
Abstract
Background:
Proficiency in total laparoscopic hysterectomy (TLH) is now a requirement of all graduating Canadian Obstetrics and Gynecology (OBGYN) trainees, but despite this requirement, a recent survey discovered that residency graduates are not receiving adequate training in TLH. Educational videos have been shown to be effective in teaching procedures in other surgical disciplines.
Objective:
To create an educational video to effectively teach TLH to OBGYN trainees.
Methods:
This qualitative study was undertaken at three academic hospitals affiliated with the University of Toronto between 2016 and 2018. Seven surgical experts were interviewed and recorded performing TLH. Qualitative and thematic analysis was used to synthesize a teaching curriculum via the Delphi method. An educational video was created and shown to small groups of consenting OBGYN trainees at various levels (15). Participants completed identical pre- and post-tests to assess knowledge, and a paired t-test was used to compare qualitative scores. A detailed focus group discussion for quality improvement was conducted.
Results:
The difference between the mean knowledge test scores pre-intervention (51%) compared with post-intervention (88%) was an increase of 37% (statistically significant, p-value = 0.001, CI = 2.7–4.8). Residents felt the tool was highly effective in demonstrating anatomy, surgical techniques, and clinical pearls. All residents recommended including the video in the residency curriculum.
Conclusion:
A TLH teaching video was systematically created, incorporating techniques from multiple surgical experts, improving gynecology trainees’ knowledge surrounding surgical technique and anatomy in a safe and convenient learning environment. Trainees would recommend this tool to their peers and recommend it be incorporated into the residency training curriculum.
Introduction
Hysterectomy is the most common major gynecological surgical procedure performed worldwide, and is the second most common procedure undergone by women following caesarean section.1,2 Total laparoscopic hysterectomy (TLH) is an important approach to hysterectomy with many short and long-term benefits. A 2015 Cochrane Review found that, compared with abdominal hysterectomy via laparotomy, laparoscopic hysterectomy resulted in less blood loss, fewer incidences of fever, fewer wound infections, a shorter hospital stay and a quicker return to normal activity. 3 Due to these benefits, the Society of Obstetricians and Gynaecologists of Canada recommends the use of a minimally invasive approach to hysterectomy for benign indications compared to the abdominal approach when possible. 4 Despite these recommendations, a large proportion of hysterectomies are still being performed abdominally. A 2011 Ontario Women’s Health Equity Report found that the percentage of women who had a laparoscopic hysterectomy for benign indications ranged by region from only 30% to 63%. 5
Proficiency in total laparoscopic hysterectomy is now a requirement of all graduating Canadian OBGYN specialists, as mandated by the “Objectives of Training in the Specialty of Obstetrics and Gynecology” through the Royal College of Physicians and Surgeons of Canada. 6 Despite this requirement, a recent survey discovered that Canadian OBGYN residency graduates are not receiving adequate training in TLH. 7 Resident training in total laparoscopic hysterectomy consists mainly of studying textbooks and ad hoc education in the operating room. This deficit in skill has been attributed to the technical difficulty of the procedure and limited exposure during residency. There is a huge discrepancy in the number of total laparoscopic hysterectomies a Canadian OBGYN resident will be exposed to during their residency training, depending on the particular training program they are part of. This number is hugely variable across programs; the number of fellowship-trained minimally invasive gynecological surgeons who practice within a training site varies across the country as well. 7
Educational videos and e-modules have been shown to be effective and desirable in teaching procedures in other surgical disciplines, such as General Surgery, ENT and Plastic Surgery.8–10 No literature exists for an equivalent tool for gynecological trainees. In surgical residency programs, there is a “Three-Stage Theory” to motor skills acquisition that involves cognition (understanding the task), integration (comprehending and performing the mechanics), and automation (performing the task with speed, efficiency and precision).11,12 Educational tools such as instructional surgical videos focus on the cognition stage, by teaching the basics, such as the steps of the procedure and function of the equipment. In tandem with traditional operating room experience, these tools may be useful in order to increase comfort level among OBGYN trainees.
