
Abstract
This narrative review explores the main surgical techniques for labiaplasty in the treatment of labial hypertrophy, focusing on their safety, efficacy, and recommendations according to the anatomical typology of the labia minora. Studies published between 2000 and 2023 were reviewed, selected according to predefined criteria, and reported clinical outcomes of reduction labiaplasty. Complications, patient satisfaction, and functional outcomes were analyzed based on available quantitative data. The most used techniques, such as wedge resection and longitudinal resection, showed complication rates below 5% and patient satisfaction levels exceeding 90%. However, a lack of standardization in the definition of hypertrophy and in the criteria for choosing the appropriate surgical technique was identified. Individualized surgical planning based on anatomical characteristics and patient expectations is crucial to optimize aesthetic and functional outcomes while minimizing complications.
Introduction
Reduction labiaplasty (RLP) has established itself as a surgical procedure of growing relevance in the field of aesthetic and functional gynecology. 1 Targeted at the treatment of labia minora hypertrophy, a condition of multifactorial etiology, RLP addresses both aesthetic and functional demands of patients. The definition of hypertrophy, while variable in the literature, typically focuses on the protrusion of the labia minora beyond the labia majora, often accompanied by clitoral hood hypertrophy. 2 Despite the lack of consensus regarding a standardized classification, it is widely accepted that this condition can generate physical, psychological, and sexual discomfort, significantly affecting the quality of life of patients. 2
In recent years, the demand for labiaplasties has grown exponentially. Recent data from the American Society of Aesthetic Plastic Surgeons report a 217.2% increase in the number of procedures since 2012, reflecting greater acceptance and pursuit of such interventions.1,3,4 However, this increase has also revealed significant challenges for surgeons, including the need to align patients’ realistic expectations with surgical outcomes. Similarly, the rise of revision labiaplasties, or “botched labiaplasties,” highlights the lack of adequate training among some professionals in safe and effective techniques.
Labia minora hypertrophy rarely occurs in isolation and must be evaluated in the context of adjacent anatomical structures, particularly the labia majora and the clitoral hood. Surgical alterations to the labia minora may influence the contour and functionality of these surrounding structures, making a comprehensive preoperative assessment essential.1–3 For instance, excessive reduction of the labia minora without considering its relationship to the clitoral hood may lead to an imbalance that disrupts the natural aesthetics or even the protective functions of the vulva.1,3 Similarly, tension changes due to resection can affect the labia majora, resulting in visible asymmetry or altered volume distribution.1,3 To achieve optimal results, the surgeon must address the patient’s expectations while maintaining harmony among all vulvar components, ensuring functional and aesthetic integration.
The concept of ideal external female genital anatomy, while subjective, has been explored to provide guidelines for aesthetically pleasing outcomes in surgical procedures such as RLP. Frojo et al. 5 utilized crowdsourcing to evaluate preferences for external female genital proportions, identifying a preferred labia majora-to-labia minora width ratio of approximately 3:1, with mid-range labia minora widths being most favored. 5 Clitoral hood length showed minimal impact on preferences. 5 These findings provide an evidence-based framework for maintaining aesthetic harmony during RLP.
The vascular anatomy of the external genitalia is a critical consideration in RLP, as inadequate preservation of blood supply can lead to wound healing complications and increased risk of tissue necrosis.1,3 The labia majora and minora receive blood supply predominantly from branches of the internal pudendal artery, including the posterior labial branches.1,3
Currently, multiple techniques have been described for performing RLP, including linear excision (trim) and wedge excision, as well as techniques such as skin-sparing and Z-plasty, with variations that include the use of lasers.1,6–8 However, there is no technique in the literature that is considered the gold standard. Reported complication rates are low, ranging from 2% to 5%, and patient satisfaction exceeds 90%.1,3 The variability in outcomes and the lack of standardization in the selection of techniques highlight the importance of a thorough review of the literature, which can guide professionals toward the most suitable surgical choice based on the anatomical profile and expectations of each patient.
This article aims to provide a critical and detailed review of the available surgical techniques for RLP, analyzing current findings in the literature and offering a comprehensive perspective to help optimize clinical outcomes and reduce complications in such procedures.
