
Abstract
Objective:
To assess the curative and reproductive outcomes of Hysteroscopic Endoscopic Operative System (HEOS) hysteroscopic cold resection system combined with plasma hysteroscopic electric resection system or patients with type III uterine fibroids seeking pregnancy.
Methods:
A retrospective case study was conducted on 13 patients who were diagnosed with type 3 uterine fibroids and underwent hysteroscopic cold resection and electric resection surgery at Zhongshan Boai Hospital in Guangdong Province, China.
Results:
All the 13 patients underwent single hysteroscopic myomectomy. The mean age was (31.4 ± 2.7) years, the mean diameter of myoma was (3.0 ± 0.7) cm, six patients had increased menstrual volume combined with anemia, and one patients had dysmenorrhea. After the operation, the menstrual flow of six patients decreased to the normal level, while seven patients showed no change, the dysmenorrhea of one patient has been improved. Two patients had mild synechia during hysteroscopy 3 months after operation. Within 2 years after operation, two were conceived naturally, eight patients conceived through IVF-ET, and one patient underwent artificial insemination (conception rate, 84.6%). Three patients had full-term natural birth, seven patients had full-term cesarean section birth, and one patient had abortion, with a live birth rate of 91%.
Conclusion:
The HEOS hysteroscopic cold resection system combined with plasma hysteroscopic electric resection system is feasible and effective in systematically treating patients with type III uterine fibroids who also have fertility demands, as it results in favorable reproductive outcomes for patients seeking fertility in the short term.
Introduction
Uterine fibroids are very common neoplasms in reproductive-aged women, with a cumulative incidence of 68.6%. 1 Studies indicate that uterine fibroids may impact the fertility and pregnancy outcomes negatively and are uniquely responsible for 2%–3% of infertility in infertile women requiring IVF-ET (in vitro fertilization and embryo transfer). 2 It is still noteworthy that the fibroids’ locations, sizes, and numbers affect female reproductive outcomes in different countries and studies. 3 The International Federation of Gynecology and Obstetrics defines type III uterine fibroids as those located in close proximity to the uterine mucosa without causing any morphological changes within the uterine cavity. 4 Some studies have shown that type III uterine fibroids often lead to adverse pregnancy outcomes such as infertility, repeated pregnancy failure, or embryo implantation failure, which may be related to fibroids being close to the mucosal layer and interfering with endometrial receptivity at the molecular level or damage to the muscle layer.5,6 Therefore, it is crucial to remove fibroids to maximize the protection of the endometrium and avoid scarred uterus for fertility protection. In the past, type III uterine fibroids were often removed using laparotomy or laparoscopy, requiring a contraception period of at least half a year, and cesarean section was often chosen as the delivery method.7,8 Additionally, there is also an elevated risk of developing pelvic adhesions and potential uterine rupture after surgery.9,10 Based on this, it is crucial to choose an appropriate surgical method to protect the patient with the desire for fertility.
With the development of hysteroscopic technology, Han et al. showed that hysteroscopic electrosurgical resection under the guidance of B-mode ultrasound is a safe and effective solution for the treatment of type III uterine fibroids. 6 Moreover, Capmas et al.’s study employed a bipolar electrosurgery method, which avoided open or laparoscopic myomectomy and effectively protected the fertility of patients with type III fibroids. 11 Although hysteroscopic electrotomy is a potential alternative to traditional surgery for the treatment of type III uterine fibroids and some progress has been made, it should be noted that it may result in thermal damage to the endometrium and an increased incidence of adhesions. 12 The World Health Organization attaches great importance to reproductive protection. Moreover, hysteroscopic cold resection system has gradually gained recognition and is now extensively utilized in treating various uterine cavity disorders. Through preliminary exploration, some scholars have found that hysteroscopic cold resection system is a convenient minimally invasive surgical method, which has less damage to the endometrium and is beneficial to patients with fertility demands. 13 However, there are few studies exploring the therapeutic effects of hysteroscopic cold resection system combined with electric resection system for type III uterine fibroids to date.