With declining duty hour requirements, surgical exposure in the operating room will only further decrease. The creation of a video module for trainees could accelerate the learning curve of TLH, and increase comfort level. Valuable OR time could then be reserved for refinement and mastery and not basic skill acquisition. The goal of this study was to create a video tool that will teach the TLH procedure and improve surgical skills, utilizing a combination of semi-structured interviews of identified TLH experts and video recording of surgeries.
Materials and Methods
Part 1: Creation of a surgical teaching tool
An educational video for total laparoscopic hysterectomy was methodically created to educate OBGYN trainees about the procedure. To create the learning tool, seven prominent experts in TLH were identified at three major academic centers associated with the University of Toronto OBGYN residency program (Sunnybrook Health Sciences Center, St. Michael’s Hospital, and Mount Sinai Hospital). These surgical experts were chosen for their teaching ability, based on staff and resident feedback. Once identified, each surgical expert was video-recorded performing at least one TLH and interviewed between 2016 and 2017.
The experts were given an informed consent form detailing the project and public nature of the educational tools. Once consented, the TLH patients of each expert were also given an informed consent form to have their surgery recorded, with all identifying information hidden. The surgery then was recorded through the laparoscopic camera view using the operating room camera system. In conjunction, an audio recording of the expert surgeon was obtained, while asking pointed questions about each key step during the surgery, important aspects of patient selection, pitfalls normally encountered by trainees, parts of the procedure that can pose a challenge, and their preferred strategies and techniques for learning and performing the surgery. All data were collected and stored on encrypted USB keys and external hard drives. The audio recordings were then transcribed.
The video-recording and audio interview from each surgeon was then analyzed for common themes using thematic analysis until saturation of themes was determined. A written document that summarized these findings was then sent to all experts for review. This final document was a collection of all the knowledge, lessons, and techniques that the experts identified as essential for teaching how to perform a TLH. Comments on the document from each expert were then reviewed and consensus regarding what to include in the instructional video was reached via the Delphi method. A recently published Delphi consensus of the key steps of TLH was used as a framework to build this educational tool. 13 The video was 20 minutes in length and was created using Adobe Premiere (See Fig. 1).

Creating a Surgical Teaching Tool.
Part 2: Evaluation of the surgical teaching tool
A focus group of OBGYN trainees from all levels was recruited and consented to trial the final educational tool between 2017 and 2018. Each focus group consisted of 4–6 individuals, with each discussion lasting approximately 45–60 minutes. A minimum of 10 participants total in groups of 5–6 has traditionally been found to be an ideal number for focus groups to ensure the maximal participation and feedback. 14
In order to test the success of this teaching video, two measures were utilized: a focus group and assessment of improvement in knowledge related to TLH. The validity of the educational tool was evaluated through focus groups and both qualitative and quantitative surveys. Participants took a TLH knowledge pre-test, comprised of questions derived from the interviews of surgical experts on topics such as patient selection, steps of a TLH, relevant anatomy, and pertinent tips and tricks. Afterwards, they were exposed to the video, and subjected to an identical post-test and qualitative survey of the educational tool. Questions within the survey included common demographic information such as age and residency training level, their opinions on the effectiveness of the tool, the length of the tool, and their comfort level in performing a TLH (Supplementary Appendix SA1, SA2).
Continuous variables were collected of pre- and post-test scores, and were analyzed using a paired t-test to assess for the educational tool’s effect on scores. Secondary outcomes analyzed were qualitative factors such as satisfaction with the educational tool, length of the tool, and applicability to their training. (See Fig. 2).
