
Abstract
Objective:
To compare intraoperative outcomes and complication between single-glove port laparoscopic hysterectomy (SGPLH) and vaginal natural orifice transluminal endoscopic surgery (VNOTES) hysterectomy.
Design:
The efficacy therapeutic research with retrospective data collection and propensity score math analysis.
Material and Methods:
Data were extracted from medical records of anonymous patients who diagnosed with benign gynecological disease and non-prolapse uterus who underwent SGPLH and VNOTES at Prapokklao Hospital, Thailand from January 2018 to August 2023. Study outcomes included operative time, estimated blood loss, perioperative complications, and postoperative pain. Factors applied for propensity score matching included age, body weight, body mass index, parity, underlying disease, previous abdominal surgery, and uterine weight.
Results:
A total of 101 patients were divided into two groups; 60 (59.4%) in the SGPLH group and 41 (40.6%) in the VNOTES group. The operative time of SGPLH was shorter than VNOTES (mean [SD], 93.7 [30.46] vs. 95.1 [41.5] minutes; p = 0.84). There was no significant difference between two groups in terms of previous abdominal surgery (p = 0.42) and others. In propensity score math analysis, among 32 pairs, there were no differences in operative time (mean [SD], 94.8 [28.18] vs. 97.2 [45.5] minutes; p = 0.79) and estimated blood loss (mean [SD], 167.5 [150.1] vs. 217.8 [212.7] minutes; p = 0.28) between the two groups.
Conclusions:
SGPLH and VNOTES showed no differences in operative time and in terms of complications. However, VNOTES required no abdominal incision.
Introduction
Currently, hysterectomy is one of the most common surgical procedures in gynecology. There are various methods and approaches to perform a hysterectomy, including open laparotomy, laparoscopic hysterectomy, vaginal hysterectomy, and robotic-assisted laparoscopic hysterectomy. The current recommendation for the treatment of hysterectomy is to consider vaginal hysterectomy as the first method if there are indications and if it is feasible, as it has fewer complications compared to other methods. 1 In addition to vaginal hysterectomy, there is also the option of performing a hysterectomy through laparoscopic surgery, which is preferred over open laparotomy. The choice of hysterectomy depends on the indication and many factors, such as the size of the uterus, the size of the birth canal, and the equipment and tools available in each hospital. All of this information should be provided to the patient to make an informed decision about the surgical method. Previously, vaginal hysterectomy was often chosen for patients with a descended uterus. In 2012, the first report of vaginal natural orifices transluminal endoscopic hysterectomy (VNOTES) in a non-descended uterus was published in Taiwan. 11 VNOTES is a combination of single-port laparoscopic surgery and vaginal hysterectomy, allowing vaginal hysterectomy to be performed in patients with a non-descended uterus or with associated uterine diseases.7–12
Currently, VNOTES is becoming more popular in Thailand, but it is not as widely available as laparoscopic hysterectomy or single-incision laparoscopic hysterectomy. This is because it requires the expertise and experience of gynecoendoscopists. However, there is an increasing amount of research on VNOTES, which has shown that it can reduce hospital stay and postoperative pain. 5 ,6,9,13 The duration of the surgery varies, with some studies showing shorter surgery times compared to single-port laparoscopic hysterectomy and comparable operation times to laparoscopic hysterectomy. 10 This study aims to compare the duration of surgery and the outcomes of VNOTES and single-glove port laparoscopic hysterectomy (SGPLH), including postoperative complications.
Material and Methods
This study is a retrospective cohort therapeutic study conducted at Prapokklao Hospital in Chanthaburi, Thailand. The protocol of the study was approved by the Ethics Committee for Research on Humans in Chanthaburi Province (CTIREC No. 058/66).
Data was collected from medical records covering the period from January 2018 to August 2023. The inclusion criteria for the study were as follows: 1) patients aged 20–80 years, 2) diagnosed with benign gynecological diseases such as leiomyoma, adenomyosis, endometrial polyp, etc., 3) having indications for surgical treatment, and 4) undergoing laparoscopic hysterectomy via SGPLH and VNOTES performed by a single surgeon certified in gynecological endoscopic surgery at the Obstetrics and Gynecology Department of Prapokklao Hospital, Chanthaburi Province.