Therefore, we performed a single-center, retrospective, case study to evaluate the effects and pregnancy outcomes of hysteroscopic cold resection system combined with electric resection system resection for type III uterine fibroids.
Materials and Methods
Study participants
A retrospective study was conducted in our hospital from April 2020 to April 2022. This study was approved by the Zhongshan Boai Hospital Ethics Committee (ID: KY-2024-06-02), and consent of the patient was obtained. We searched the electronic case system of patients diagnosed with type 3 uterine fibroids and who underwent cold resection system combined with electric resection system myomectomy in Zhongshan Boai Hospital, Guangdong Province, China, to determine all study subjects who met the inclusion criteria for gynecological visits in our hospital within the past 2 years. Our study included (1) patients aged 27–35 years, (2) fibroids with diameter > 1.9 cm, (3) desiring future fertility; and (4) type III uterine fibroid (occasionally in addition to type 0–2 fibroids). Our study excluded (1) patients with contraindications to hysteroscopic surgery, (2) patients with congenital or acquired uterine malformations, (3) a single fibroid is > 4.5 cm in diameter, and (4) missing cases.
An experienced reproductive surgeon (performing > 1000 hysteroscopic procedures per year for > 20 years as a resident) performed all procedures. All operations were performed by one doctor, eliminating data interference caused by different doctor.
Preoperative preparation, surgical method, and follow-up
Patients were admitted to the hospital for surgery within 3–7 days after the end of the menstrual cycle (patients with prolonged menstruation: 8–10 days). After admission, all patients were required to complete relevant examinations, such as blood and urine routine and coagulation function, to exclude surgical contraindications. Patients with anemia were treated with blood transfusion until their hemoglobin was > 80 g/L. Cervical softening and dilation is performed one day before surgery, and antibiotics are administered 30 minutes before surgery to prevent infection. After the surgery begins, oxytocin is administered intravenously. During the surgical procedure, we utilized the HEOS system, a product of the French company Sopro-comeg, along with the plasma hysteroscopic electric resection system manufactured by Olympus Company.
During the operation, the shape of uterine cavity was observed comprehensively to determine the diameter, shape, and location of fibroids. At the same time, type 3 myoma was located under ultrasound. The cold knife shear was employed to incise the endometrium and the subendometrial fibroid capsule, with a length roughly equivalent to the fibroid diameter (Figs. 1 and 2). Double curved scissors were then utilized to delicately separate the fibroid from the surrounding tissue layers, layer by layer. A 3 mm × 3 mm-toothed forcep was delicately utilized to gently draw the fibroid toward the uterine cavity. The fibroid transformed from a type 3 fibroid into a type 1–2 submucosal fibroid (Fig. 3). According to the specific situation of fibroids, the five steps of “cutting, clamping, twisting, pulling, and delivery” were adopted.