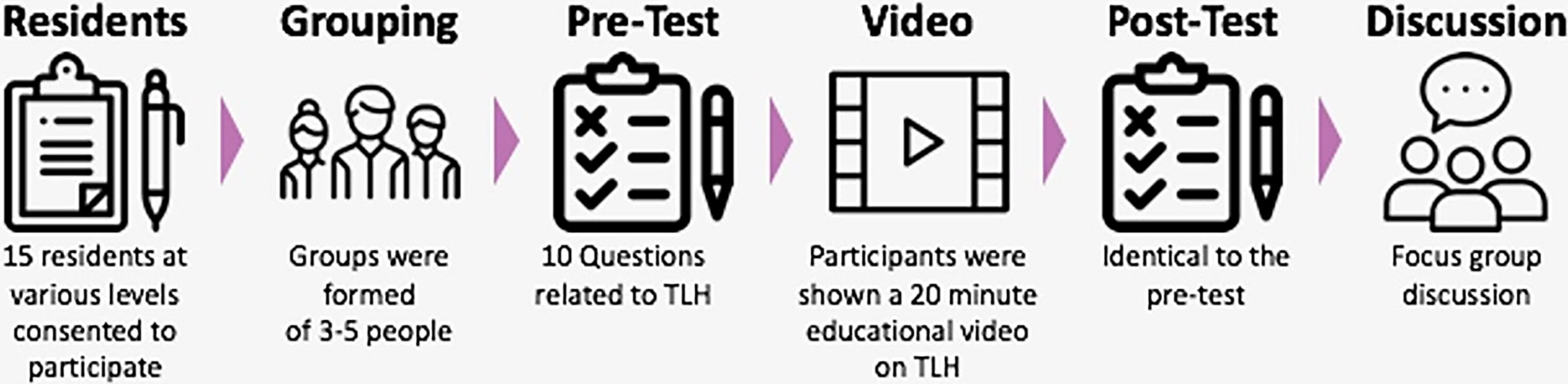
Evaluating a Surgical Teaching Tool.
IRB approval from Sunnybrook Health Sciences Center, #321–2015
Results
Fifteen postgraduate trainees consented to participate (Table 1)
Knowledge test scores
The quantitative results of our study showed that residents’ overall knowledge significantly improved after watching the video teaching tool. The mean knowledge test score pre-intervention was 5.1/10 (51%). The mean knowledge test score post-intervention was 8.8/10 (88%). The difference between the mean knowledge test scores pre-intervention compared with post-intervention was 3.7/10 (37%), which was statistically significant (p-value = 0.001, CI = 2.70–4.77). See Figure 3.
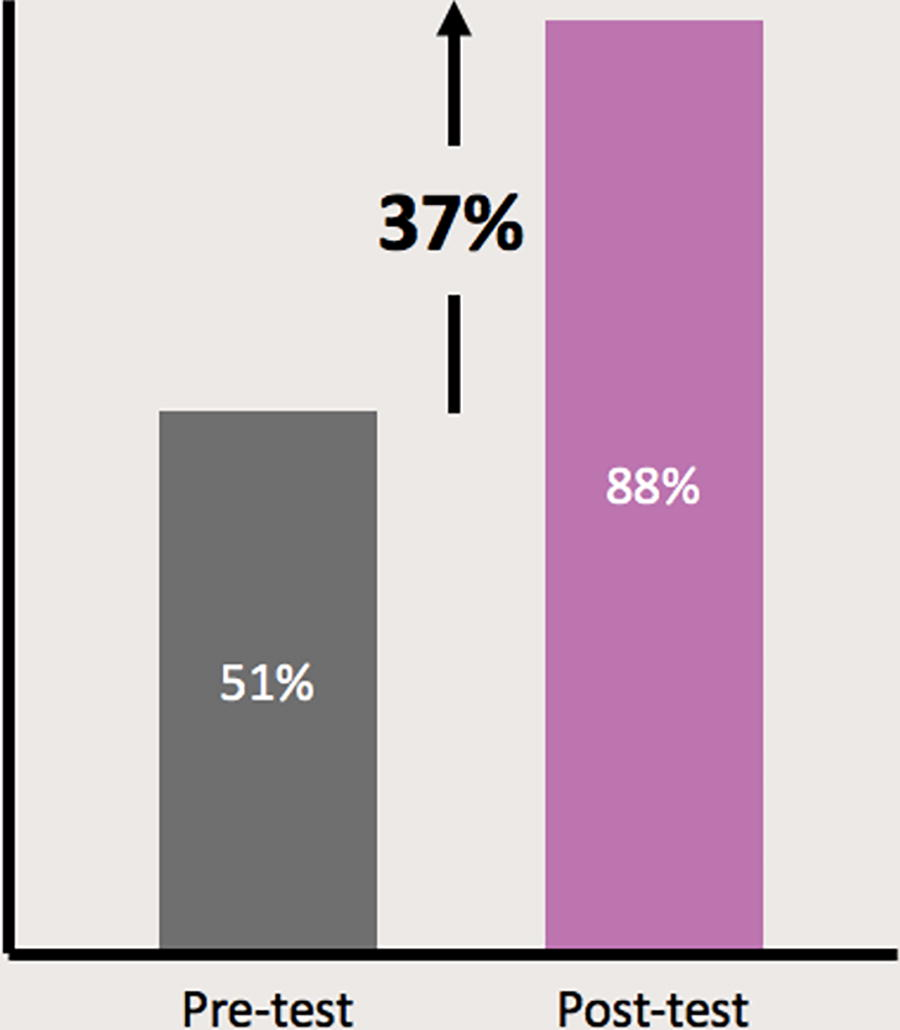
Difference between the mean knowledge test scores pre-intervention versus post-intervention.
