
Abstract
Objectives:
To evaluate the prevalence of polyp findings in office endometrial biopsies, estimate the incidence of endometrial polyps on diagnostic evaluation, and to describe demographic and clinical characteristics associated with these findings.
Materials and Methods:
We conducted a retrospective chart review of 7073 patients undergoing an endometrial biopsy between January 1, 2015 and December 31, 2019. We collected demographic data, clinical characteristics, and findings at diagnostic workup. Bivariate analysis was performed to compare demographic and clinical characteristics between patients with and without a clinically identifiable polyp and stratified analysis was performed according to menopausal status. Patients with hyperplasia, premalignancy, or malignancy were described.
Results:
Among endometrial biopsies performed during the study period, 10.2% (n = 719/7073) were reported to have polyp findings. Further diagnostic evaluation was pursued in 33.4% (n = 240/719) with hysteroscopy or hysterectomy. Among those with diagnostic procedures performed, 70.4% (n = 169/240) had a clinically identifiable polyp at the time of the procedure or on pathological specimen report. Patients with clinically identifiable polyps were more often postmenopausal (71.6% vs. 21.1%, p < 0.001), age 55 or older (63.3% vs. 18.3%, p < 0.001), had a history of hypertension (42.0% vs. 28.2%, p = 0.04), or current or prior tamoxifen use (11.2% vs. 2.8%, p = 0.04) compared with patients without clinically identifiable polyps. Patients with clinically identified polyps more often had initial endometrial biopsy pathology reports stating “endometrial polyp” (p < 0.001) and had undergone endometrial biopsy for postmenopausal bleeding (p = 0.04). Stratified analysis in postmenopausal patients demonstrated confirmed polyp in 88.9% (n = 121/136) of cases, with 8.8% (n = 12/136) of patients demonstrating hyperplasia and premalignant or malignant findings.
Conclusions:
Approximately 1 in 10 endometrial biopsies report polyp findings. Further diagnostic evaluation should be considered when an endometrial biopsy indicates polyp, particularly in postmenopausal patients, given the high probability of a clinically identifiable polyp, hyperplasia, and premalignant or malignant findings.
Introduction
Accurate detection of endometrial polyps is important in the assessment of many gynecological conditions including abnormal uterine bleeding and infertility. Endometrial polyps are also associated with premalignant or malignant findings in 4.9% to 5.5% of postmenopausal patients and 1.1% to 1.7% of premenopausal patients.1–3 When an endometrial biopsy reports findings consistent with “polyp,” it is unclear if further investigation is warranted and no standard guidelines exist for this common clinical question.
Endometrial polyps are characterized by a combination of irregular endometrial gland architecture, fibrotic or otherwise altered stroma, and presence of thick-walled vessels; it can be challenging to definitively meet these histological criteria with a biopsy sample that contains only small tissue fragments.4,5 A range of outcomes are seen at the time of more definitive assessment including heterogeneous endometrium, discrete polyp, and premalignant or malignant tissue. The heterogeneity of findings upon further workup leaves gynecologists without clear management recommendations. Hysteroscopy is the gold standard for identification of endometrial polyps, but it remains unclear if this is universally indicated based on endometrial biopsy findings.6–7
Given challenges in polyp identification and lack of standard guidance for management, we performed a retrospective chart review (1) to determine the prevalence of polyp findings in endometrial biopsies, (2) to describe the incidence of clinically identifiable polyps upon further diagnostic workup, and (3) to evaluate demographic and clinical characteristics associated with endometrial polyps, hyperplasia, and malignancy in patients with polyp findings on an endometrial biopsy.
Methods and Materials
We performed a retrospective chart review of patients aged 18 or older who underwent an endometrial biopsy at our institution between January 1, 2015, and December 31, 2019, under institutional board approval (E-20-864). Further chart review was performed for all patients for whom the endometrial biopsy pathology report mentioned polyp findings. This included reports stating: “polyp,” “fragments of polyp,” “suggestive of polyp,” “possible polyp,” “features consistent with polyp,” and “polypoid.” All endocervical polyps (n = 113) were excluded from further analysis as these are composed of endocervical glands rather than endometrial glands. Given endocervical polyps are a distinctly different pathological entity, the risk of endometrial atypical hyperplasia, endometrioid intraepithelial neoplasia, or serous endometrial intraepithelial carcinoma is negligible. Dysplasia or carcinoma within endocervical polyps is rare and is typically related to human papillomavirus. 8 All endometrial biopsies with diagnosis of complex atypical hyperplasia or malignancy were also excluded, even if there was a separate mention of polyp findings.