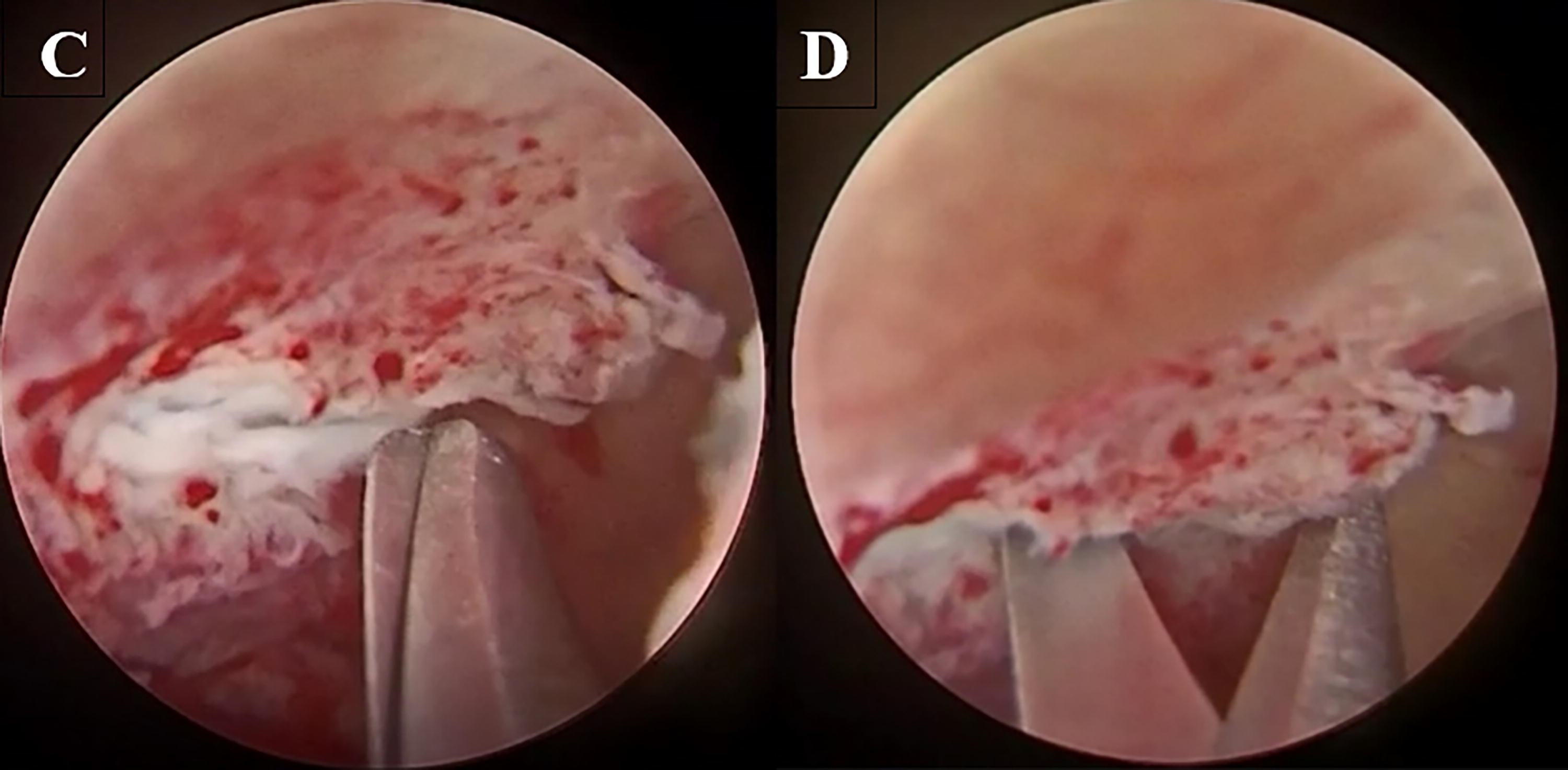
Cutting the envelope of myoma near the intima under B-ultrasound guidance
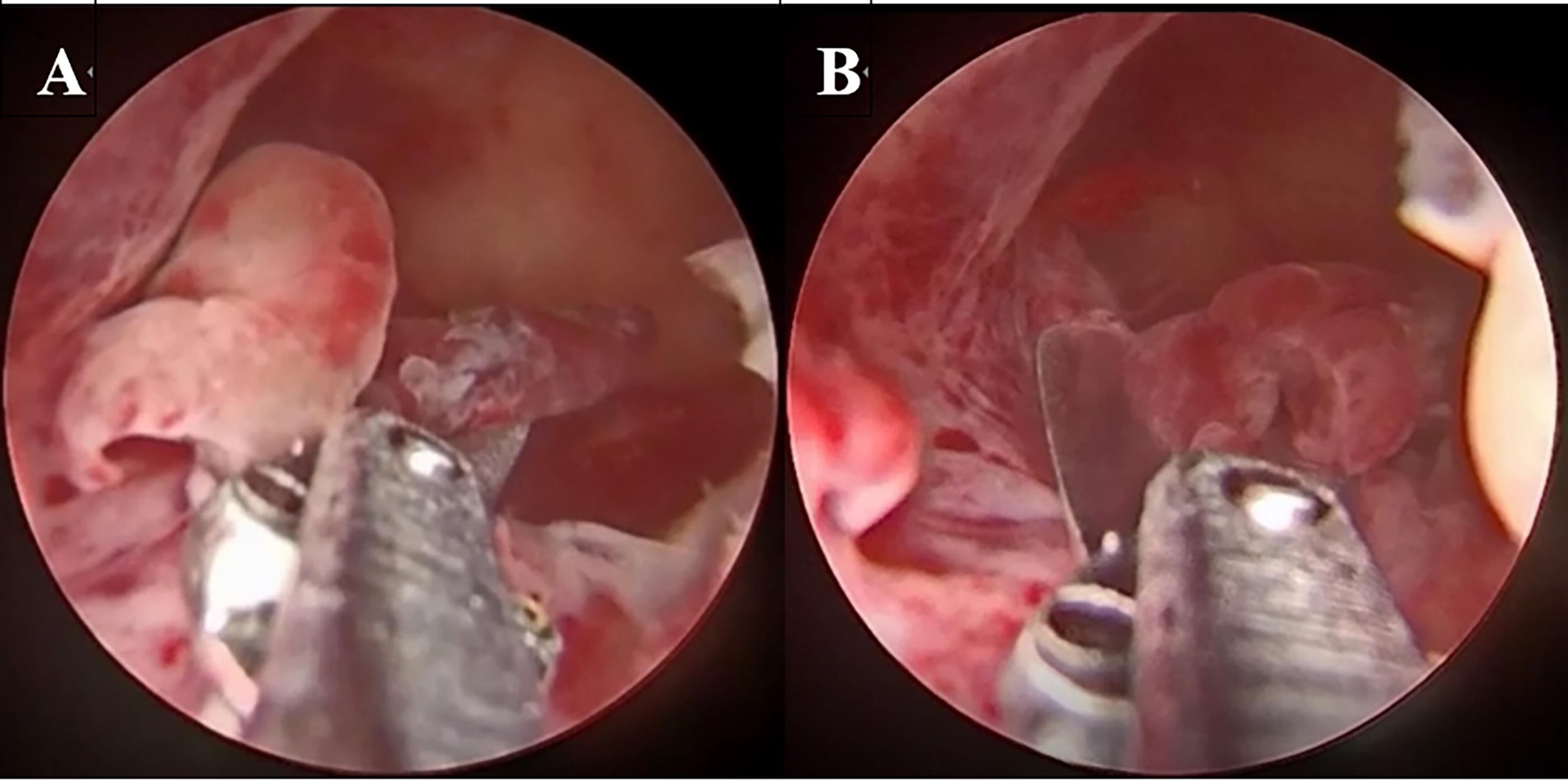
Cold knife resection of endometrial polyps
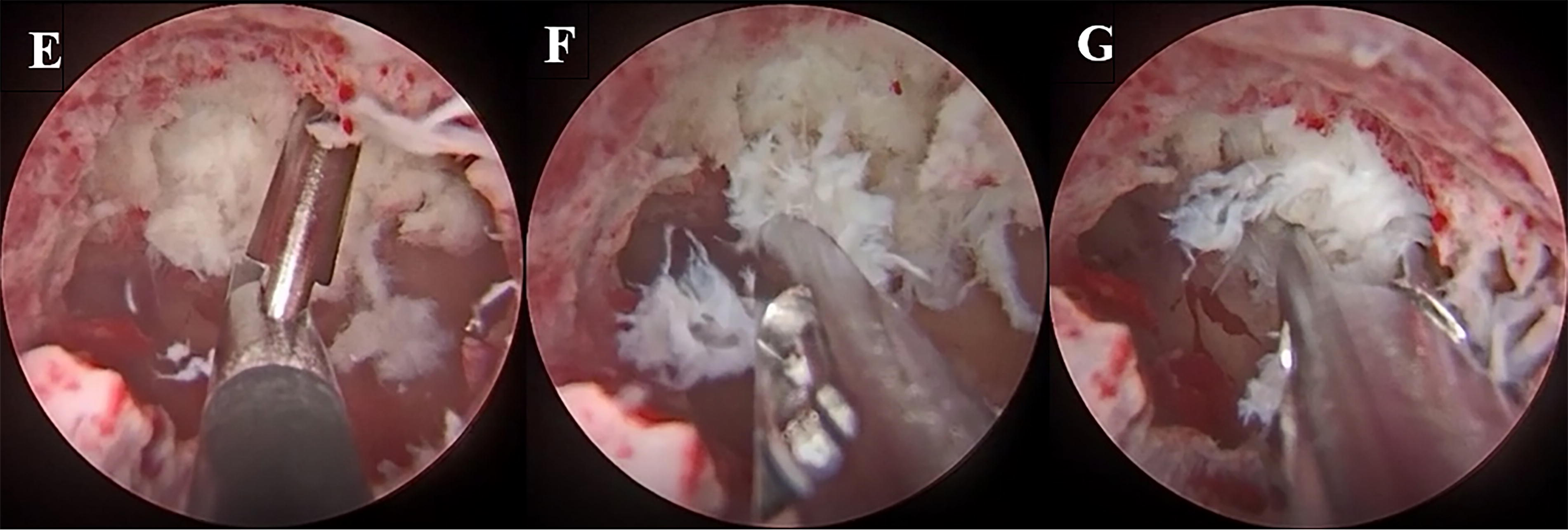
The myoma was separated into type 1–2 by cold knife clamp
After resection of the fibroids, the distance between the edge of the fibroid fossa and the serosa layer was measured by ultrasound, and all the fibroid tissues were sent for pathological examination. For patients with fertility requirements, a hysteroscopy review is recommended within 3 months postoperatively to assess any potential intrauterine adhesions, as well as to detect changes in endometrial thickness and menstrual flow volume. Patients were followed up by outpatient examination or telephone for 24 months to detect the recurrence of fibroids and postoperative pregnancy.
Statistical analysis
The SPSS 25.0 software package for Windows (SPSS Inc., Armonk, NY, USA) was used to calculate the statistical data. According to the data distribution, paired sample t-test or chi-squared test was used. All tests were two-tailed, and p < 0.05 was considered to indicate statistical significance for all analyses.