The exclusion criteria for the study were as follows: 1) no surgical management, 2) conversion from VNOTES or SGPLH to conventional laparoscopic or open laparotomy, 3) incomplete medical records, 4) suspected uterine neoplasms before the operation, 5) laparoscopic hysterectomies performed for other conditions such as mental retardation, and 6) descended uterus.
The patients were divided into two groups: the first group comprised patients who underwent SGPLH, and the second group comprised patients who underwent VNOTES. This study compared factors between the two groups, including age, weight, height, body mass index, parity, prior abdominal surgery, uterine size from physical examination, hemoglobin level before surgery, and underlying diseases.
The primary outcome of this study is to compare operative time between the two groups, and the secondary outcomes include estimated blood loss during surgery, blood transfusion, uterine weight, length of hospital stay, postoperative pain, postoperative fever, and adjacent organ injury.
SGPLH was performed using a single trans-umbilical incision with a self-made glove port (created by suturing a No.7.5 sterile glove with an Alexis retractor) and three trocars (one-incision three-port laparoscopic), as shown in Figure 1. The trocars were secured with sterile rubber bands instead of using a commercial multi-access port, which is more expensive than the self-made glove port. VNOTES was performed with the same self-made glove port instead of a commercial gel port, as shown in Figure 2. Both groups used the same laparoscopic instruments, including a 30-degree 10-mm laparoscope (KARL STORZ, Tuttlingen, Germany), LigaSure (Covidien, Maryland 5 mm-37 cm, Boulder, CO, USA), grasping forceps, uterine manipulator, and monopolar hook. In all cases, the uterus was removed through the vagina, and the vaginal cuff was sutured transvaginally with continuous sutures using Vicryl 1-0. Both groups were operated on by the same surgeon, ensuring that the technique and sequence of steps in the operation were consistent. Manual morcellation was performed when the uterus could not be removed via the vagina, and no power morcellation was done in any of these cases.
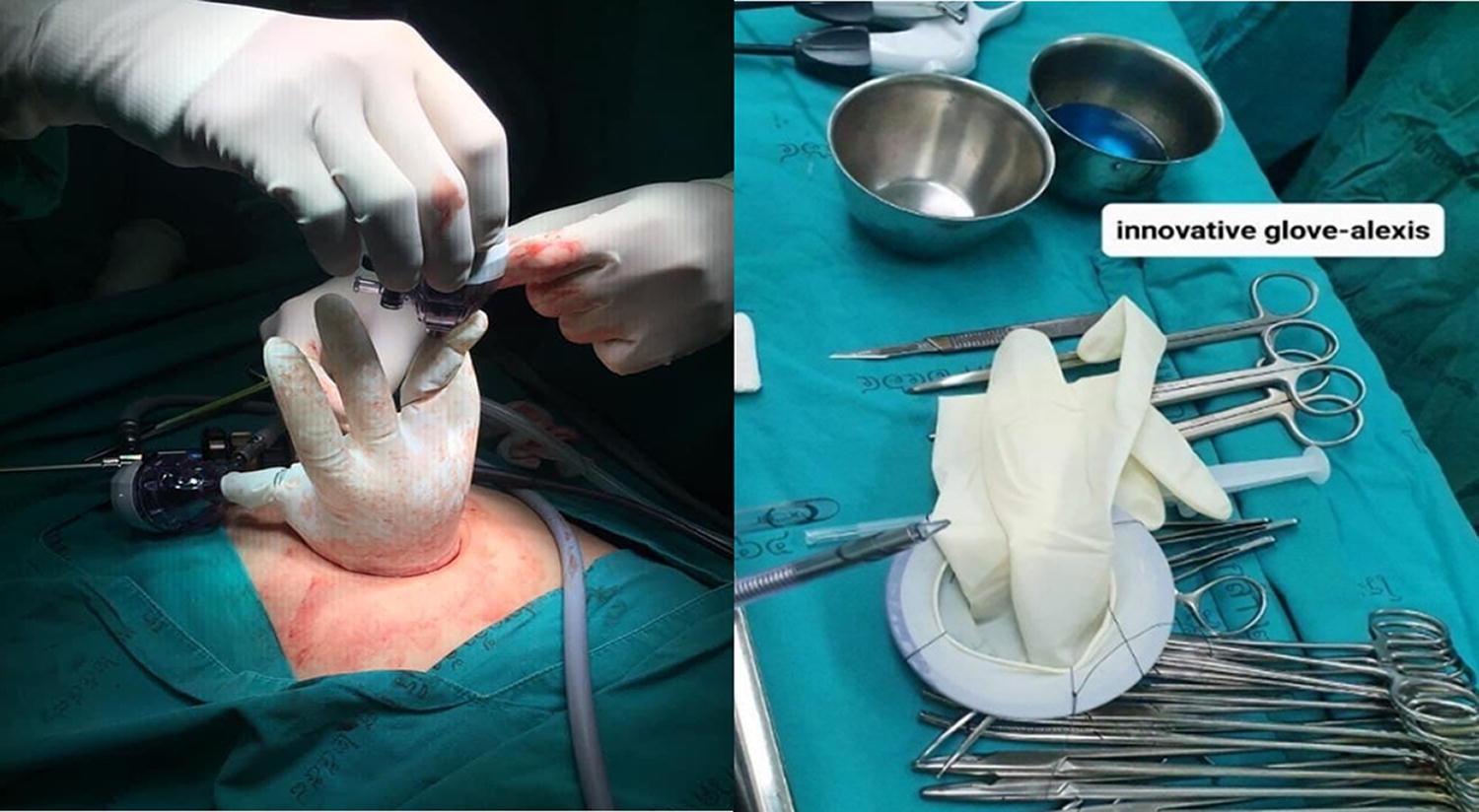
Single-glove port laparoscopic hysterectomy with self-made glove port.
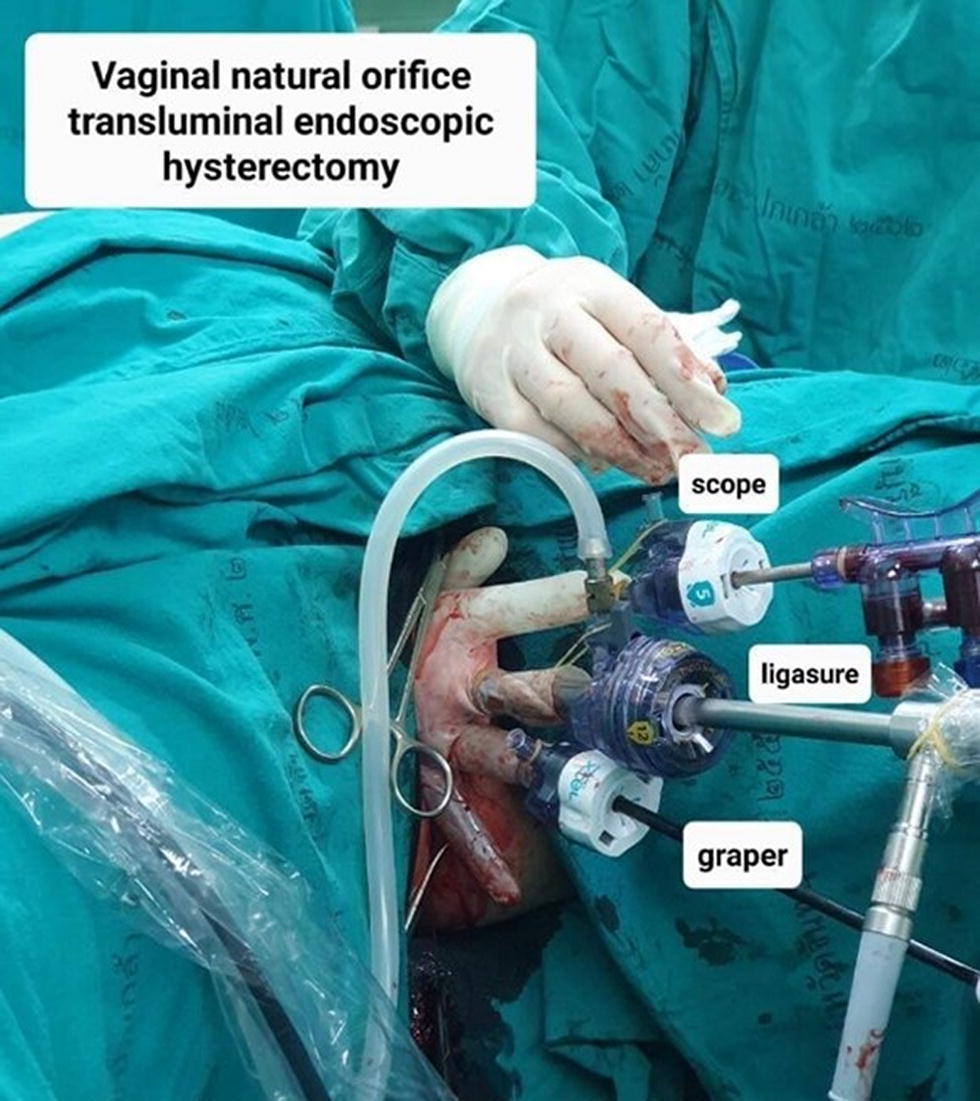
VNOTES with self-made glove port.
