
Abstract
Study Objective:
Assess what demographic variables affect self-representation in online biographies.
Design:
National, cross-sectional review and analysis of surgeon biographies.
Setting:
Publicly available biographies obtained online.
Patients:
2011–2021 FMIGS US Graduates.
Interventions:
Data extracted for each surgeon included sex, graduation year, and state and region of current practice. Biography text was uploaded into the Linguistic Inquiry and Word Count (LiWC) Software and analyzed for measures of analytic thinking, clout, and authenticity using a summary statistic provided by LiWC. RStudio was used to analyze LiWC output.
Measurements and Main Results:
Of the 268 biographies collected, 75.4% were from female surgeons, and 24.6% were from male surgeons. Graduates practiced in 29 states and Washington, DC, primarily centered around urban areas including Los Angeles, San Francisco, Philadelphia, New York City, Pittsburgh, and DC. State and region of practice significantly impacted authenticity, while region had impacts on analytic thinking and clout. Biographies from Western states scored higher on authenticity than those from Northeastern and Southern states. Western states scored lower on clout than the South or Northeast, and the South scored higher than the Midwest. Surgeon sex or graduation year did not significantly impact the studied variables.
Conclusion:
The significant impact of region and state of current practice on a surgeon's biography suggests that surgeon representation differs between geographies and reinforces how local factors strongly influence the health care market. Further research into market characteristics and practice patterns can elucidate what drives the importance of biographical characteristics and whether that impacts patient care.
Introduction
In the past century, health care has evolved to incorporate patient preferences, 1 in addition to medical indication, as an additional central component to treatment plans. One of the pillars of patient preference involves the choice of a physician. Private insurers have provided some guidance for patients searching for a primary care physician and recommend scheduling an in-person, face-to-face meeting. 2 This time commitment, however, can be challenging given the average American's work, school, and family responsibilities. To better assist in a patient's choice in selecting a new provider, health care providers increasingly include personal information in their online biographies to help patients in their remote searches.
Physician biographies tend to include both philosophy of care and personal information: where they are from, their marital status, number of children, and other interests. 3 The information in the biography can be understood as a self-described representation of the care the patient will receive.
Location and, more importantly, access to health care services should be considered as playing a role in this choice. These variables can have a significant influence on health care decision-making. Rural women are less likely to see an OBGYN than their urban counterparts and more likely to visit with family medicine physicians or Advanced Practice Providers (APPs). 4 Part of this disparity is likely due to differences in access to OBGYNs versus family medicine physicians or APPs 4 in rural areas. Still, availability is not the only factor that can influence care consumption. Perceived quality of care, 5 affiliations with an academic hospital, or communication style (for which a proxy could be a physician's self-representative biography) can all influence a patient's choice of a provider. 6 Affiliations with academic centers inherently vary based on the location of currently existing academic centers—which tend to cluster in urban areas. Specialists, such as minimally invasive gynecological surgery (MIGS) surgeons, providing care at these centers are thus less available in rural America. Patient-perceived stigma about certain procedures (such as pregnancy termination) or specialty care can vary in rural areas, 7 affecting the way physicians write about their care philosophy or services provided. Satisfaction with care, due to perceived quality of care and communication style preferences, can also shift based on local cultural factors. This then results in a shift in patient priorities for what they want from their care and how they interact with their providers.
Location also impacts insurance status and other demographic variables. People living in rural areas are more likely to be older, uninsured, and have completed less education, while people in urban areas are more likely to be foreign-born or live in poverty. 7 These are significant differences that, with the aforementioned geographic factors, can influence a patient's choice in physician. There has been little research on how self-representation in physician biographies is impacted by sex, location, or other factors. It is important to note the difference between gender and sex. Sex is defined as a biological characteristic (female or male), and gender as a social one gender is a social one. 8
MIGS is a popular surgical technique associated with lower rates of postoperative complications, shorter hospital stays, and quicker return to normal activity compared to more invasive approaches. 9 Subspecialty accredited fellowship training in MIGS is a growing field in OBGYN, 9 importantly increasing MIGS access for patients in both rural and urban settings. Understanding how gynecological surgeons represent themselves to patients may influence patient decision-making in the field. This study aims to describe the online biographies of fellowship-trained MIGS surgeons and demonstrate linguistic differences based on surgeon sex, location, region, and fellowship graduation year.