All patients with polyp findings on endometrial biopsy were investigated. A manual chart review was completed examining outpatient clinic notes, the preoperative history, and physical, operative notes and pathology reports. We collected covariates of interest such as age, race, body mass index (BMI), and smoking status. Race was patient-reported and categorized into two groups: White and non-White. Reported risk factors for endometrial polyps were reviewed, including history of polyp, history of hypertension, history of or current use of tamoxifen, history of or current use of postmenopausal hormone therapy and menopausal status. We defined menopause as the absence of menses for >12 months. We were unable to adequately assess premenopausal versus perimenopausal status based on chart review, so all patients who were not classified as menopausal were considered premenopausal in this analysis. Finally, we evaluated clinical factors, such as initial indication for endometrial biopsy and the wording in which polyp findings were reported on initial endometrial biopsy pathology. Given the variable description of polyp findings on initial endometrial biopsies, pathology was categorized into four groups: endometrial polyp only or both endometrial and endocervical polyp; fragments of polyp; nonspecific or possible polyp; or polypoid. Further workup was divided into two categories: nondiagnostic and diagnostic. Nondiagnostic evaluation included procedures that were not able to visualize the entire endometrial cavity such as repeat endometrial biopsy or dilation and curettage. Diagnostic evaluation included hysteroscopy findings or hysterectomy specimen analysis.
We analyzed all variables using descriptive statistics. The normality of BMI was assessed by inspecting skewness and kurtosis, and the Shapiro-Wilk test, and expressed using median and interquartile range. We performed bivariate analysis to compare demographic and clinical characteristics between patients with and without clinically identifiable polyps. Comparisons between non-normally distributed variables were performed using Wilcoxon rank test and chi square or Fisher’s exact test for categorical variables. Data were missing for indication for endometrial biopsy (n = 13) and not included in statistical comparisons. Demographic and clinical factors were then analyzed in the context of premenopausal and postmenopausal status as gathered from the clinician notes prior to initial endometrial biopsy. Patients with hyperplasia and premalignant or malignant findings at the time of follow-up evaluation with either hysteroscopy or hysterectomy were described using select demographic and clinical follow-up information. Hyperplasia within a polyp was not considered pathological as polyps tend to be less hormone-responsive and have irregularly distributed glands with areas of crowding at baseline.9,10 Hyperplasia in the surrounding endometrium was recorded and any atypia and/or complex hyperplasia was classified as a premalignant lesion. All data management and analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, N.C.) and statistical significance was assessed using p < 0.05.
Results
A total of 7073 endometrial biopsies were performed during the study period with 832 reporting polyp findings. Polyp findings were reported in a variety of ways within the pathology report, with “endometrial polyp” (44.5%) and “fragments of polyp” (29.7%) being the most common (Table 1).
Initial Endometrial Biopsy Findings (n = 832)
Includes “possible polyp,” “suggestive of,” and “features consistent with.”
Patients with endocervical polyps alone were excluded (n = 113) from further analysis (Fig. 1). A total of 719 biopsies reported endometrial polyp findings with an incidence of 10.1% (n = 719/7073). Of those with endometrial polyp findings on endometrial biopsy, 43.4% (n = 312/719) underwent further evaluation. However, only 33.3% (n = 240/719) of patients underwent further diagnostic evaluation for polyps with hysteroscopy or hysterectomy. Based on review of the operative note and pathology report, 70.4% (n = 169/240) of patients who underwent diagnostic evaluation were found to have a clinically identifiable polyp. Polyps were more commonly identified after hysteroscopy than hysterectomy (84.5% vs. 33.3%, p < 0.001).