Results
The mean age of the patients was 31.4 ± 2.7 (range, 27–35) years. Before surgery, histopathological examination confirmed that all the 13 cases were common uterine leiomyoma, which showed crisscrossing of muscle layers and disordered tissue arrangement under the microscope. The average diameter of fibroids was 3.0 ± 0.7 (range, 1.9–4.2) cm, six patients presented with a combination of type 0–2 multiple uterine fibroids, six patients had hypermenorrhea and anemia, and one patient had dysmenorrhea before operation. The average distance between myoma and serous membrane of uterus was 3.5 ± 1.0 (range, 1.8–5.0) mm.
All 13 patients underwent single operation. The mucosal layer was incised by using the cold knife scissors. Subsequently, the fibroids were pulled out with a cold clamp and then resected electrically. Regarding the choice of surgical methods, for type 0 pedunculated submucosal fibroids, our hospital suggests to use the electric resection system. However, when combined with types 1 to 3 submucosal fibroids, a combination of cold resection system and electric resection system surgical methods should be selected. Intraoperatively, the mean duration of surgery was 38.5 ± 9.7 (range, 20–55) minutes, and the mean blood loss was 23.9 ± 10.2 (range, 15–50) ml. After surgery, no patients reported dysmenorrhea. Those patients who experienced menorrhagia pre-op had resolution of these symptoms post-op. The mean recovered muscle layer thickness from the tumor bed to the serosal layer was 9.9 ± 0.7 (range, 8.6–11.2) mm, which was within the normal range, and the difference was statistically significant compared with that before surgery (p = 0.000). During the hysteroscopy, review 3 months after surgery, two patients exhibited mild adhesions (stage I, according to The American Fertility Society classification 14 )—adhesions were was easily lysed by using Hegar’s dilators or moving the tip of the hysteroscope. All patients underwent surgery smoothly, experiencing no complications either during or after the procedure. Furthermore, there was no recurrence of fibroids reported within 2 years post-surgery (Table 1).