Methods
This national, cross-sectional review of surgeon biographies was considered exempt by the Northwestern IRB. A list of publicly available 404 MIGS Fellowship (FMIGS) graduates over 10 years (2011–2021) was reviewed. Biographies were obtained from internet searches. Text from each biography was extracted and saved into a document along with the following variables from the surgeon's website: sex of the surgeon, medical school, year of graduation from FMIGs fellowship, and state and region of current institution. Though gender and sex are not interchangeable, the literature has yet to adequately include this consideration in their reporting of research data. Due to these limitations, we have represented our data on surgeon sex as male or female. If a graduate was found to be practicing outside the United States or complete information for the state and region of the current institution or a complete biography was not obtained for any of the FMIGS graduates above, they were excluded from analysis. The United States was split into four regions: Northeast (including Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island, Vermont, New Jersey, New York, and Pennsylvania), South (including Delaware, Florida, Georgia, Maryland, North Carolina, South Carolina, Virginia, Washington DC, West Virginia, Alabama, Kentucky, Mississippi, Tennessee, Arkansas, Louisiana, Oklahoma, and Texas), Midwest (including Illinois, Indiana, Michigan, Ohio, Wisconsin, Iowa, Kansas, Minnesota, Missouri, Nebraska, North Dakota, and South Dakota), and West (including Arizona, Colorado, Idaho, Montana, Nevada, New Mexico, Utah, Wyoming, Alaska, Hawaii, Oregon, and Washington). These designations are based on United States Census Bureau statistical regions. 10 The biography text was uploaded into the Linguistic Inquiry and Word Count (LiWC)—22 Software and analyzed. LiWC is a validated analysis software utilized previously to analyze linguistic content in other medical fields.11,12 LiWC output variables are designed to be interpreted without additional specialist training.
Data were reviewed by P.S., T.K., and K.H. Word count (WC) was obtained from the LiWC-22, and the following summary statistics (based on previous studies performed in this area11,12) were obtained: Analytic, Clout, Authentic, and Tone. The summary statistics are reported as percentiles ranging from 1 to 99 that were based on standardized scores as calculated by LiWC. LiWC derived these algorithms from their own empirical research. Analytical thinking is represented by the statistic “Analytic,” which captures how people use words that suggest formal, logical thinking. 13 The “Clout” statistic refers to the confidence level or social status indicated in the writing. 14 Authenticity is measured by “Authentic,” which reflects the degree to which a person is self-monitoring or speaking about themselves in an honest way. 15 Emotional tone is measured by ‘Tone’, 16 which includes the entire range of positive and negative tones: the higher the number, the more positive the tone.
Secondary variables included percentages of words provided automatically by the LiWC Software. For example, the variable “we” would be the percent of times “we” was used in the text.
Statistical analyses
RStudio was utilized to perform statistical and summary analysis. A Type II Multiple Analysis of Variance (MANOVA) test was performed for each variable (sex, graduation year, region, and state) and all output variables from LiWC (including WC, Analytic, Clout, Authentic, and more). This initial MANOVA analysis allowed for simultaneous analysis of differences between multiple dependent LiWC output variables. Following this, a univariate one-way ANOVA was utilized to understand which specific dependent variables were contributing to the significant effects observed in the MANOVA. Each LiWC output variable and each independent variable, including sex, graduation year, region, and state, were analyzed individually. Pairwise comparisons for region and graduation year were also performed.
Results
Demographics
A total of 268 of 404 participants were eligible for inclusion—Table 1 displays a summary of the sociodemographic characteristics of this study cohort. Of the eligible participants, 202 (75.3%) were female and 66 (24.7%) were male. For regions of the United States, 72 (26.9%) surgeons, 83 (31.0%), 44 (16.4%), and 69 (25.8%) were from the Northeast, South, Midwest, and West, respectively. The cohort included physicians who graduated between 2011 and 2021. The most represented graduating years were 2013, 2020, 2019, and 2021, with 29 (10.8%), 27 (10.1%), 28 (10.5%), and 27 (10.1%), respectively. The cohort included physicians from 40 states within the United States (Table 1).
Summary of Cohort
Linguistic analyses
See Figures 1–2 for a visual representation of linguistic output variables by sex, and region of practice. The average WC for female biographies was 194.7 versus 182 for male ones. The average analytic statistics for female biographies was 87.7; clout was 68.4, authentic was 15.4, and tone was 55.6 vs. 88.1, 67.1, 19.6, and 53.7 for males, respectively (Table 2).