Focus group discussion results
Through focus group discussion, residents were able to express that they felt the tool was highly effective in demonstrating anatomy, surgical techniques, and clinical pearls relevant to TLH.
All residents (15/15, 100%) agreed that they would recommend including the video tool in the residency program curriculum. All residents (15/15, 100%) also agreed that they would recommend this video to their resident peers. Most residents (12/15, 80%) were completely satisfied with the length and depth of the video. A total of 2/15 (13%) residents wanted the video to be 5 minutes shorter in length. A total of 1/15 (7%) residents thought it should be longer in length to include more detail. Residents wanted to see more detail on ureterolysis, retroperitoneal dissection, and alternative port placement, but suggested this could also be the focus of a future teaching video.
The data from all focus groups was analyzed and compared for consensus between all focus groups. The highlights of what all residents agreed upon pertaining to what they liked and suggestions for improvement can be found in Table 2.
Areas of Strength/Improvement
TLH, total laparoscopic hysterectomy.
Discussion
TLH is one of the most technically challenging procedures that a trainee in gynecological surgery will learn throughout their residency. This project was initially devised to offer a solution to the issue that many new Canadian OBGYN graduates did not feel competent to perform a TLH at the end of their residency training program. 7 Residency training in OBGYN in Canada has traditionally been 5 years in length, although this may change in the era of competency-based training, which was implemented as of July 1, 2019 by the Royal College of Physicians and Surgeons of Canada to all new OBGYN resident trainees. 15 This shift towards competency-based skill acquisition reflects the growing emphasis on outcomes-based surgical education. 16 Over this finite period, trainees must not only become competent performing gynecological surgery procedures, but also master obstetrical skills and become proficiently trained in all the related OBGYN subspecialties (maternal fetal medicine, gynecological oncology, reproductive endocrinology, urogynecology, pediatric, and adolescent gynecology). 6
Minimally invasive surgical techniques have become more of a norm within the specialty of gynecological surgery, leading to better patient outcomes. 3 In a climate of decreased clinical exposure, it is essential to modify and optimize our current teaching models to set our trainees up for success, allowing for the acquisition of such techniques prior to the end of residency training. 16 A systematic review by Ahmet et al. indicated that video-based education is effective and has significant potential for use in surgical education, suggesting the use of videos in addition to the standard traditional surgical education techniques. 17
Our study found the surgical teaching video our team created was able to improve knowledge related to TLH. If trainees are well versed in the relevant knowledge related to the procedure prior to entering the operating room, this may allow for more opportunity for hands-on procedural training. According to a study of general surgery trainees by Crawshaw et al., watching a brief instructional video prior to performing a surgery may improve the learning curve of trainees and improve safety. 18 In another study of general surgery trainees by van Det et al., it is reported that educational videos in addition to conventional education through a master-apprentice model improved learning, enhanced technical skill development during the early learning curve, and cost very little extra time. 19 Solidifying knowledge related to the procedure and relevant anatomy prior to entering the OR helps trainees build confidence and appear more prepared. This could result in decreased intraoperative time for teaching technical skills versus basic didactic knowledge. The operating room has often been called a “costly, high-risk classroom,” but surgeons feel more at ease and allow for more trainee participation when trainees are prepared. 20
The parts of the video residents valued most in this study were the organized review of the key steps of the procedure, condensed high-yield information including relevant anatomy and clinical pearls, and the ability to visualize different techniques to perform the same surgery. This is similar to findings from literature pertaining to plastic surgery education, which supports organized videos that clearly delineate steps of the procedure, meaningful pauses to highlight difficult steps, and highlighting key anatomy with arrows or legends. 21 These are important considerations in planning future educational videos.
