
Abstract
Introduction:
The fundamental approach to managing advanced epithelial ovarian cancer (EOC) involves optimal cytoreductive surgery (CRS) coupled with platinum-based chemotherapy. Despite this, index surgeries often miss potential disease-harboring sites, resulting in incomplete or “pseudo-complete” cytoreduction and early pseudo-recurrences, essentially a residual disease.
Materials and Methods:
A prospective observational study was conducted at the Department of Surgical Oncology, AIIMS, New Delhi, India, from 2012 to 2022. This study included 250 patients with stages III–IV ovarian cancer who had undergone prior surgery at other centers and required additional cytoreductive surgery. The aim was to identify residual disease sites and correlate operative records from previously documented optimal CRS with intraoperative findings at our oncologic center.
Results:
The bladder peritoneum, porta hepatitis, retrohepatic peritoneum, lesser omentum, and retroperitoneum were the most prevalent sites of residual disease. Significant agreement (kappa coefficient 0.61–0.80) was observed between documented operative records from other centers and our intraoperative findings for procedures like hysterectomy, bilateral salpingo-oophorectomy, and infracolic omentectomy. Moderate agreement (0.41–0.60) was noted for subdiaphragmatic peritonectomy, pelvic nodal dissection, and bladder peritonectomy, with fair agreement (0.21–0.40) for supracolic omentectomy, pouch of Morrison peritonectomy, lesser omentum omentectomy, and para-aortic lymph node dissection. Achieving no gross residual disease required standard cytoreductive procedures in 56% of patients, radical resections in 17%, and ultraradical surgery in 27%.
Conclusion:
Patients with advanced EOC benefit from complete CRS involving more aggressive resections. Training for surgeons should emphasize avoiding “pseudo-cytoreduction” to enhance overall patient outcomes.
Introduction
Globally, ovarian cancer ranks as the third most prevalent gynecological malignancy, 1 with high-grade serous epithelial carcinoma emerging as the predominant histopathological type. 2 The late-stage diagnosis of ovarian cancer contributes to its formidable lethality, as evidenced by a meager 5-year survival rate of 17% for patients at advanced stages. The cornerstone of managing this malignancy lies in cytoreductive surgery (CRS), followed by adjuvant chemotherapy. Advanced epithelial ovarian cancer (EOC) is characterized by peritoneal spread, often concealed on preoperative imaging, necessitating a comprehensive exploration of the entire abdominal cavity during surgery to identify all disease sites.3,4 Hence, we introduce the term “pseudo cytoreduction” (PCRS) to describe a situation where inadequate assessment of disease sites within the abdomen results in suboptimal surgery for women with advanced EOC. This inadequate surgery consequently compromises patient survival.5–7
Materials and Methods
From 2012 to 2022, the Department of Surgical Oncology at Dr. B.R.A. Institute Rotary Cancer Hospital, AIIMS, New Delhi, conducted a prospective clinical observational study. The study has been approved by the ethics committee of the AIIMS, New Delhi.
Inclusion criteria
EOC of stages III–IV.
Documented optimal cytoreduction at another center with comprehensive operation records.
Disease confined to the peritoneal cavity within 1 year of completing treatment.
Candidates for cytoreductive surgery following a multidisciplinary tumor board discussion.
Exclusion criteria
Poor performance status (unoptimized Eastern Cooperative Oncology Group Performance Score 2 or above).
Unwillingness for surgery.
Multidisciplinary decision for systemic chemotherapy only.
The review encompassed patient files, examining details of surgical procedures performed elsewhere, pre-referral chemotherapy, treatment completion date, and post-surgery imaging. At our center, histopathology blocks were reassessed, CA 125 was measured, and radiological imaging contrast-enhanced computed tomography (CECT abdomen and pelvis with/without chest) was repeated. Discrepancies between reported operative findings and disease burden on CECT were identified. After a multidisciplinary tumor board discussion, patients requiring further cytoreductive surgery were included, with heated intraperitoneal chemotherapy performed selectively according to the institute’s policy. During laparotomy, residual disease sites were documented and photographed, highlighting disparities between findings from the initial outside surgery and operative results at our center. Some patients underwent extensive resections to achieve complete cytoreduction, with the complexity of CRS classified as standard, radical, or ultraradical. Standard procedures typically include hysterectomy, oophorectomy, pelvic, and para-aortic lymphadenectomy, and both lesser and greater omentectomy, along with disease-specific peritonectomy. Radical cytoreductive surgery may involve total parietal peritonectomy, visceral peritoneal resection (including the mesentery), anterior or low anterior resection, Glisson capsule resection, resection of up to 1.5 m of small bowel, hemicolectomy, distal gastrectomy, cholecystectomy, and appendectomy. Ultraradical procedures further extend to diaphragmatic resection, segmental or wedge liver resection, splenectomy (with or without distal pancreas removal), multiorgan resection, cardiophrenic lymph node removal, and pleurectomy. Post-surgery, enhanced recovery after-surgery protocols were adhered to, following the institute’s guidelines. Follow-up involved clinical examinations and imaging to discern patterns and sites of recurrence.