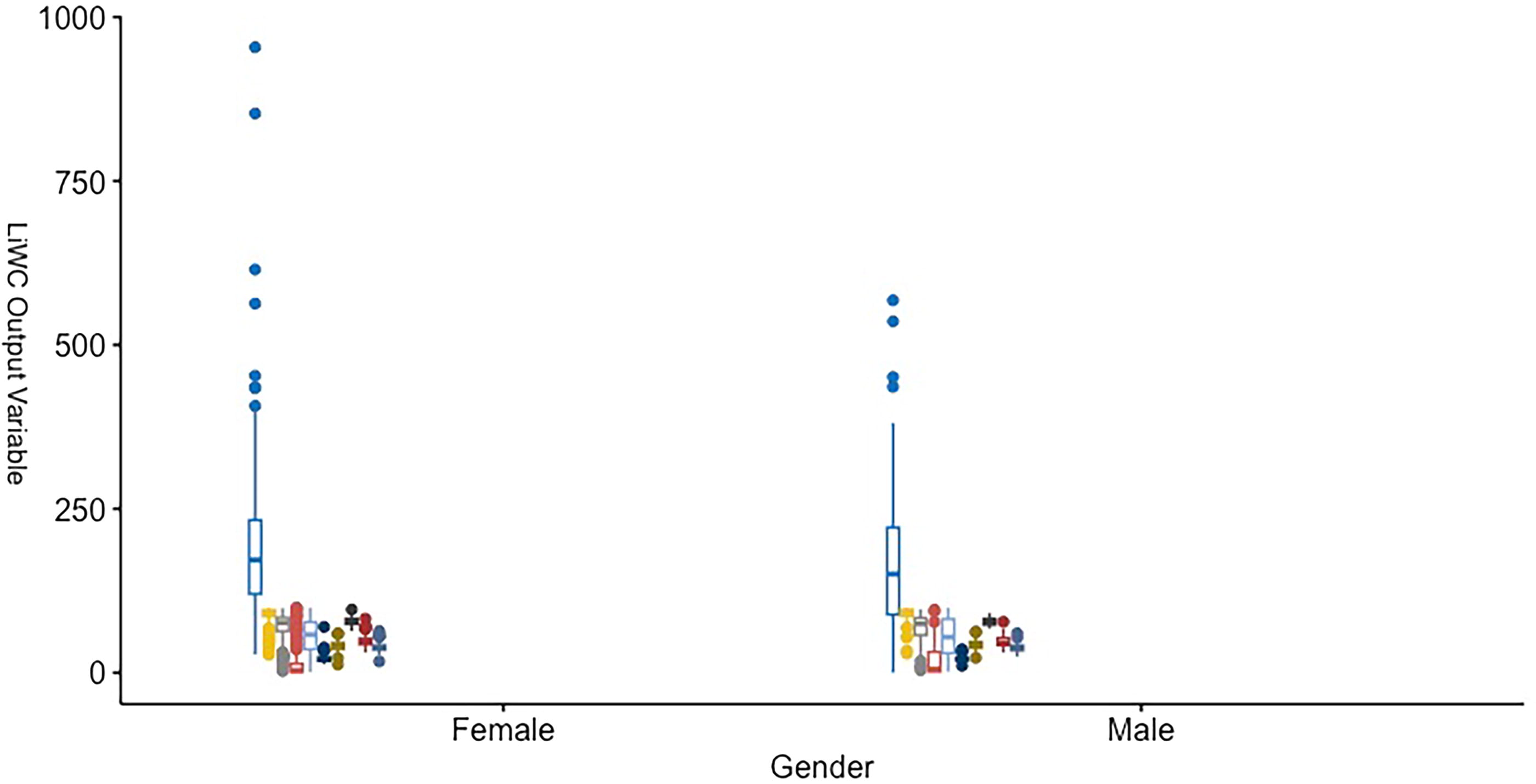
Linguistic Output Variable by Gender.
