
Abstract
Objective:
To determine if implementation of a standardized evidence-based preoperative testing protocol within a patient population undergoing benign gynecological surgery would reduce unindicated evaluation without an associated increase in surgical complications.
Methods:
This was a retrospective cohort study. Patients assigned female at birth who underwent scheduled benign gynecological and urogynecological surgeries from May to October 2020 (before implementation) and August to November 2021 (after implementation) were included. Demographic information, preoperative testing, perioperative outcomes, and postoperative complications were collected for all patients. Tests were compared with the standardized testing protocol to determine what was indicated or not for each individual patient. A linear regression was used to estimate differences in total number of tests performed between groups. Surgical outcomes were compared for patients who underwent surgery before and after protocol implementation.
Results:
The total cohort was 378 patients, with 197 before implementation and 181 after implementation. The American Society of Anesthesiologists class was similar between groups. Prior to implementation, providers were more likely to obtain a preoperative complete blood count (CBC) (OR = 2.87, 95% CI: 1.69–4.88), a metabolic panel (basic metabolic panel [BMP] or complete metabolic panel [CMP]) (OR = 3.55, 95% CI: 2.24–5.64), and type and screen (OR = 2.21, 95% CI: 1.38–3.55) and less likely to obtain an electrocardiogram (OR = 0.45, 95% CI: 0.20–0.99). The number of unindicated CBCs and BMP/CMPs obtained decreased significantly over the study period (p < 0.01) as did the number of unindicated type and screens (p = 0.01). Intraoperative and postoperative complications were rare and did not differ significantly between groups.
Conclusion:
Implementation of an evidence-based preoperative testing protocol resulted in a reduction in unindicated testing without an associated increase in complications.
Introduction
Existing evidence-based guidelines discourage universal laboratory testing before scheduled surgery and support preoperative testing based on history and physical examination.1,2 Preoperative testing is estimated to cost $3–18 billion dollars annually in the United States, and 50%–70% of preoperative tests performed are unindicated.3–5 Studies in urogynecological cohorts observed no significant change in perioperative plan based on routine testing, and literature examining routine blood type and screens (T&S) before minimally invasive hysterectomies found low overall rates of transfusion for patients without a known history of anemia.6–8
The American Society of Anesthesiologists (ASA) has defined recommendations to perform preoperative testing for higher-risk (>ASA class 2) patients or those aged 65 years or older undergoing intermediate-risk or major-risk gynecological surgeries.3,9 Intermediate-risk and major-risk gynecological surgeries, as defined by the Johns Hopkins surgical risk classification system, consider the invasiveness of the procedure, surgical risk to the patient independent of anesthesia, and expected blood loss. 3 Despite multiple recommendations from surgical societies and recent gynecological surgical literature that demonstrated no changes in surgical outcomes between those receiving routine testing or not, the incidence of unindicated preoperative testing remains high, even in large academic institutions.8,10–13
We aimed to assess our institutional practice patterns of preoperative testing for scheduled gynecological surgery through a pilot study before and after institutional implementation of an ASA class-based testing protocol. We hypothesized that unindicated preoperative testing would decrease after protocol implementation, without a significant increase in perioperative or postoperative complications.
Methods
This study was approved by the University of Texas Institutional Review Board on August 23, 2022 (STUDY00003038). This was a retrospective cohort study of patients assigned female at birth undergoing benign gynecological and urogynecological surgery by an academic OB/GYN department at two hospitals before (May–October 2020) and after (August–November 2021) implementation of a standardized testing protocol.
Surgical cases were identified for inclusion from departmental case logs. Baseline data (before implementation cohort) for a period of approximately 5 months were first collected to assess a need for a quality improvement tool addressing perioperative surgical testing prior to proceeding with implementation. The postimplementation cohort was initiated 3 months after protocol publication over a similar timeframe to obtain a comparable number of patients for the baseline data. Surgical cases that were nonemergent and performed for benign gynecological and urogynecological indications were included. Emergent or urgent cases were excluded. Cases performed by a gynecological oncologist were excluded to remove those with a suspected or known malignancy. Included cases were assigned to one of two cohorts: patients undergoing surgery before (May–October 2020) or after (August–November 2021) the implementation of the studied testing protocol. Chart abstraction of inpatient and outpatient medical records was performed manually by the study authors, and data were entered in a REDCap database. Demographic information, preoperative testing obtained by surgical clinic providers (gynecological and urogynecological surgeons and nurse practitioners), perioperative outcomes, and postoperative complications were collected. Cases were excluded if any data points were unavailable.