Results
This study incorporated data from 250 patients diagnosed with stages III–IV EOC, who were referred to our institute between January 2012 and December 2020 following surgeries conducted elsewhere. The predominant stage among these patients was IIIc, constituting 78.8% of the cases. Based on operative records, 88.4% (221) had undergone optimal cytoreduction before referral, with 70.8% (177) having primary cytoreductive surgery and 29.2% (73) undergoing interval cytoreductive surgery after neoadjuvant chemotherapy. Demographic details of the study population are presented in Table 1.
Demographic Profile of Study Population
As determined from operative records.
CRS, cytoreductive surgery; NACT - Neoadjuvant Chemotherapy.
All patients included in the study exhibited evidence of disease on imaging after referral to our center, leading to surgical re-exploration. The duration between imaging (CECT) and the second surgery was on average 6–8 weeks because of the high volume. The mean interval between primary and completion surgery was 4 months. Of these, 40% of patients received chemotherapy before the second cytoreductive procedure—usually after two cycles of paclitaxel and carboplatin, which we considered as interval cytoreductive surgery, not as secondary. In these patients, the average duration of time between chemotherapy and the second cytoreductive procedure is 3.3 months. The mean tumor size at the time of the second surgery was 2.5 cm (1–6 cm). The comparison of our intraoperative findings with the initial treating center’s operative records revealed the degree of agreement, as assessed by Cohen’s kappa, as follows:
Substantial agreement (0.61–0.80) for a total hysterectomy, bilateral salpingo-oophorectomy, and infracolic omentectomy. Moderate agreement (0.41–0.60) for subdiaphragmatic peritonectomy, pelvic node dissection, and bladder peritonectomy. Fair agreement (0.21–0.40) for supracolic omentectomy, lesser omentectomy, pouch of Morrison peritonectomy, and para-aortic lymph node dissection.
Tier-I cities, with populations exceeding 100,000, are known for their robust real estate markets, advanced civic and social infrastructure, and status as established business centers. Tier-II cities, housing over 50,000 people, are characterized by emerging real estate markets and steadily improving infrastructure. Tier-III cities, with populations between 20,000 and 49,999, have nascent real estate markets and evolving business landscapes. In patients treated in Tier-I cities, a recurrent or residual disease most affected the lesser omentum and retrohepatic peritoneum. Conversely, in Tier-II and Tier-III cities, the bladder peritoneum and infracolic omentum were more frequently involved as subsites of recurrent or residual disease, respectively (refer to Fig. 1 and Table 2).
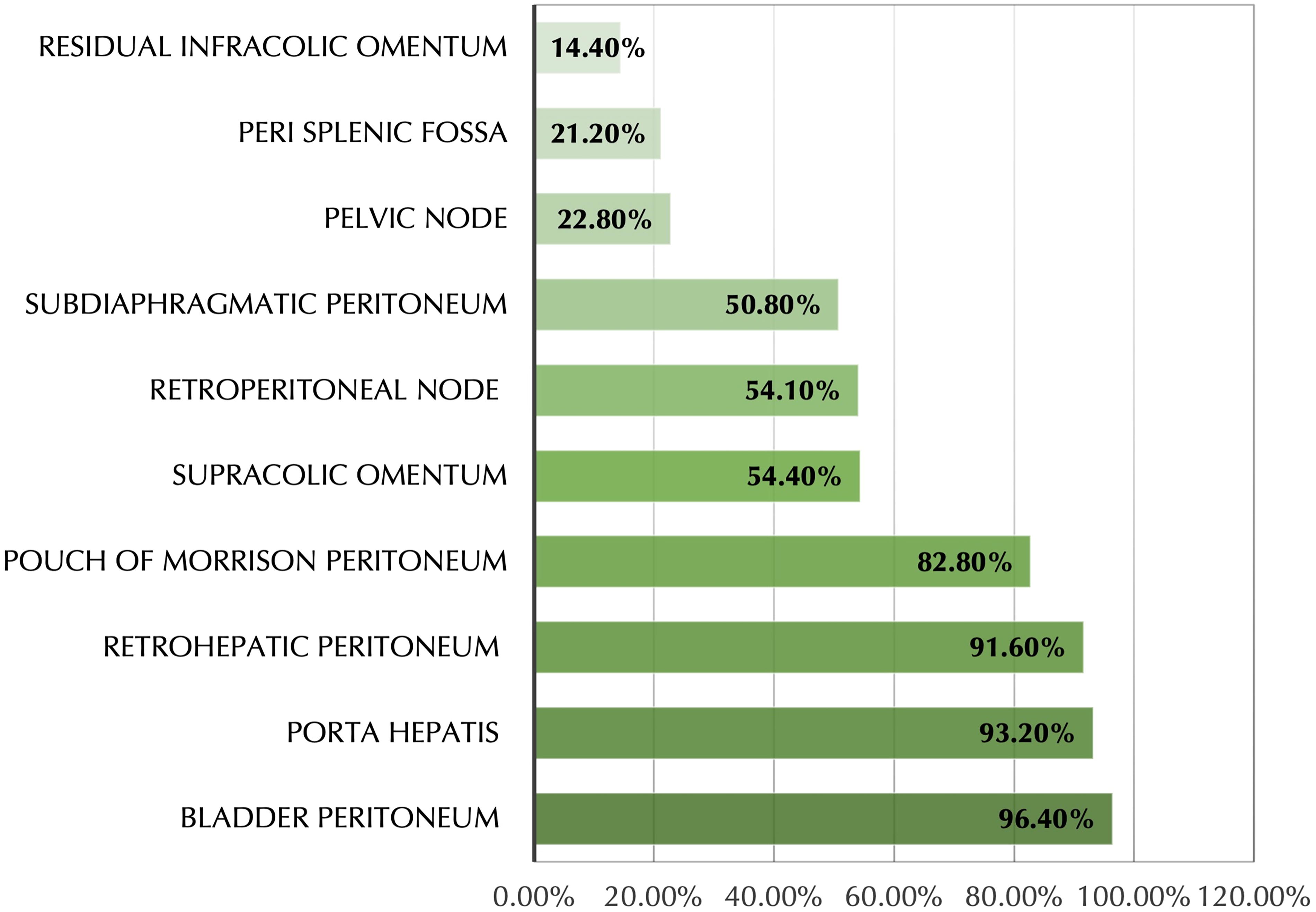
Sites of residual disease.
Sites of Residual Disease as per the Type of Initial Treating Facility
To achieve no gross residual disease (CC 0 resection), 56% of patients required additional standard cytoreductive procedures, 17% necessitated further radical resections, and 27% had extensive upper abdominal disease, mandating ultraradical surgery (URS). Detailed information on individual resections performed is presented in Table 3.
Details of Surgery Performed at Our Center to Complete Optimal Cytoreduction
LN, Lymph node.
Discussion and Review of Literature