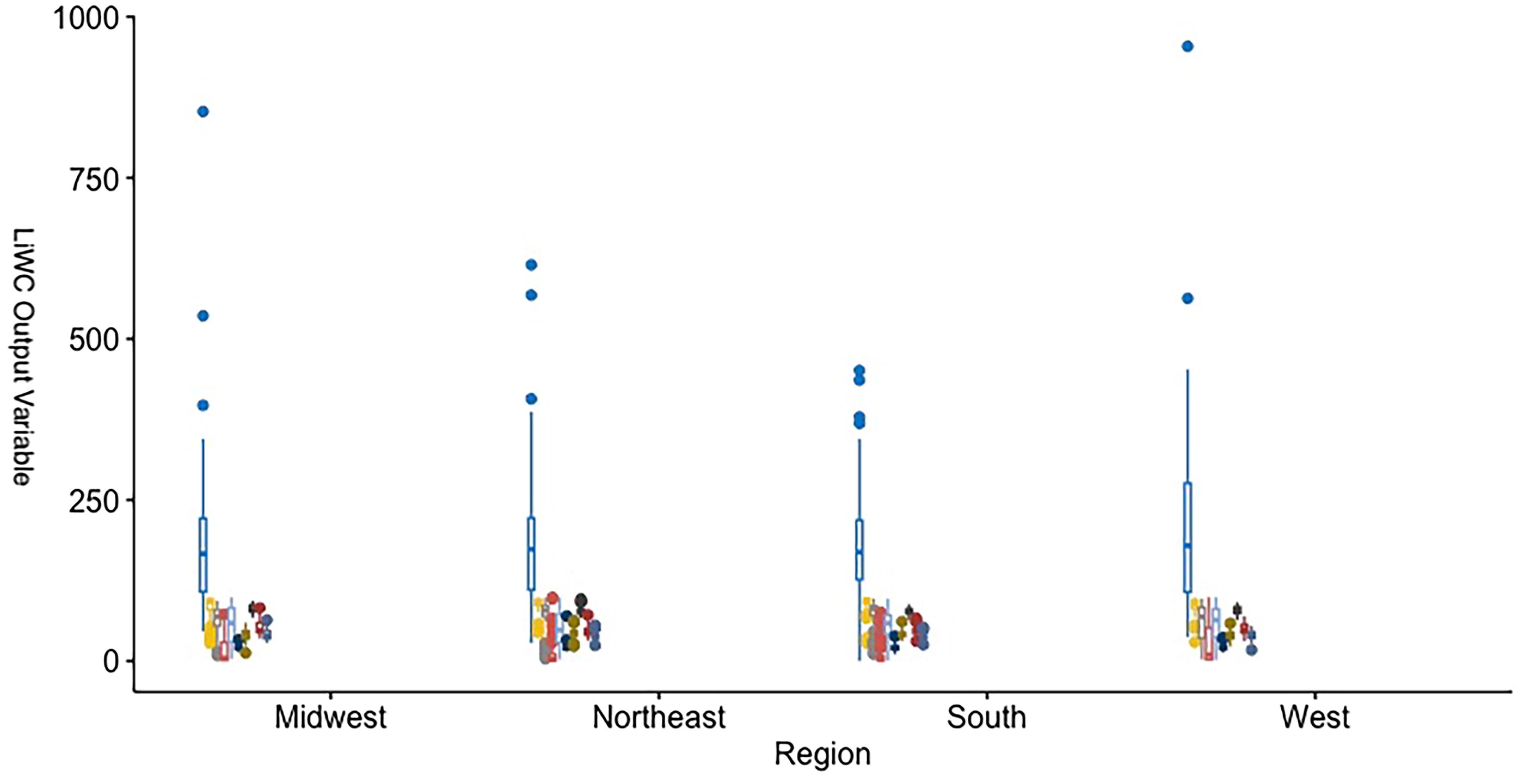
Linguistic Output Variable by Region of Current Practice.
Average Output Variables by Sex
Biographies from the Western region of the United States had the highest average word count (211.8), and the South (183.4) had the lowest. The South had the highest average analytic variable (90.9), and the Midwest had the lowest (82.3). The West scored highest on authenticity (27.8), and the South scored the lowest (9.1). The West also had the most positive tone (58.4) versus the Northeast at 50.8 (Table 3).
Average Output Variables by Region
WC was highest in graduation year 2013 (232.4) and lowest in 2015 (160.9). Analytic was highest in 2014 (92.1) and lowest in 2018 (85.7). Clout was highest in 2020 (72.8) and lowest in 2019 (62.2). Authenticity was highest in 2019 (21.2) and lowest in 2020 (12.2). Tone was most positive in 2017 (65.7) and most negative in 2018 (47.6) (Table 4).
Average Output Variables by Graduating Year
No significant relationship was found between sex or any of the main output variables from the linguistic software. Overall, state (p = 0.028) and region (p = 2 × 10−4) had a significant relationship to output variables from LiWC. Region of practice was significantly related to the level of analytical thinking (p = 0.081) represented in a biography, as well as Clout (p = 0.004) and Authenticity (p = 1 × 10−4). State of practice was significantly related to Analytic (p = 0.010) (Table 4).
When comparing different regions and states pairwise, authenticity was significantly higher in the West than in the Northeast (p = 0.009) and South (p = 0.001). Clout was higher in the South than in the Midwest (p = 0.031) and West (p = 0.001) and higher in the Northeast than in the West (p = 0.026) (Table 5).
