgical settings. In general surgery, residents have reported limited opportunities to operate a robotic console, and up to 92% of graduating general surgery residents report deficits in their preparation to perform common procedures independently.4,5
In the field of obstetrics and gynecology, there is a documented discordance between comfort levels for independent performance and objectives set forth by the Council on Resident Education in Obstetrics and Gynecology.6,7 Gynecology residents have self-reported deficits in preparation for surgical practice, particularly in robotic training. 8 Despite high surgical volumes of cases in major academic medical centers, obstetrics and gynecology training programs may struggle to reach the minimum requirements for major cases—such as hysterectomies and robotic surgeries. The primary source of surgical training occurs with active participation in an operating room (OR), but there is no standardized method to hold attending physicians accountable for surgical education on a case-by-case basis.
Hesitancy to allow significant resident involvement may relate to attending comfort levels, surgical complexity, or concerns surrounding longer operative times. 9 However, resident involvement in surgical cases has been demonstrated to affect outcomes for patients positively, resulting in lower mortality rates. 10 Although some evidence suggests that participation of a resident can increase operating time for low-volume surgeons, the same evidence supports minimal increases in operating time when the resident is supervised by high-volume surgeons, who are often based at major academic medical centers. 11
Given self-reported deficits in surgical training in gynecology as well as observed resident difficulty in meeting requirements for certain operative cases, the current authors sought to determine the portion of major gynecologic cases that allowed active trainee participation over a 3-month timeframe.
Materials and Methods
As part of a quality-improvement initiative, a baseline assessment of residents' participation in gynecologic surgical cases was conducted over a 3 month at a single site, a large academic medical center in New York City. From February 1, 2021, to April 30, 2021, all open and robotic-assisted gynecologic cases were recorded by the institution's obstetrics and gynecology residency education team. With the assistance of chief residents of the surgical gynecology service, trainees were asked to document if each case (1) allowed their active participation in at least 50% of the case, (2) allowed only minimal surgical participation, (3) allowed only observation, or (4) was unable to be covered by a resident. Residents were reminded to only log operative cases in their ACGME clinical case logs if they were able to participate actively in 50% of the case.