Materials and Methods
A comprehensive literature search was conducted on the surgical techniques used in RLP, focusing on efficacy, safety, complications, and patient satisfaction. Articles published between January 2010 and September 2024 were collected through electronic search systems such as Google Scholar, MEDLINE, PubMed, Scopus, and the Cochrane Library, as well as secondary resources like books and conference proceedings.
The search terms included combinations of “labiaplasty,” “labia minora hypertrophy,” “surgical techniques,” “wedge resection,” “longitudinal resection,” “surgical complications,” “patient satisfaction,” and “functional outcomes.” The resulting articles from these searches and the relevant references cited within those articles were reviewed. Included in the review were studies that met the following inclusion criteria: (i) studies focused on the evaluation of surgical techniques for labiaplasty and (ii) studies assessing complications, patient satisfaction, and/or functional improvements related to RLP.
The exclusion criteria were as follows: (i) studies that included only expert opinions without clinical data; (ii) articles focusing exclusively on labiaplasties for post-traumatic or oncological reconstructive purposes; and (iii) studies lacking postoperative follow-up or clearly reported outcomes.
Two independent reviewers carried out the selection of studies based on the inclusion and exclusion criteria. In cases of disagreement, a third reviewer intervened to reach a consensus decision.
Hypertrophy of the labia minora
Hypertrophy of the labia minora is commonly defined as the growth or increase in size of the labia minora in relation to the labia majora, such that the former protrudes beyond the plane of the latter when at rest. 2 However, there is considerable lack of standardization in the exact definition of “hypertrophy” in the scientific literature. The difficulty in establishing a consensus is partly due to the considerable anatomical variability among women and the absence of universal criteria that define normality in vulvar morphology. 9 Some authors suggest that any protrusion greater than 1–2 cm could be considered hypertrophy, while others propose that classification should be based more on functional symptoms and the discomfort perceived by the patient than on strictly anatomical measurements.9,10 This lack of standardization not only creates ambiguity in diagnosis but also complicates surgical indications and the comparison of results across different studies.
In this context, it is essential to remember that variations in vulvar anatomy are normal, and not all protrusions or asymmetries should be considered pathological or automatic indications for surgical intervention.9,11 It is vital to differentiate between the aesthetic and functional reasons that lead patients to request labiaplasties, as the latter represents the primary medical indication for the treatment of hypertrophy.
Labia minora hypertrophy is a condition of multifactorial etiology.
2
Among the most associated factors for its development are:
Congenital factors: In many women, labia minora hypertrophy is present from birth and is associated with normal physiological development. Congenital hypertrophy may manifest during childhood, although it is more notable during adolescence when hormonal changes intensify the growth of genital tissues. Congenital variations may be linked to differences in connective tissue arrangement or collagen proportion in the labia minora, leading to increased growth or protrusion.
2
Hormonal factors: Hormonal fluctuations, particularly those related to estrogen, play an important role in the etiology of labia minora hypertrophy.2,12 These hormones directly influence the structure and elasticity of vulvar tissue. An increase in estrogen levels during puberty or pregnancy can promote the growth of the labia minora. Prolonged use of hormonal contraceptives has also been suggested to affect the morphology of the external genitalia.
2
Traumatic factors: Repeated trauma to the genital area, such as that caused by sports activities, tight clothing, or certain types of sexual activity, can result in hypertrophy as an adaptive response of the tissue. These microtraumas cause chronic inflammation and stimulate compensatory growth of the labia minora, eventually leading to increased protrusion.
2
Infectious factors: Recurrent infections in the vulvovaginal area, such as vaginitis or vulvitis, have also been implicated in the etiology of hypertrophy.
2
Chronic inflammation caused by bacterial, fungal, or viral infections can contribute to the enlargement of the labia minora. In these cases, tissue growth may be a response to persistent inflammation and changes in collagen structure induced by repeated infections.
2
One of the main difficulties in the surgical approach to labia minora hypertrophy lies in the absence of a standardized anatomical classification. Although various classifications have been proposed in the literature, none have been universally accepted. Among the most recognized are:
Motakef et al. classification: This system classifies labia minora hypertrophy into four grades based on the length of protrusion beyond the labia majora.
13
This classification is simple and based on objective measurements, making it useful for selecting candidates for labiaplasty. However, its strictly anatomical approach does not always reflect the patient’s functional or psychological discomfort.