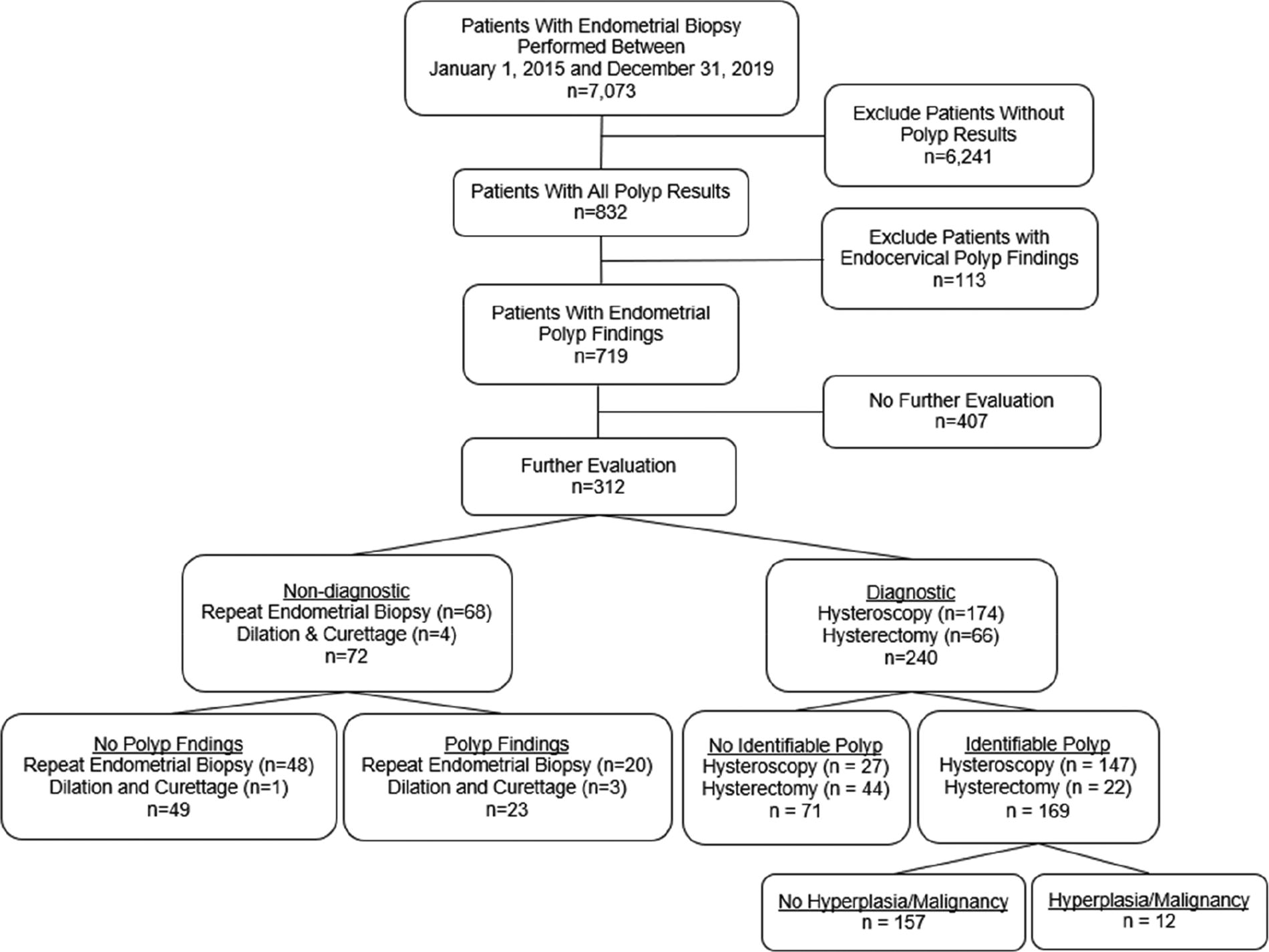
Flowchart of analytic sample selection.
An additional 10.0% (n = 72/719) of patients underwent additional nondiagnostic evaluation, including 9.5% (n = 68/719) with repeat endometrial biopsy and 0.6% (n = 4/719) with dilation and curettage. With repeat nondiagnostic tissue sampling, 31.9% (n = 23/72) had persistent pathology findings indicating endometrial polyp.
Compared with patients who did not have clinically identified polyps on diagnostic evaluation, patients with clinically identified polyps were more often postmenopausal, age 55 or older, had a history of hypertension, and a history of current or prior tamoxifen use (Table 2). Patients with clinically identified polyps also more often had “endometrial polyp” only or both “endometrial and endocervical polyp” reported on initial endometrial biopsy pathology and had undergone endometrial biopsy for indication of postmenopausal bleeding. Menopausal-specific stratified analysis was performed (Table 3) and there were no statistically significant differences except for age, which clearly correlates with menopausal status.