Operative time was recorded from the moment of the umbilical skin incision until the completion of the last skin closure. The amount of blood loss was calculated from the total volume of liquid in the vacuum aspirator’s cylinder minus the peritoneal lavage. Uterine weight was obtained by weighing after pathological examination. Patients were evaluated for postoperative fever, defined as a body temperature greater than or equal to 37.8°C for at least six consecutive hours, excluding the first 24 hours after surgery. Postoperative pain was assessed using the numeric pain rating scale at the time the patient arrived at the ward after surgery and 24 hours after surgery.
This research utilized statistical analysis through the computerized statistical software Stata version 14.2. For categorical data, the Chi-square test or Fisher’s exact test was employed for comparison, and results were reported as counts (%). For continuous data, independent t-tests were used for comparison, and results were reported as mean ± standard deviation. Following this, a logistic regression analysis was conducted using the variables of age, weight, body mass index, prior abdominal surgery, uterine size from physical examination, uterine weight (from the pathology report), underlying disease, menopause status, and parity to obtain propensity scores for each dataset. Subsequently, the entire dataset was divided into five groups with equal propensity score ranges. Afterward, each group was compared between SGPLH and VNOTES. A random selection was made for each of the five groups, resulting in 32 individuals for SGPLH and 32 individuals for VNOTES. The data from all 64 individuals were then analyzed and compared using the aforementioned statistical methods.
Results
A total of 421 female patients who underwent laparoscopic hysterectomy from January 2018 to August 2023 were initially considered for participation in the research. A total of 104 individuals were included in the study. However, 3 patients were excluded from the study: one due to a change in surgery to open laparotomy because of previous surgery and severe adhesion to other organs such as the small and large bowel, and two due to conversion to conventional laparoscopic hysterectomy because of severe adhesions. After these exclusions, a total of 101 participants remained for the research. Among them, 60 underwent SGPLH, and 41 underwent VNOTES, as shown in the study flow in Figure 3.