13
González-Isaza classification: This proposes a more detailed assessment, considering not only the length of the labia minora but also their relationship with the clitoral hood and the specific morphological characteristics of each patient.
14
This topographical classification suggests a personalized surgical approach, facilitating the planning of the intervention according to individual anatomical variants. Gress classification: Based on symmetry and the degree of hypertrophy, this classification allows for correlations with the aesthetic and functional expectations of patients and is designed to guide the choice of the most appropriate surgical technique.
15
Each of these classifications presents advantages and limitations. However, they all agree on the importance of conducting a comprehensive evaluation of vulvar anatomy before opting for surgical intervention.1,3 The choice of surgical technique should be personalized according to the anatomical characteristics of the patient, their expectations, and the underlying clinical indication.
Surgical techniques for RLP
The selection of the appropriate surgical technique for RLP is critical to achieving the best functional and aesthetic outcomes while minimizing the risk of complications.
Wedge resection
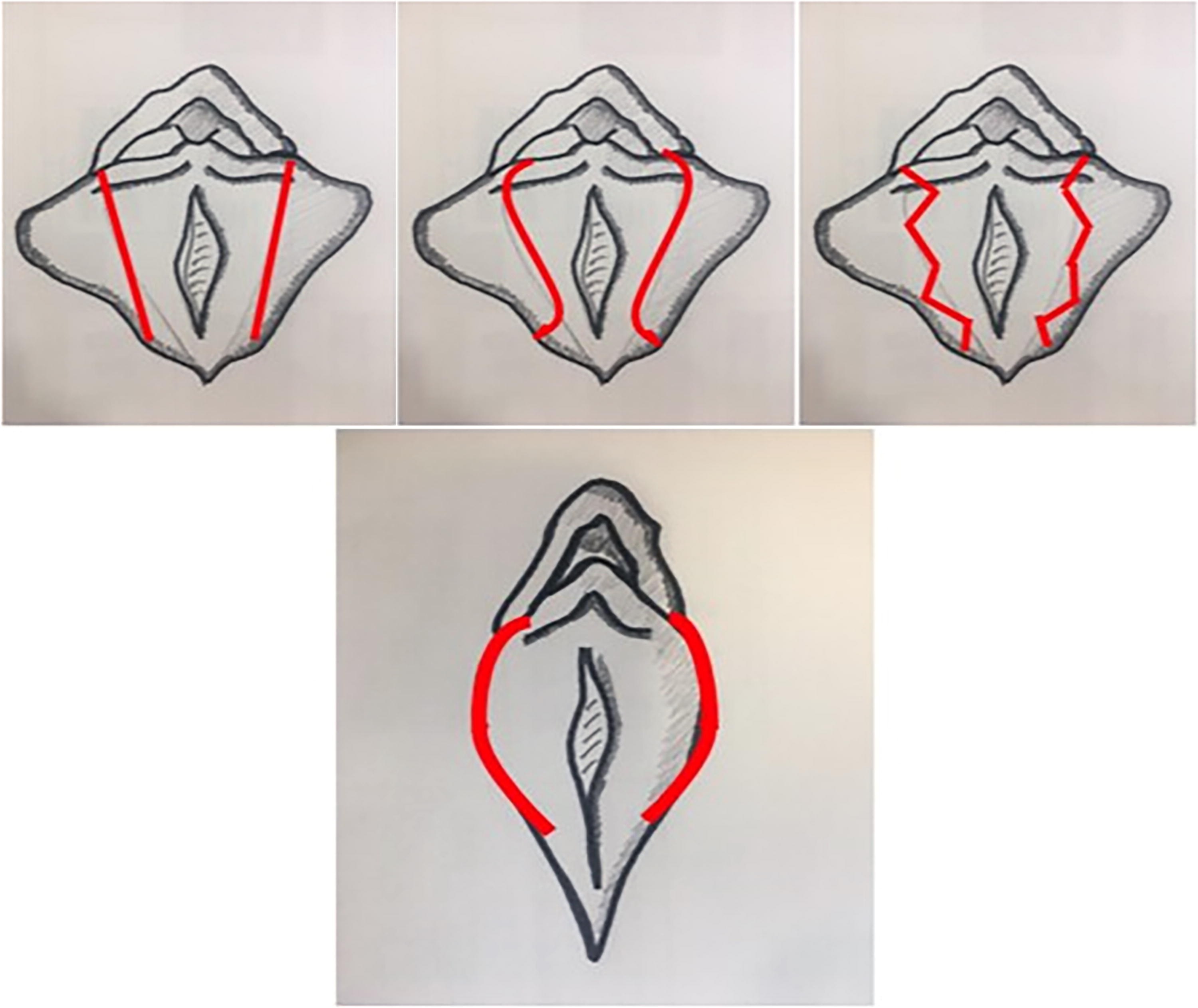
Wedge resection involves the removal of a triangular wedge of tissue from the midsection of the labia minora (Fig. 1). 16 This technique preserves the natural edge of the labia minora, which is one of its main aesthetic advantages. Central resections can be performed (Fig. 2) or in more specific areas depending on the morphology and individual needs of the patient. Variants of the technique include complete (Fig. 3) or partial wedge resections and wedge resections with de-epithelialization (Fig. 4), which can be adapted to the case.17,18 Suturing is done along the inner edge of the defect, facilitating a more discreet healing process.16,17