Demographic and Clinical Characteristics of Patients with Initial Endometrial Biopsy Results Indicating Polyp
Data are presented as n (%) unless otherwise specified. Data are missing for indication for endometrial biopsy (n = 13).
Data are presented as median (interquartile range).
Wilcoxon rank test.
Fisher’s exact test.
Includes diagnoses of pelvic pain, infertility, incidental ultrasound findings, abnormal pap smear, and pelvic mass.
Includes “possible polyp,” “suggestive of,” and “features consistent with.”
AUB, abnormal uterine bleeding.
Demographic and Clinical Characteristics of Patients with Nonspecific Endometrial Biopsy Findings by Menopausal Status
Data are presented as n (%) unless otherwise specified.
Fishers exact test.
Data are presented as median (interquartile range).
Wilcoxon Rank test.
Data are missing for indication for endometrial biopsy (n = 13).
Includes encompassed diagnoses like pelvic pain, infertility, incidental ultrasound findings, abnormal pap smear, and pelvic mass.
Includes “possible polyp,” “suggestive of,” and “features consistent with.”
Includes complex atypical hyperplasia or atypical hyperplasia.
In postmenopausal patients who had an initial endometrial biopsy result indicating polyp, 8.8% (n = 12/136) had a more advanced pathological finding than benign polyp on diagnostic workup. These findings included hyperplasia (n = 3), hyperplasia with atypia (n = 1), complex atypical hyperplasia (n = 3), or malignancy (n = 5). All of these patients had presented with postmenopausal bleeding, and four had either current or prior use of tamoxifen (Table 4).
Patients with Hyperplasia, Premalignancy, or Malignancy (n = 12)
BMI, body mass index; Both, both endometrial and endocervical polyp; EMB, endometrial biopsy; Endo, endometrial polyp; Fragment, fragments of polyp; HT, hormone replacement therapy; HTN, hypertension; PMB, postmenopausal bleeding.
Discussion
In our study, approximately 1 in 10 endometrial biopsies described findings consistent with endometrial polyp, and the description of histological findings was fairly heterogeneous. Similarly, clinical management varied widely, reflecting the current lack of standard guidelines or management recommendations. Only one-third of patients with a polyp finding underwent diagnostic evaluation with hysteroscopy or hysterectomy. When further diagnostic evaluation was pursued, the majority (70.4%) of patients did have a clinically identifiable polyp. Notably, the proportion of patients who had confirmed polyp diagnosis was significantly higher among those who underwent diagnostic compared with nondiagnostic (70.4% vs. 31.9%, p < 0.001) evaluation following initial biopsy results, likely reflecting a missed opportunity for confirmation of endometrial polyp with nondiagnostic evaluation. This study was performed prior to incorporation of office hysteroscopy at our institution. With the advent of widespread access to office hysteroscopy, low procedure-associated risk, and minimal recovery, direct visualization seems especially prudent when polyp findings are reported on an endometrial biopsy.
Postmenopausal status was the most significant risk factor for the presence of clinically identified polyps. In fact, diagnostic evaluation confirming the presence of endometrial polyps was substantially greater in postmenopausal (88.9%) compared with premenopausal patients (46.2%), (p < 0.001). This is consistent with prior data indicating higher prevalence of endometrial polyps in postmenopausal patients. 11 Additionally, all of the cases of hyperplasia or carcinoma in our study were identified in postmenopausal patients. In this study, 8.8% (12/136) of postmenopausal patients were found to have hyperplasia and premalignant or malignant findings upon diagnostic evaluation of an endometrial biopsy that initially reported benign polyp. Notably, 7.4% (9/121) of postmenopausal patients with a clinically identifiable polyp demonstrated premalignant or malignant findings, which is higher than the rate described in existing literature.1–3 Together, these findings indicate that endometrial biopsy results reporting polyp in postmenopausal patients may warrant additional diagnostic evaluation given the high probability of confirmed polyp and the risk of hyperplasia, premalignancy, or malignancy.