The Patients’ Clinical Characteristics
Note(s): +, present; -, not present; NR, normal range; Pre, preoperative; Post, postoperative; /, ratio; N, norm
Regarding pregnancy outcomes, all 13 patients expressed a desire to conceive. Seven patients had successful pregnancies within 3–5 months after surgery, two of them had two implant failures before surgery, three patients became pregnant within 6–12 months, one of them had two implant failures before surgery, and one patient was successfully pregnant between 12 and 24 months. However, two patients did not conceive within 2 years. One of the factors contributing to the failure of IVF-ET for a particular patient stemmed from her premature ovarian failure as well as her partner’s diagnosed asthenozoospermia. Another patient who tried to conceive spontaneously did not become pregnant due to blockage of fallopian tubes within the follow-up time (24 months). Second, among the 13 patients, two were conceived naturally, eight patients conceived through IVF-ET, and one patient underwent artificial insemination (conception rate, 84.6% [11/13]). Finally, three patients had full-term natural birth, seven patients had full-term cesarean section birth, and one patient had abortion, with a live birth rate of 91% (10/11) (Table 2).
Pregnancy outcomes.
IVF-ET, in vitro fertilization and embryo transfer.
Discussion
Currently, the surgical treatment of type 3 uterine fibroids remains understudied and relatively overlooked. There are only sporadic case reports of the HEOS hysteroscopic cold resection system combined with the plasma hysteroscopic electric resection system in the treatment of type 3 uterine fibroids. Consequently, the clinical effects and pregnancy outcomes of patients who wish to preserve fertility need to be further explored and studied. Compared with the traditional operation method, the hysteroscopic resection of type 3 uterine fibroids in this study has shorter operation time, less intraoperative and postoperative bleeding, faster postoperative recovery, and shorter hospital stay. Furthermore, the cold cutting system minimized the incidence of uterine adhesion. This method achieved remarkable therapeutic outcomes with high safety, effectively aiding menstrual recovery and enhancing post-surgical pregnancy prospects. It is a desirable choice for patients with short-term pregnancy and fertility preservation goals.
In this study, we employed a technique that first utilized a cold knife to delicately open a window, minimizing damage to the surrounding endometrium. Subsequently, an electric knife was introduced into the fibroid cavity to swiftly excise the tumor, significantly enhancing surgical efficiency, which was similar to the study by Zhao et al. 15 Zhao et al. 15 reported that the combined application of cold clamp and energy instrument of HEOS system completed the treatment of diffuse uterine leiomyomatosis, resulting in less intraoperative blood loss, shorter operation time, improved the recovery effect of myometrium thickness after operation, and postoperative pregnancy rate. Therefore, surgeons need to be trained and combined with their own experience to choose the appropriate device for different cases individually. If necessary, the combination of electric resection and cold resection instruments can provide the best treatment effect for patients, which may be an effective strategy.