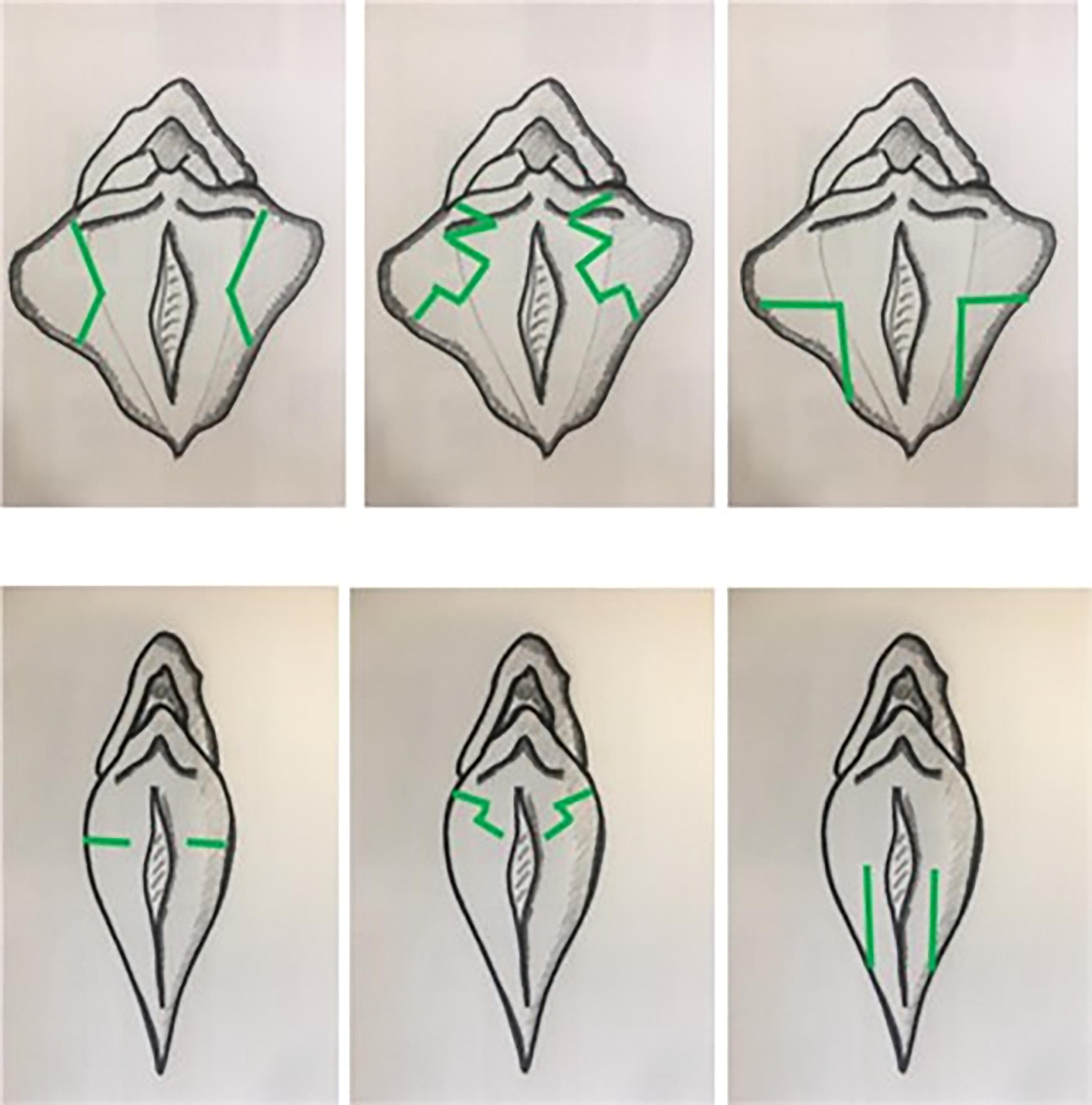
Wedge resection. Original work. Adapted from Özer et al. 1
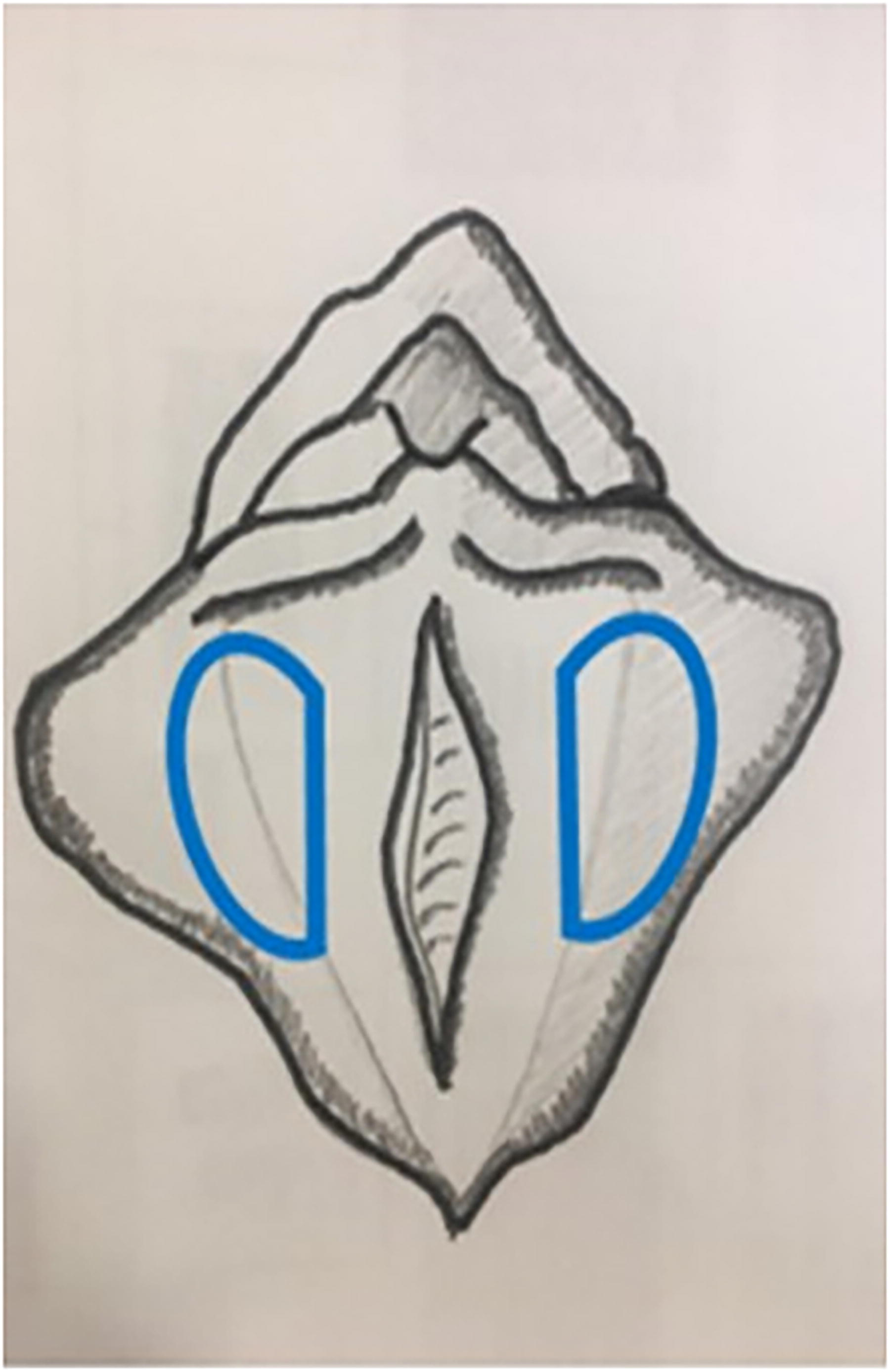
Central resection. Original work. Adapted from Özer et al. 1

Complete wedge resection technique and via de-epithelialization. Original work. Adapted from Hamori et al. 6

Choi de-epithelialization technique. Original work. Adapted from Choi et al. 17
Surgeons must ensure meticulous hemostasis while avoiding overtension on the remaining tissue, which may compromise blood flow and delay healing.16,17
Wedge resection presents several advantages, particularly in terms of preserving anatomical and aesthetic integrity. 16 One of its primary benefits is the preservation of the natural edge of the labia minora, which helps maintain the vulvar aesthetics postoperatively.16,17 This technique significantly reduces the risk of visible scarring, as the incisions are placed in less conspicuous areas, enhancing the overall aesthetic outcomes. 16 Wedge resection carries a lower risk of clitoral detachment compared to more extensive surgical approaches, as it minimizes the chance of damaging the clitoral hood, a key consideration for functional and sensory preservation.16,17
The main complications include wound dehiscence, particularly if the wedge is too deep or subjected to excessive tension during suturing.16,18 Tissue necrosis has also been reported in cases where vascularization is not adequately preserved. However, the overall complication rate is relatively low.1,18,19