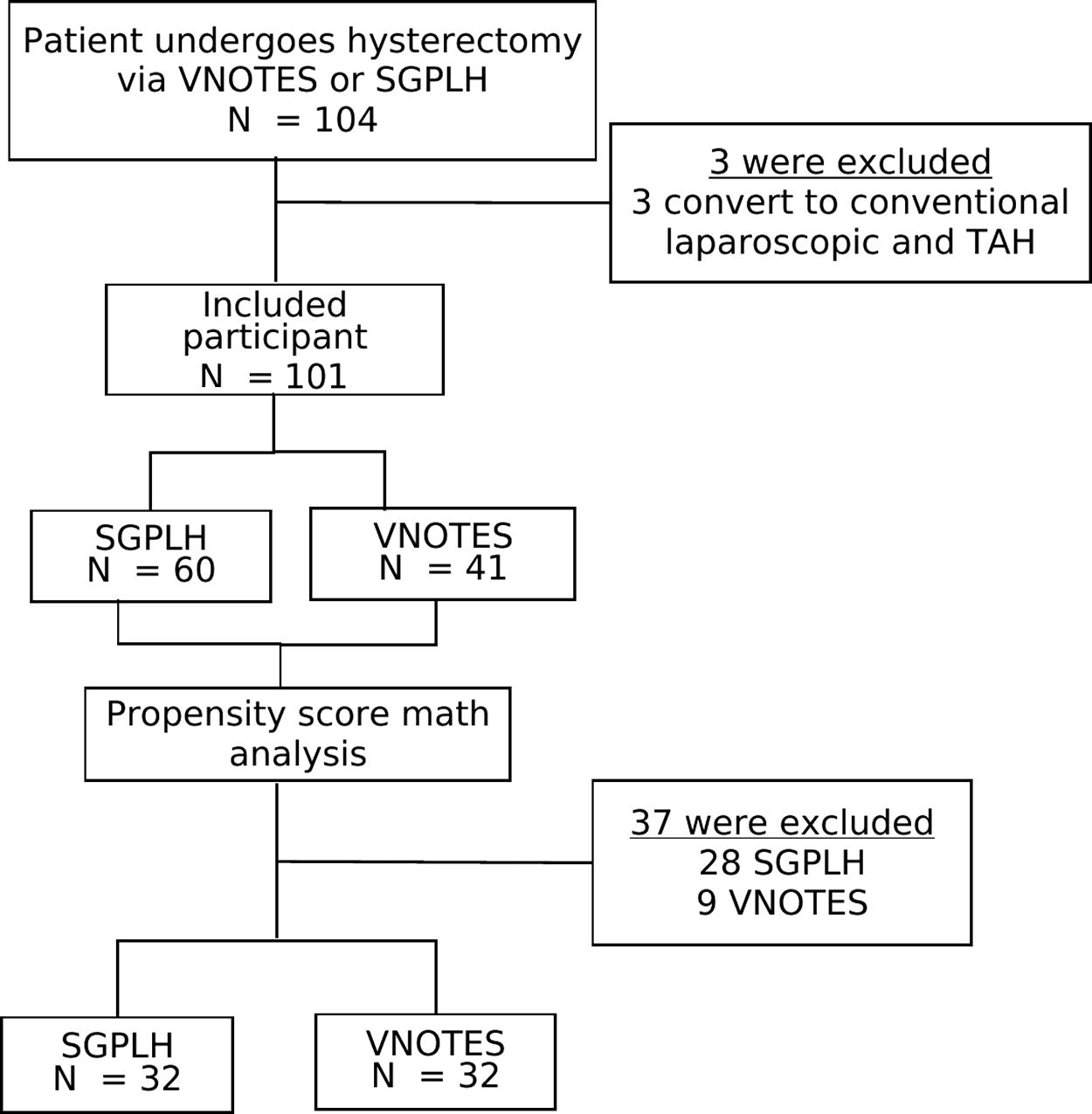
Study flow.
Demographic data of the research participants, including age, weight, height, body mass index, underlying medical conditions, parity, menopause status, prior abdominal surgeries, uterine size from physical examination, and hemoglobin level before surgery, were collected. Statistical analysis of this baseline data revealed a significant difference in underlying medical conditions between the group that underwent VNOTES and the group that underwent SGPLH. Specifically, it was observed that in the VNOTES group, the percentage of patients with underlying medical conditions was higher compared to the SGPLH group (53.7% vs. 28.3%).
This may be because of chance. This difference was statistically significant with a p-value of 0.013, as shown in Table 1. Other demographic data were not statistically significant.
Baseline Clinical Characteristics
After analysis with propensity scores and grouping the participants, a random sample of 32 individuals was selected from each group. Statistical analysis of the baseline data revealed no significant differences between the two groups. The average age of patients undergoing laparoscopic hysterectomy was 47.1 years for the SGPLH group and 46.1 years for the VNOTES group, with no statistically significant difference. Although, concerning medical history, previously there was a difference between the two groups, after analysis with propensity scores, it was found that the number of patients with a medical history did not differ significantly between the two groups. Specifically, 11 individuals in SGPLH group and 13 individuals in VNOTES group had underlying medical conditions (34.38% and 40.63%, respectively, p-value = 0.79), as shown in Table 2.