One of the main strengths of this study is the meticulous methodology used to create this clinical teaching tool. A rigorous, systematic approach was used to create a validated tool to teach the important steps of TLH to our trainees. The video we created itself is high quality and truly a collaboration of the expertise of multiple surgical experts within our department. The video is presented in a concise, easy-to-follow format with logical flow. The video itself shows multiple different approaches to each step of the procedure. It also demonstrated different types of equipment that can be appropriately used to achieve the same purpose within surgery. One final strength of this study is the acceptability of the teaching tool by our trainees. All trainees interviewed wanted this video incorporated into the residency teaching curriculum and there appears to be a demand for similar videos to teach other surgical procedures in the future. The satisfaction with video-based teaching exhibited by our own trainees is similar to that described in other surgical disciplines.17–19
The limitations of our study were that we did not incorporate an objective surgical assessment of technical skills into this project to determine if our intervention resulted in an improvement in surgical performance. Given the difference in the level of study participants (PGY 2–5 residents), it was not possible to determine an objective scoring system to equally evaluate all levels in the timeframe allotted to carry out this research study. In addition, staff gynecologists were not comfortable with the autonomy such a study would require for the more junior residents involved. The teaching video could have been further subdivided to determine if certain portions were more beneficial than others. This could have been assessed via pre/post-test analysis or through feedback elicited from focus groups, and is a consideration for future studies. A future direction would be surgical evaluation of the trainees before and after watching this video tool. Another limitation is that our study did not assess maintenance of knowledge gained from watching the instructional video. Another future direction would be to evaluate the ongoing use of the video within the residency curriculum and to determine if the knowledge gained was retained by trainees. We would also like to evaluate the use of this video among practicing gynecologists trying to advance their surgical skills and learn TLH. This could be used and evaluated at formal continuing medical education events in order to streamline knowledge translation.
We plan to include this teaching video into the University of Toronto OBGYN residency curriculum and make it easily accessible and readily available to trainees as an online resource. We would also be willing to make our video available to other training programs nationally and internationally. Ideally, a central educational video library for trainees made up of high quality systematically created videos could be generated. There is a need for updated teaching methods within our specialty, that are systematically created to incorporate multiple styles and techniques for carrying out difficult surgical procedures, especially in keeping with the unique needs of this current generation of trainees. Given the positive response to this video, we hope to create similar video tools to effectively teach other gynecological surgical procedures and techniques to enhance the educational curriculum. The steps used to create this video could act as a framework for future work.
Conclusion
A robust video-based educational tool was methodically created to teach OBGYN residents to perform a total laparoscopic hysterectomy, incorporating techniques from multiple surgical experts from the three academic gynecological teaching hospitals in Toronto. This tool improved gynecological trainees’ knowledge surrounding surgical technique and anatomy pertaining to TLH. Trainees would recommend this tool to their peers and recommend it should be incorporated into the residency training curriculum.
Research Ethics Board Approval
IRB approval received from Sunnybrook Health Sciences, Sept 10, 2015, #321–2015.
Precis
An educational video that was collaboratively and systematically created to teach Total Laparoscopic Hysterectomy was shown to improve overall knowledge scores and was well-received by trainees.
Footnotes
Authors’ Contributions
C.McC.: Conceptualization, methodology, investigation, resources, data curation, writing—original draft, writing—review and editing, visualization. B.L.: Conceptualization, methodology, investigation, resources, writing—review and editing. G.Y.L.: Conceptualization, resources, writing—review and editing. R.K.: Conceptualization, resources, writing—review and editing. H.W.: Conceptualization, resources, writing—review and editing. A.S.: Conceptualization, resources, writing—review and editing. S.K.: Conceptualization, resources, writing—review and editing. J.S.: Conceptualization, resources, writing—review and editing. A.S.: Conceptualization, resources, writing—review and editing. J.K.: Conceptualization, methodology, resources, data curation, writing—review and editing, supervision.
Author Disclosure Statement
There are no conflicts of interest.
Funding Information
Ontario AHSC AFP Innovation Funding Grant Sunnybrook Health Sciences Center.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.