Recent studies have demonstrated that wedge labioplasty has a high satisfaction rate, averaging 90% in patient follow-up series.16,17,19 A meta-analysis of labioplasty procedures that included wedge resection reported complication rates below 5%, with dehiscence being the most common complication. 19
Longitudinal resection
Longitudinal resection or “trim” technique involves removing a segment along the edge of the labia minora. 7 In this procedure, a linear incision is made to uniformly reduce the overall size of the labia minora (Fig. 5). This method is one of the oldest and most widely practiced surgical procedures and can be performed using either a scalpel or laser.7,8,20
Longitudinal resection. Original work. Adapted from Özer et al. 1
While versatile in addressing significant hypertrophy, this technique poses a risk of impairing superficial blood supply if not carefully executed. Preserving the lateral edges and minimizing excessive tension during the closure are essential to maintaining perfusion7,20
The longitudinal resection technique offers several advantages that contribute to its widespread use. First, its technical simplicity makes the procedure relatively straightforward and quick, making it a suitable option for surgeons with varying levels of experience.7,20 This ease of execution does not compromise its effectiveness, particularly in cases where significant tissue reduction is required. Second, the versatility of this technique allows for the removal of large amounts of tissue, making it especially appropriate for patients with severe labial hypertrophy.7,20 Last, the immediate and noticeable reduction achieved through longitudinal resection often enhances the patient’s initial satisfaction, as the results are immediately visible postoperatively. 20