This project was approved by the New York University Obstetrics/Gynecology Quality Improvement Committee and through the Research on Medical Education Outcomes initiative. Responses were collected anonymously, and attending providers were de-identified so trends could be presented to departmental leadership at the end of the academic year.
Results
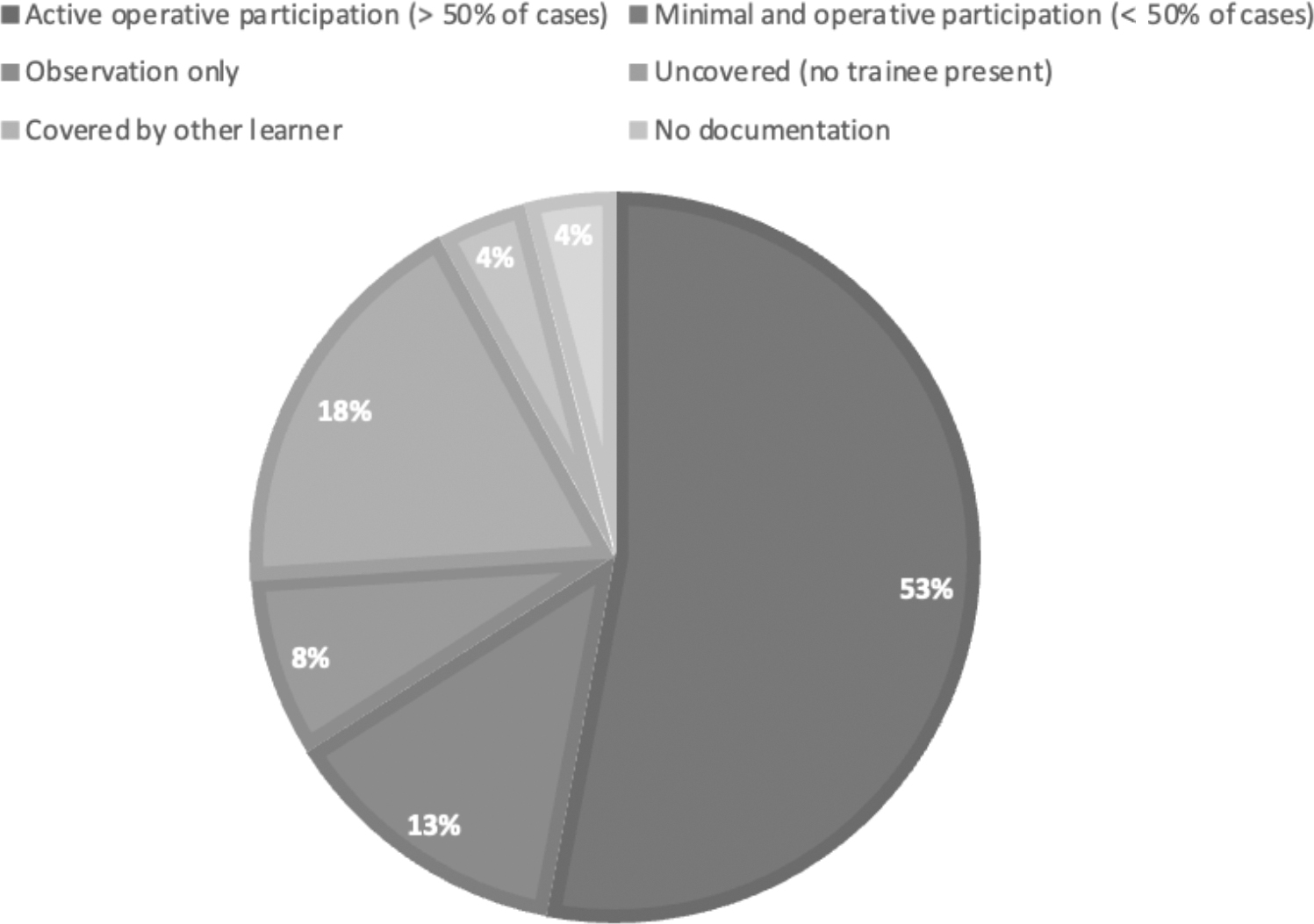
A total of 324 open and robotic-assisted gynecologic surgeries were performed at the site during the 3-month tracking timeframe. Of these surgeries, 74% were able to be covered by residents, and 18% were documented as uncovered—largely due to concurrent didactic or clinical obligations, or by attending surgeons' requests (Fig 1). Among the major cases, 4% were covered by alternative learners and not resident physicians (i.e.,: medical students or Fellows), and in 4% of cases the level of trainee participation was not recorded. Of the 240 cases in which residents were present in the OR, 71% allowed active participation and could be entered into clinical case logs, and 29% of these surgical cases covered by residents permitted minimal-to-no active participation (Fig. 2). Hence, resident trainees were only able to enter 53% of all open and robotic-assisted gynecologic surgery cases during this 3-month timeframe into their ACGME clinical case logs, with the remaining 47% of cases either uncovered by residents or permitting minimal-to-no involvement by the assigned resident (Fig. 3).
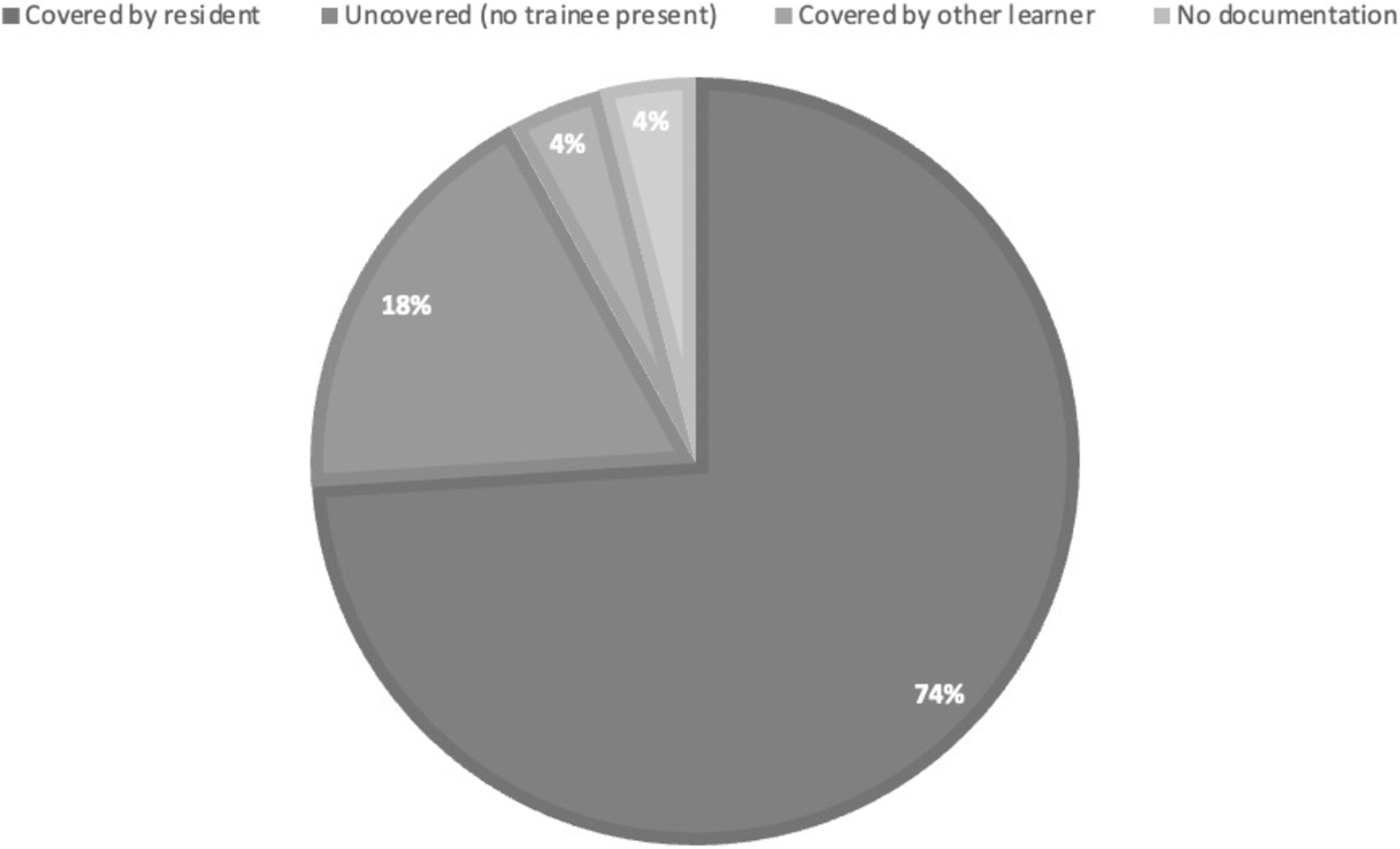
Trainees' (residents’) coverage of robotic and open gynecologic surgery cases during the specified study timeframe.

Degree of trainees' (residents’) participation in open and robotic gynecologic surgery cases covered by residents during the specified study timeframe.
Composite educational experience of trainees (residents) with respect to all robotic and open gynecologic surgery cases during the specified study timeframe.
Discussion
This baseline assessment confirmed that operative case volume at this academic medical center is not necessarily reflective of resident participation and surgical training experience. Nearly half of all open and robotic-assisted gynecologic surgery cases during the tracking timeframe were not able to be logged into residents' ACGME clinical case logs, suggesting a significant loss of surgical-training opportunities. Some of these lost opportunities occurred secondary to the absence of resident coverage. During the study timeframe, nearly ¼ of cases were not covered by residents, most