Pathology reports stating “endometrial polyp” only or both “endometrial and endocervical polyp” were associated with a higher likelihood of finding a clinically identifiable polyp, compared with reports stating “fragments of polyps, suggestive of polyps, or polypoid.” This “hedging” is understandable when considering the many gray areas of pathology interpretation, particularly in the setting of fragmented endometrial biopsies. Nevertheless, clinicians attempting to interpret these results would likely benefit from more standardized terminology.
The likelihood of finding a clinically identifiable polyp may be understated in this study and this is an important limitation. The incidence of clinically identifiable polyps was significantly increased for hysteroscopy compared with hysterectomy procedures. It is possible that the presence of a polyp was not reported in all hysterectomy specimens and polyps may have been harder to identify after uterine manipulator placement or morcellation. Given this was a retrospective cohort study, we cannot ensure the completeness or accuracy of operative and pathology reports or clinic documentation. This study was also limited to a single institution, and these practice patterns may not apply to other health systems or geographic regions. Further diagnostic evaluation and treatment with hysteroscopy or hysterectomy may have been more commonly pursued in patients with more concerning clinical symptoms such as heavy or persistent bleeding or abnormal ultrasound findings; thus, falsely increasing the incidence of clinically identifiable polyps, hyperplasia, and malignancy. Presence of multiple polyps and polyp size was initially extracted as part of our chart review but omitted from the final analysis owing to missingness. Measurements of polyp number and size were rarely recorded in the operative descriptions and follow-up pathology reports. Strengths of this study include a large cohort of endometrial biopsies obtained over 5 years. Our data collection was able to examine many factors previously described as risk factors for endometrial polyps. A prospective study is needed to clarify these findings.
Conclusions
We found that diagnostic evaluation following an endometrial biopsy reporting polyp findings was highly likely (70.4%) to result in confirmation of an endometrial polyp, particularly in patients who were postmenopausal, had a history of hypertension, a history of current or prior tamoxifen use, and had “endometrial polyp” reported as the initial endometrial biopsy pathology. Furthermore, our findings demonstrated a higher than expected probability (8.8%) of detecting hyperplasia, premalignancy, or malignancy at the time of diagnostic evaluation in postmenopausal patients with initial endometrial biopsy reporting polyp. Together, these findings may indicate that postmenopausal patients warrant diagnostic evaluation and definitive pathological diagnosis in response to endometrial biopsy results indicating polyp.
Authors’ Contributions
E.L.M.: Conceptualization (equal), data curation (supporting), formal analysis (equal), funding acquisition (equal), investigation (equal), project administration (equal), resources (equal), software (equal), supervision (equal), validation (equal), visualization (equal), writing—original draft (lead), writing—review and editing (equal). A.E.: Conceptualization (equal), data curation (lead), formal analysis (supporting), funding acquisition (equal), investigation (equal), project administration (equal), resources (equal), software (equal), supervision (supporting), validation (equal), visualization (equal), writing—original draft (supporting), writing—review and editing (equal). E.K.K.: Conceptualization (equal), data curation (equal), formal analysis (lead), funding acquisition (supporting), investigation (equal), project administration (supporting), resources (supporting), software (supporting), supervision (supporting), validation (equal), visualization (supporting), writing—original draft (equal), writing—review and editing (equal). S.L.S.: Conceptualization (supporting), data curation (supporting), formal analysis (supporting), funding acquisition (supporting), investigation (equal), project administration (supporting), resources (supporting), software (supporting), supervision (supporting), validation (supporting), visualization (supporting), writing—original draft (supporting), writing—review and editing (equal). K.O.: Conceptualization (supporting), data curation (supporting), formal analysis (supporting), funding acquisition (supporting), investigation (equal), project administration (supporting), resources (supporting), software (supporting), supervision (supporting), validation (supporting), visualization (supporting), writing—original draft (supporting), writing—review and editing (equal). S.R.T.: Conceptualization (equal), data curation (supporting), formal analysis (equal), funding acquisition (supporting), investigation (equal), project administration (supporting), resources (equal), software (equal), supervision (equal), validation (equal), visualization (equal), writing—original draft (equal), writing—review and editing (equal).
Footnotes
Data Availability
All data are available for review upon request.
Author Disclosure Statement
The authors do not have any conflicts of interest to declare.
Funding Information
No funding was received for this article.