The primary outcome was the mean number of unique tests obtained per patient before and after protocol implementation. Secondary outcomes included percentages of unindicated testing obtained and indicated testing not obtained, as well as intraoperative and postoperative complications.
Patient age, self-reported race and ethnicity, insurance type, ASA class, BMI, medical conditions, and preoperative diagnosis were collected. ASA class was determined by the assigned class documented in the anesthesia surgical record. Preoperative testing data collected included complete blood count (CBC) within 3 months of surgery, basic or complete metabolic panel (BMP/CMP) within 3 months of surgery, T&S performed within 3 days of surgery (per hospital protocol), and electrocardiogram (EKG) within 12 months of surgery. Each test obtained was designated as either indicated or unindicated based on our protocol. Tests that were indicated but not obtained were also determined. Perioperative surgical outcomes collected included procedures performed, intraoperative blood transfusion, and conversion of surgical route from minimally invasive to open. Postoperative complications within 6 weeks of surgery collected included postoperative blood transfusion, hospital readmission, and reoperation.
Based on literature review of recommendations on preoperative testing in gynecological surgery, specifically, a 2019 meta-analysis of preoperative testing for gynecological surgery by Shields et al., a testing protocol for use in our department’s benign gynecology and urogynecology divisions was created by a quality improvement team of resident and attending physicians at our institution. 3 Preoperative testing protocols were presented and vetted at a regional quality improvement conference on May 13, 2021. We presented an institutional preoperative testing protocol for benign gynecological and urogynecological surgery based on ASA recommendations and modified to address common gynecological and urogynecological conditions and procedures (Fig. 1). The protocol included ASA class definitions and class-based testing recommendations. 14 Regardless of ASA class, CBC was determined to be appropriate for patients with a history of anemia or uncontrolled abnormal uterine bleeding. The history of anemia was determined by chart review, of a documented hemoglobin less than 12 g/dL or a diagnosis documented within the patient’s medical record. A metabolic panel (BMP or CMP) was determined to be indicated for patients with an ASA class of 3 or greater. EKG within 12 months was determined to be indicated for patients aged 65 years or older. T&S was recommended for major surgeries, including abdominal hysterectomy, abdominal myomectomy, diagnosed/suspected stage 4 endometriosis, or if the estimated blood loss was projected to be >500 mL. After departmental review for feasibility, the protocol was immediately implemented in all our department’s associated benign gynecological and urogynecological surgery clinics, where patients’ preoperative assessment and ordering of labs is performed. Paper copies of the protocol were posted in all preoperative gynecological clinics and email reminders with the protocol attached were sent out to the gynecology and urogynecology departments monthly.

Standardized testing protocol created and adopted by the gynecological surgery department.
Demographic characteristics were compared using Student’s t-test or χ2 test as appropriate. p-Values <0.05 were considered significant. The primary outcome was the mean number of unique tests (CBC, BMP/CMP, EKG, and T&S) obtained per patient before and after protocol implementation. Secondary outcomes included intraoperative and postoperative complications, as well as the proportion of patients for which each test was obtained and whether the obtained test was indicated. A linear regression was performed to determine the change in rate of test ordering after protocol implementation controlling for age, race/ethnicity, insurance type, ASA class, and BMI. Analyses were conducted using SAS 9.4.
Results
A total of 378 cases met criteria for inclusion: 197 performed before protocol implementation and 181 performed after protocol implementation (Table 1). Patients undergoing surgery before protocol implementation were significantly older than those who had surgery after protocol implementation (before 52.1 ± 15.5 years, after 44.5 ± 13.3 years, p = 0.001). Most patients were White, non-Hispanic/Latina, and Hispanic/Latina, reflecting the patient population of Travis County served by the two hospitals in this study, and there were no significant differences in racial and ethnic backgrounds between groups (Table 1). 11 Most patients were commercially insured in both groups. Before implementation, more patients were insured through Travis County Central Health’s Medical Assistance Program (40% vs. 26%, p = 0.004) or were self-pay (9.6% vs. 2.2%, p = 0.003). After implementation, more patients had government-sponsored insurance (i.e., Medicaid or Medicare) (Table 1). There were no significant differences between patients classified as ASA class 1, 2, or 3 between groups. The most common underlying health condition in both groups was hypertension. Patients in the latter cohort were slightly more likely to have hypertension, cardiovascular disease, and kidney disease (Table 1). Surgery for abnormal uterine bleeding, pelvic pain/endometriosis, or adnexal mass was more common before implementation, and surgery for pelvic organ prolapse and urinary incontinence was more common after implementation.