Our study also found that patients did not experience moderate to severe adhesions after surgery. The incidence of mild adhesions 3 months after surgery was 15.4% (2/13). These findings indicate that the use of nonenergetic instruments such as cold forceps in hysteroscopic cold resection reduces endometrial damage, which is beneficial to reduce the incidence of uterine adhesion. Additionally, our patients did not experience complications such as uterine perforation, significant bleeding, or infection during or after surgery, which is contrary to previous reports. 1 This may also be attributed to the fact that the patients in this study had only one operation, or the surgeons who operated on them were highly experienced. Moreover, compared with the electroresection group in the study of Yong et al., 16 the time point of embryo transfer for our study subjects was moved forward by 3 months, which met the demands of the rapid embryo transfer couple. The pregnancy rate of seven patients was 53.8 (7/13) at 3–5 months, the pregnancy rate of three patients was 23.1 (3/13) at 6–12 months, the pregnancy rate of one patient was 7.7 (1/13) at 12–24 months after surgery, the pregnancy rate reached 84.6% (11/13), and the live birth rate was 91% (10/11). Within 2 years after surgery, all our patients had good reproductive results and finally realized their desire to conceive. However, due to the follow-up time of only 2 years, follow-up of pregnant patients was not continued. Therefore, the reason for no pregnancy within 24 months after the operation may be that the follow-up time was not long enough, patients changed their minds about reproductive goals, or pregnancy was impossible due to comorbid conditions or other uncontrollable factors.
Compared with traditional laparoscopic and open surgery, hysteroscopic cold resection system combined with plasma hysteroscopic electric resection system has obvious advantages in reducing pain and endometrial damage, and improving reproductive prognosis. However, for large fibroids with few interwall protrusions, hysteroscopic operation is difficult, and intraoperative complications such as perforation may occur. Preoperative evaluation using transvaginal ultrasound or pelvic magnetic resonance imaging to assess the location of fibroids and myometrial thickness can significantly aid in determining the precise depth and extent of fibroid resection during hysteroscopic surgery. This approach helps prevent complications such as uterine perforation, thereby ensuring the safety and completeness of the procedure. Furthermore, cold knife instruments are fine and sharp, easy to cause uterine perforation and instrument damage, the operation is relatively difficult, and needs to be completed by experienced doctors. Given the relatively high cost of the equipment and instruments required for hysteroscopic cold resection surgery systems, economic factors must also be taken into account during instrument selection.
The results of this single-center retrospective study may not be fully generalizable to all patients with type 3 uterine fibroids who require assisted reproductive technology. Although there are reproductive surgery and assisted reproductive technology centers in our hospital, the statistical power is insufficient and the small number may affect the degree of bias in the results. Therefore, a long-term observational study with a large sample size is recommended. It is possible to collaborate with multiple centers and combine basic research to expand research into the diagnosis and treatment of type 3 fibroids and ultimately better guide future clinical work.
In summary, our findings provide evidence that hysteroscopic cold resection system combined with electric resection system is an option for the treatment of some type 3 fibroids.
Conclusion
Although type 3 fibroids do not cause changes in the shape of the uterine cavity in women, they may affect fertility. In this study, the combination of hysteroscopic cold cutting system and electric cutting system makes the myometrium without wound, the patient recovers quickly after operation, and the time of embryo transfer is moved forward, which better protects the endometrium, reduces the uterine scar, and the patient’s fertility is greatly provided.
Footnotes
Acknowledgment
Thank you for all the contribution of the researchers in this study.
Ethics Approval and Consent to Participate
This study was approved by the Zhongshan Boai Hospital Ethics Committee (ID: KY-2024-06-02) and obtained informed consent of all study participants.
Consent for Publication
All participants and researchers consented to publication.
Availability of Data and Materials
The datasets generated and analyzed during the current study are not publicly available but are available from the corresponding author upon reasonable request.
Authors’ Contributions
All authors made significant contributions to this article. B.G. contributed to the conception of this work. L.X. and S.G. contributed to the acquisition of data. B.G., L.Y., L.X., and D.J. contributed to the analysis and interpretation of data. B.G. and L.Y. drafted this article, and all authors critically revised the article and approved the final version to be published. All authors are responsible for all aspects of the work and the article.
Author Disclosure Statement
The authors declare that they have no conflicts of interest and nothing to disclose.
Funding Information
This study did not receive funding support.