EOC typically presents in advanced stages (III–IV), characterized by widespread dissemination in the pelvic and abdominal regions. The key to influencing prognosis and survival lies in maximal cytoreductive surgery followed by systemic or intraperitoneal chemotherapy.3,4 Over the past decades, numerous studies have highlighted the benefits of cytoreductive surgery in advanced disease. However, the critical factor determining prognosis is the extent of residual disease post-cytoreduction. Shifting toward more comprehensive primary cytoreduction has shown the potential to enhance survival rates in advanced ovarian carcinomas. Several studies have demonstrated that incorporating ultraradical procedures, particularly extensive upper abdominal procedures, can increase optimal cytoreduction rates and significantly improve progression-free survival and overall survival (OS).4–8
Defining the degrees of cytoreduction
The concept of cytoreductive surgery was initially proposed by Meigs in 1935, emphasizing the removal of maximum tumor burden to enhance the postoperative efficacy of chemotherapy. Subsequent studies, such as Munnell’s in 1968, established a positive correlation between maximal surgical efforts and OS. Griffiths, in a study of patients with stages II and III ovarian cancer, found that survival was consistently poor when the diameter of the largest residual tumor mass exceeded 1.5 cm, irrespective of the volume resected.9–11 GOG protocols 52 and 97, introduced by Hoskins in 1992, compared adjuvant chemotherapy outcomes based on residual disease size after primary cytoreduction, revealing better survival with smaller or no visible residual disease.12,13 Further analyses, including a meta-analysis by Bristow, indicated that increasing cytoreduction by 10% improved average survival by 5.5%. 14 Current trials emphasize that the absence of macroscopically visible disease has a more significant impact on survival than residual disease less than 1 cm. Optimal disease-free survival and OS are achieved with nil residual disease (R0 resection).15,16
Impact of radicality on survival
Increased radicality in surgical procedures directly correlates with enhanced survival. URS or maximal cytoreductive efforts involve additional procedures to eliminate all visible cancer. Cummins et al. demonstrated that cancer survival rates were highest in centers practicing more radical surgery, emphasizing the need for a change in policy for centers predominantly performing low-complexity surgery. 17
Upper abdominal involvement in advanced EOC
Approximately 60%–70% of patients with advanced EOC exhibit upper abdominal involvement. Standard procedures for tumor clearance in this region include diaphragmatic peritonectomy, diaphragm resection, liver resection, Glisson’s capsulectomy, cholecystectomy, periportal region clearance, Morrison’s pouch clearance, lesser omentectomy, clearance of the lesser sac, splenectomy, and suprarenal retroperitoneal lymphadenectomy. These procedures are crucial due to the frequent dissemination of malignant cells into these areas through ascitic fluid flow. 18
Benefits of ultraradical upper abdominal cytoreduction
Studies by Chi et al. and Ren et al. demonstrated that extensive upper abdominal surgery significantly increased the proportion of patients achieving complete gross resection without a significant rise in morbidity. Ultraradical surgery was associated with significantly higher median OS.8,19 Harter et al. showed that an improvement in optimal cytoreduction rates, achieved through more aggressive surgical procedures, corresponded to enhanced OS in patients with stages IIB–IV disease. 20