Patient Baseline Characteristics
Data presented as n (%) unless otherwise noted.
Mean ± SD.
ASA, American Society of Anesthesiologists.
After adjusting for age, race/ethnicity, insurance type, ASA class, and BMI, patients who underwent surgery before protocol implementation had more preoperative tests (1.91 ± 0.96) than those who underwent surgery after protocol implementation (1.45 ± 1.07, p < 0.001) (Table 2).
Differences in the Number of Unique Tests Performed Between Patients Who Received Care Before and After the Implementation of New Guidelines
Data presented as mean ± SD.
The final model adjusted for age, BMI, ethnicity/race, insurance, ASA class.
Complete blood count (CBC), metabolic panel (BMP/CMP), electrocardiogram (EKG), blood type & screen (T&S).
The goal of protocol implementation was to decrease the percentage of unindicated testing obtained while maintaining or improving percentage of patients receiving tests that were indicated. Patients receiving unindicated testing decreased significantly for three of the four studied laboratory evaluations (Table 3). There was a slight increase in indicated CBCs that were not obtained postimplementation, but the overall percentage of indicated testing that was not obtained was low (Table 3).
Proportions of Studied Preoperative Tests Performed or Not Performed in Accordance with the Testing Protocol Before and After Implementation
Data presented as n (%).
CBC, complete blood count; BMP, basic metabolic panel, CMP, comprehensive metabolic panel; EKG, electrocardiogram; T&S, blood type and screen.
After adjusting for whether a test was indicated, providers were more likely to obtain a CBC (OR = 2.87, 95% CI: 1.69–4.88), BMP/CMP (OR = 3.55, 95% CI: 2.24–5.64), or T&S (OR = 2.21, 95% CI: 1.38–3.55) before testing protocol implementation. Providers were less likely to obtain an EKG before protocol implementation (OR = 0.45, 95% CI: 0.20–0.99).
Intraoperative and postoperative complications were rare for both study groups, and there was no significant difference in the total number of complications before or after implementation (n = 10 and n = 5, p = 0.25) (Fig. 2). Of the three patients who received intraoperative blood transfusions (all after implementation), all underwent preoperative T&S (all were unindicated) and two underwent CBCs (one was unindicated). All three patients who received postoperative transfusions (all before implementation) underwent preoperative CBCs (all indicated) and T&S (two indicated and one unindicated). There were no documented intraoperative or postoperative cardiopulmonary or end-organ complications in either cohort.
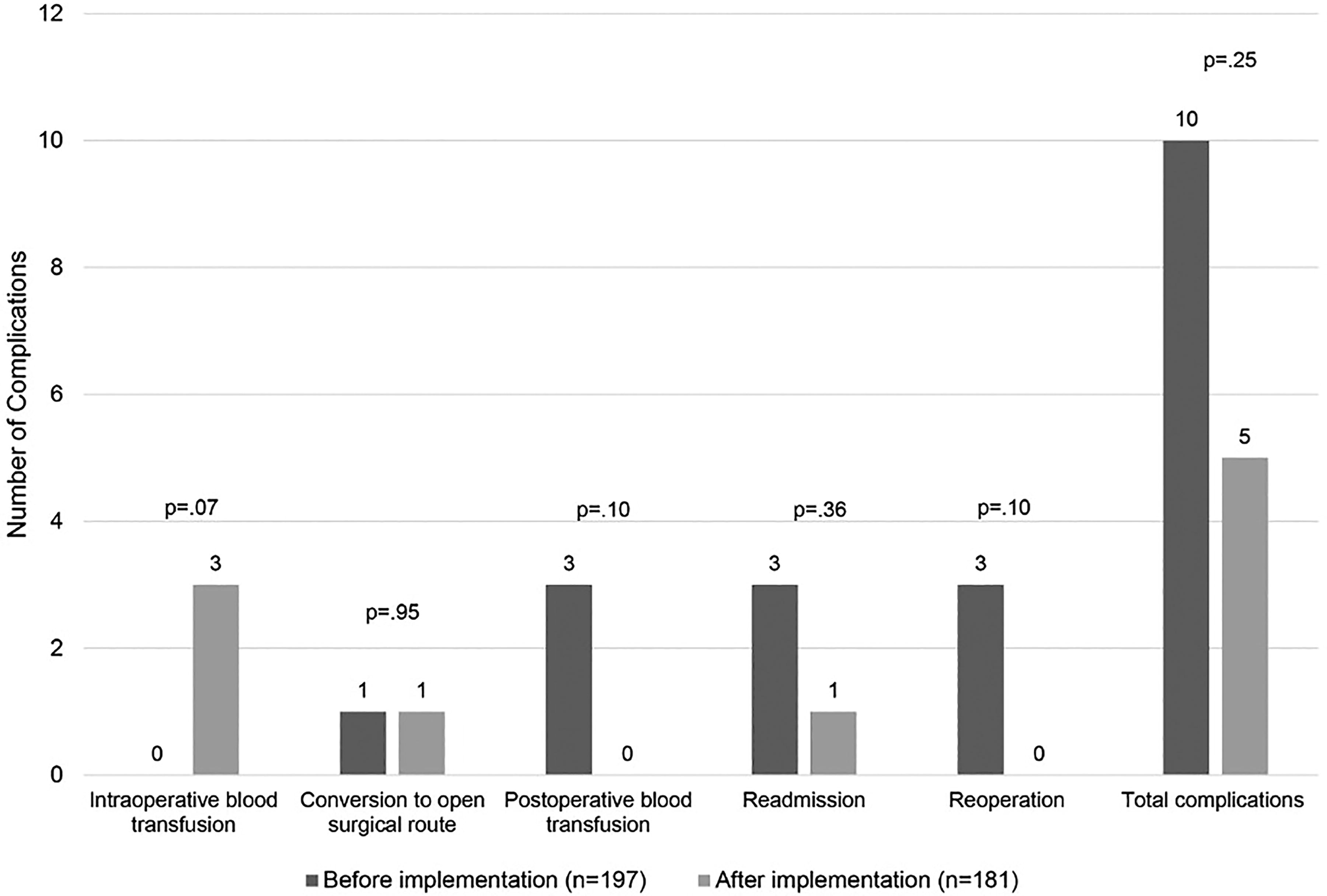
Complications within 6 weeks of surgery.
Discussion