Baseline Characteristics of Study Participants after Propensity Score Matching Analysis
After analyzing the data, it was found that the average duration of surgery between SGPLH and VNOTES was 94.8 ± 28.2 minutes and 97.3 ± 45.5 minutes, respectively. The SGPLH approach appeared to be faster, although this difference was not statistically significant (p-value = 0.79). For other outcomes such as blood loss during surgery, uterine weight, length of hospital stay, postoperative pain levels, and the need for intensive care unit admission, there were no statistically significant differences between the two groups, as shown in Table 3. In addition, the postoperative complications, including postoperative fever and injuries to adjacent organs, did not show statistically significant differences between the two groups, as indicated in Table 4.
Surgical Outcomes
Complication
Discussion
From the study results, it was found that the duration of surgery for the SGPLH group and the VNOTES group did not show statistically significant differences. Although SGPLH had a shorter duration, compared to previous studies on VNOTES from Housmans, 2 Lerner, 5 Noh, 8 and Soo Jin Park, 9 the expertise in VNOTES at Phrapokklao Hospital, which started about 2 years ago (from 2022 to 2023), might not be equivalent to single-port laparoscopic surgery. This could lead to longer surgery times for VNOTES.
Other collected data, such as blood loss during surgery and admission to the critical care unit, did not show significant differences between the two groups, consistent with prior research by Housmans, 2 Seong Hee Kim, 4 and Soo Jin Park. 9 However, the hospital stay duration after surgery in both groups was approximately 3 days, with no significant difference, which contrasts with the longer hospital stay required after SGPLH reported in prior research by Housmans, 2 Kaya, 3 and Puisungnoen. 10 In contrast, open laparotomy requires a longer hospital stay, which typically lasts 4–5 days.
Regarding postoperative pain, previous research by Kaya, 3 Lerner, 5 and Noh 8 found less pain in VNOTES compared to single-port or traditional multi-port laparoscopic hysterectomy. However, in this study, the postoperative pain scores of both groups did not differ significantly, consistent with a previous study by Soo Jin Park. 9 In the study by Soo Jin Park, it was shown that postoperative vaginal pain in the VNOTES group was higher than in the single-site laparoscopic hysterectomy group.
Side effects from surgery in both groups were found to be similar and minimal. However, it’s essential to note that the study only collected short-term postoperative data, with follow-up appointments limited to three weeks after surgery. Long-term effects such as pelvic organ prolapse, wound separation, vaginal cuff separation, or postoperative infections may not be captured due to the lack of extended follow-up.
This comparative study has limitations, as it was not conducted as a randomized controlled trial. Selection bias in choosing patients for each surgical approach might exist, as surgeons and patients discussed and decided on the most suitable surgical method based on individual circumstances. To minimize bias, propensity score matching was employed to create two comparable groups with similar baseline characteristics. In conclusion, this research aimed to compare the outcomes of two surgical approaches. While the retrospective nature of the study and the limited sample size may pose some limitations, the findings suggest that VNOTES may take a comparable amount of time to SGPLH, considering the expertise and experience in both approaches. Future studies with larger sample sizes and longer follow-up periods are warranted to provide more comprehensive insights into the outcomes of these surgical techniques.
Conclusion
The VNOTES did not yield significantly different results compared to SGPLH across various outcome measures, including the duration of surgery, blood loss during surgery, length of hospital stay, intensive care unit admission, postoperative pain levels, and postoperative complications. The two surgical approaches showed no significant differences in terms of both the primary and secondary outcomes. It is noteworthy that VNOTES, being characterized by the absence of abdominal incisions, demonstrated comparable outcomes to SGPLH. As a result, VNOTES, which avoids visible abdominal scars, emerges as a viable and effective option for minimally invasive surgery in current medical practice.
Footnotes
Authors’ Contributions
Watcharin Chirdchim: Conceptualization, Methodology, Software, Data creation, Visualization, Investigation, Validation, and Writing—Reviewing and Editing. Pornpitcha Khumsupt: Data creation and Writing—Original draft preparation.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was provided for this study.