Role of secondary cytoreduction in recurrent ovarian cancer
AGO DESKTOP III and SOC1 trials have indicated a survival benefit in carefully selected patients with platinum-sensitive low-volume disease. A Peritoneal Carcinomatosis Index score <8 or involvement of 1–2 regions of the peritoneal cavity can guide the eligibility of patients for secondary cytoreduction. However, in patients with upper abdominal recurrence or disseminated disease, the benefits of secondary CRS remain undefined.
Optimizing outcomes in advanced EOC
Adjuvant chemotherapy following cytoreductive surgery is essential for optimizing outcomes in advanced EOC. Standard surgical procedures include total abdominal hysterectomy, bilateral salpingo-oophorectomy, total omentectomy, systematic lymphadenectomy, and selective removal of diseased peritoneum. Radical resections, such as anterior resection, low anterior resection, and ultraradical procedures like diaphragm peritoneal stripping and hepatic segmental resection, are frequently necessary. However, in many instances in our country, ovarian cancer surgeries are inadequately staged or involve “pseudo cytoreduction,” contributing to higher recurrence rates and poorer outcomes. The study reveals common recurrence and residual disease sites in the peritoneum and lymph nodes.
Conclusion
In our study, a significant portion of patients (56.6%) initially deemed to have optimal cytoreduction and presenting with recurrent disease were found to have residual rather than recurrent disease. This has led us to introduce the term “pseudo cytoreduction” to describe surgeries that, while considered optimal by many ovarian cancer surgeons, leave behind residual disease. The lack of standardized criteria for cytoreductive surgery in ovarian cancer may be contributing to this issue, possibly due to variations in skill levels or insufficient training among surgeons.
Our findings revealed that in 66.7% of cases, critical procedures such as lesser omentectomy, retrohepatic, and Morrison pouch peritonectomy were not performed, and incomplete resection of the Pouch of Douglas resulted in disease regrowth in the vault area. This phenomenon, rather than true recurrence, is what we term “pseudo recurrence.”
Notably, 49% of the initial surgeries were performed by general gynecologists, whereas only 18% were performed by gynecologic oncologists. Many patients lacked access to oncologists for their initial surgeries, which may limit the generalizability of our findings to populations with better access to specialized care.
Aggressive cytoreductive surgery, incorporating radical and ultraradical procedures as needed, is imperative for achieving complete disease clearance in advanced EOC. Specialized centers must shift practices towards performing more complex surgeries, making complete cytoreductive surgery an essential skill for surgical and gynecological oncologists treating advanced EOC. Emphasizing training for all surgeons involved in this field is crucial for improving patient outcomes.
Footnotes
Authors’ Contributions
M.D.R. the lead surgeon, contributes to the conceptualization, data curation, and formal analysis. C.R. is engaged in formal analysis and the creation of the original draft. S.R. participates in data curation, formal analysis, and the composition of the review, as well as editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.