In our pilot study, implementation of an evidence-based preoperative testing protocol significantly decreased unindicated preoperative testing for ASA classes 1 and 2 patients undergoing benign gynecological and urogynecological surgery without increasing adverse outcomes. Our findings align with evidence from multiple specialties including anesthesia, general surgery, gynecology, ophthalmology, orthopedic surgery, and plastic surgery and support moving away from routine preoperative testing and toward an individualized approach based on medical history, comorbidities, and surgical procedure.1,4,11–17 Although our study was not powered to detect differences in surgical complications and morbidity, a previous large database study by Mutter, et al. found that there were no differences between those who received preoperative testing versus those who did not in an ambulatory gynecological setting. 13
Our findings are an improvement from previous work that study the impact of a standardized guideline to decrease unindicated testing. Sigmund et al. found that the 2002 ASA guideline resulted in decreased unindicated testing nationally in only one of five tests examined. 18 In Benarroch-Gampel et al.’s National Surgical Quality Improvement Program database study of patients undergoing elective hernia repair after publication of the 2002 ASA guideline, 54% of patients still underwent laboratory testing without a clear indication and found no association between testing and occurrence of postoperative complications. 19 Bryson, et al. examined compliance to different preoperative testing guidelines published by two Canadian societies (Canadian Anesthesiologists’ Society and the Ontario Preoperative Task Force) at a single Toronto hospital, finding varying levels of noncompliance (5%–98%) for each test to either of the guidelines. 20 These authors concluded that the overuse of preoperative testing is influenced by practice traditions, medicolegal concerns, institutional policies, and lack of awareness of available evidence.12,17
During review of our preoperative clinic and hospital practices for creation of the quality improvement testing protocol, we observed some trends that may have contributed to our high rate of unindicated preoperative testing before protocol implementation. Preoperative testing previously was conducted based on ordering provider discretion rather than a specific institutional protocol. In addition, the majority of preoperative orders, both in resident and faculty clinics, were submitted via generic prechecked checklists that were not patient- or procedure-specific. After protocol implementation, providers were strongly encouraged to use forms with no prefilled laboratory orders for each patient to ensure individualization. Departmental educational presentations about our protocol and the data supporting its development ensured that implementation was not limited by lack of provider awareness.