Significant Pairwise Differences
Discussion
In this national, cross-sectional survey of FMIGS graduates, region and state of practice significantly impacted FMIGS biographies. Word count, authenticity, analytical thinking, and clout varied based on location. This relationship suggests that surgeon representation differs between geographical regions and can even differ from state to state within the same region.
Pairwise comparisons revealed some disaggregated differences about authenticity and clout by region, specifically that the Western United States had more “authentic” biographies than the Northeast or South. Interestingly, the Northeast and South both scored higher on Clout than the West did, implying that the social status and confidence with which physicians represent themselves may be more important to patients in these areas than markers of authenticity.
This regional variation may be explained by an emerging subarea of study called geographical psychology, which describes the spatial clustering of psychological characteristics. It hypothesizes that social and ecological influences and selective migration are responsible for various regions’ different “personalities.” 17 Our data may be placed in the context of other research investigating this hypothesis. One study outlines three different personalities of regions across the US as Friendly & Conventional (Midwest area), Relaxed & Creative (West), and Temperamental & Uninhibited (Northeast), with Southern states falling more within Friendly & Conventional. 18 Suppose the Western region of the US is more relaxed and adventurous than the other regions, as described by the study. In that case, the physicians in this area might also focus less on social status and words that ascribe Clout in biographical information, as found in this article. It would then follow that language to present themselves as “authentic” is of greater importance to help them appeal to a population that prefers individualism and tolerance. This could also explain why Clout is more important than authenticity for physicians in the South, as the Southern population tends to follow convention based on the aforementioned personalities. The Northeast also tends to score higher on “neuroticism,” which could help explain why Clout was more important than authenticity for physicians here than in the West. 19
Notably, as most of the physicians included in this study were practicing in or near urban centers and these regional differences persisted, meaning that regional differences also supersede urban and rural differences. It also reinforces the disparities in access to MIGS care between rural and urban areas.
It is known that health care access and treatment are closely related to a patient's location. During the COVID-19 pandemic, significant treatment disparities were observed across various areas of the United States, including delayed care rates. 20 Social Determinants of Health (SDOH) continue to be an essential factor in public health discussions across the United States, as more research makes it clear that numerous factors beyond the operating room may impact a patient's ability to recover and thrive postoperatively. SDOH includes socioeconomic indicators such as income or education and encompasses religion and culture. 21 As such, SDOH factors vary across the United States, and locations and regions also change. 21 It would follow that patient preferences for physicians would also vary by location, which could alter how a physician self-represents.
There are limitations to this study. Of the total biographic data, 75% was from female physicians, which can make it more challenging to ascertain significant relationships due to differences in sample size between sexes. Having a more proportionate representation of males and females may have provided a more accurate analysis of the differences in language used by each sex to describe their medical practice. In addition, a greater proportion of graduates that were excluded from analysis were foreign medical graduates (FMG) (having completed medical school outside the United States), resulting in possible underrepresentation of FMGs in our analysis. Some physicians had video biographies; the transcripts of those videos were not analyzed and may have led to an alternate analytic output. There was no standard location from which surgeon biographies were obtained—some were obtained from private practice sites, while others came from academic or personal sites. Most of the biographies obtained were from surgeons practicing at academic institutions or teaching hospitals, thus making it hard to generalize these findings to physicians at private practices or community hospitals. Different websites generally target different audiences and carry a different context, likely impacting how a biography is written. Strengths of this study include the strong statistical methodology used to analyze LiWC output as well as it being one of the first to investigate linguistic differences in physician biographies.
Online physician biographies may be a tool to understand patient preferences and perhaps even implicit biases from the patient or physician. Further research should be done to understand market characteristics and practice patterns that can potentially elucidate what drives biographical characteristics’ importance and whether they impact patient care.
Footnotes
Acknowledgments
The authors would like to acknowledge Northwestern University for its support in this scholarly endeavor.
Authors’ Contributions
P.S.: Conceptualization (lead), methodology (lead), formal analysis (lead), investigation (lead), methodology (lead), project administration (lead), writing—original draft (lead), writing—review and editing (lead), visualization (lead). T.K.: Methodology (supporting), investigation (supporting), writing—original draft (supporting), writing—review and editing (supporting), visualization (supporting). K.H.: Investigation (supporting), writing—original draft (supporting), visualization (supporting). A.A.E.: Conceptualization (supporting), methodology (supporting), investigation (supporting), resources (supporting), writing—review and editing (supporting). L.Y.: Writing—review and editing (supporting), visualization (supporting). M.P.M.: Conceptualization (lead), resources (lead), supervision (lead), writing—review and editing (supporting).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.