commonly due to scheduling constraints including residents' didactics, concurrent clinical obligations, or by attending surgeons' requests. While protected resident didactic time is critical, hands-on learning in the OR is equally essential. Residents' didactic schedules should be considered as surgical schedules are created in order to maximize resident coverage of major elective cases with strong surgical-education potentials.
In cases when a resident was present in the OR, suboptimal trainee participation occurred in nearly 30% of major gynecologic surgeries during the study timeframe. The current study was limited with respect to the data that were collected. Thus, it was not possible to assess the rationale for a given level of resident participation, the training level of a specific assigned resident relative to the complexity of the operation, or variations in the level of resident participation permitted by different attending surgeons. Trends in teaching behaviors of attending physicians were identified and shared with division directors in order to target potential areas for improving surgical education. Educators who consistently incorporated residents into their surgical cases were highlighted, and this feedback was incorporated into their annual faculty reviews.
Given that involvement in the OR is the mainstay of surgical training, an effort must be made to maximize resident participation in cases when residents are present. As such, these results highlight the need for incorporation of surgical teaching skills into faculty-development programs. The importance of active trainee participation in surgical training must be emphasized. Surgeons who are providing this essential education, particularly at academic medical centers, should expect to incorporate the teaching of trainees into their clinical obligations and should expect to receive feedback on this metric as a part of their own performance evaluations. Furthermore, increasing opportunities for real-time, bidirectional surgical feedback may increase accountability for both surgical attendings and trainees. Providing faculty with transparent data on residents' degree of involvement in surgical cases is the first step to building context and identifying areas for improvement in surgical education.
Footnotes
Authors' Contributions
Data collection and analysis were performed by Dr. Myrick. The article's draft was by Ms. Marty. This draft was reviewed and edited by Dr. Myrick. Both authors commented on previous versions of the article, as well as reading and approving the final article.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
There was no funding provided for this research.