Our results also showed that although there was a decrease in unindicated testing; there was also an increase in not performing indicated testing. Post-implementation, there was a statistically significant increase for CBCs that was not obtained despite being indicated (0.5%–4.4%, p < 0.001) (Table 3). This could be due to an exaggerated effort by providers to decrease testing after protocol implementation or a lack of fully understanding the protocol, further demonstrating the importance of continued coaching and repetition of guidelines when implementing a new practice, as well as using resources such as the Plan-Do-Study-Act method to continually study and improve upon the protocol long term. 21
Strengths of this study include its diverse patient population, large sample size, and variety of settings. Our patients were racially diverse, with a high proportion identifying as “Hispanic/Latina” and about half as “White, Non-Hispanic/Latina.” These racial/ethnic demographics reflect the study county demographics, as well as the growing Hispanic population nationally. 22 In addition, the study was performed in a variety of clinical settings including two academic hospitals and three different outpatient clinics, which supports the utility of our implementation process.
There are several limitations. First, the current published recommendations from which the protocol in this study was created are of overall low strength, demonstrating a need for more concrete evidence to improve the levels of recommendation on this topic. Implementation occurred in an academic training setting, which may have increased protocol adherence. This study was a pilot, with a post hoc power analysis on our limited cohort calculated to be 20.8%, confirming that it was underpowered to definitively detect any differences in complication rates. However, a prior large national database study has demonstrated no difference in complication rates in ambulatory gynecological surgery between those undergoing preoperative testing and those who did not. 13
There were differences in patient baseline demographics before and after protocol implementation, possibly due to selection bias related to study timeframe, which included short temporary hospital-initiated pauses in nonemergent surgeries related to the COVID-19 pandemic. The age difference between cohorts could be confounding, as providers may have been more likely to order more tests for older patients prior to protocol implementation. However, patients were slightly more likely to have certain medical comorbidities post-implementation, which is also a often noted factor that leads practitioners to obtain preoperative tests. Overall, there were no significant differences in ASA class between groups, which was the main deciding factor for preoperative testing in the protocol, and the number of truly “indicated” tests was similar between cohorts.
There were differences between cohorts on percentage of patients with certain types of insurance, specifically, a larger percentage of patients using the county’s Medical Access Program (which provides an insurance option for uninsured or low-income individuals) within in the first cohort, and more patients with Medicare or Medicaid in the post-implementation cohort. However, both insurance types are publicly funded and therefore may confer similar risk of restriction of coverage for medical care and evaluation. As such, the percentage of patients funded by public insurance was not significantly different between cohorts. In addition, we did control for patient age and insurance type in our logistic regression model on number of mean tests per patient, which are likely covariates with surgery indication and medical condition.
These differences in patient demographics and insurance status demonstrate a potential selection bias and highlight a need for continued study. A future study with an expanded patient population could help mitigate this bias and further confirm validity of these findings. In addition, future analysis over an extended time frame could examine if the changes in practice described in this study remain beyond the initial introduction of a standardized protocol, as well as any risk factors associated with returning to prior practice patterns.
Conclusion
Implementation of an evidence-based preoperative laboratory testing protocol for benign gynecological and urogynecological procedures resulted in a notable reduction in unindicated testing. At times, a clinician’s judgement may need to override algorithm-based testing, but in most cases, a framework like this protocol will promote value and reduce unnecessary patient cost.
Footnotes
Author’s Contributions
E.I. and N.B., under the supervision of M.T.B. and A.B.W., were responsible for the conceptualization and study methodology. E.I., N.B., and A.C. performed the investigation under the supervision of A.B.W., M.M.R., and M.A. curated the data and performed the formal analysis. E.I. wrote the original draft of this article, and N.B., A.C., A.B.W., M.M.R., L.K., and M.T.B. reviewed and edited it.
Prior Presentation
This research was presented via electronic poster at the 49th Annual Scientific Meeting of the Society of Gynecological Surgeons, held from March 19–22, 2023, in Tucson, Arizona.
IRB Approval
This study was approved by the University of Texas Institutional Review Board on August 23, 2022 (STUDY00003038).
Data Availability Statement
Data are available from the authors upon reasonable request.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was provided for this project.