Common complications include visible scarring along the free edge of the labia minora, which can alter the natural aesthetic appearance of the vulva. 19 Loss of pigmentation at the edges has also been reported, which may be a concern for some patients. Other complications include hypersensitivity in the treated area and scar contractures.1,19
Comparative studies have shown that while longitudinal resection is effective in reducing the labia minora, it tends to have a higher rate of aesthetic complications due to the loss of the natural labial edge.7,8,20
Central Z resection and variants
Central Z resection is a less common technique involving the creation of a Z-shaped flap, similar to reconstruction techniques used in other surgical areas. This procedure is indicated in cases where symmetry and proportion of labial tissue are essential. 21 The Z-plasty design, specifically, repositions flaps of tissue without excising significant vascular structures, thereby maintaining adequate perfusion to the surrounding areas.21,22 This approach reduces the risk of ischemia and promotes optimal wound healing. However, improper planning of incision angles or excessive tension on the tissue flaps can impair microcirculation, increasing the risk of wound dehiscence or delayed healing. 21 The Z technique allows for tissue redistribution without direct linear resection, which may better preserve natural texture and elasticity (Fig. 6). 21 This technique is especially useful for patients with moderate hypertrophy and significant labial asymmetry, and it is beneficial in cases where minimizing visible scarring and preserving tissue functionality is desired.
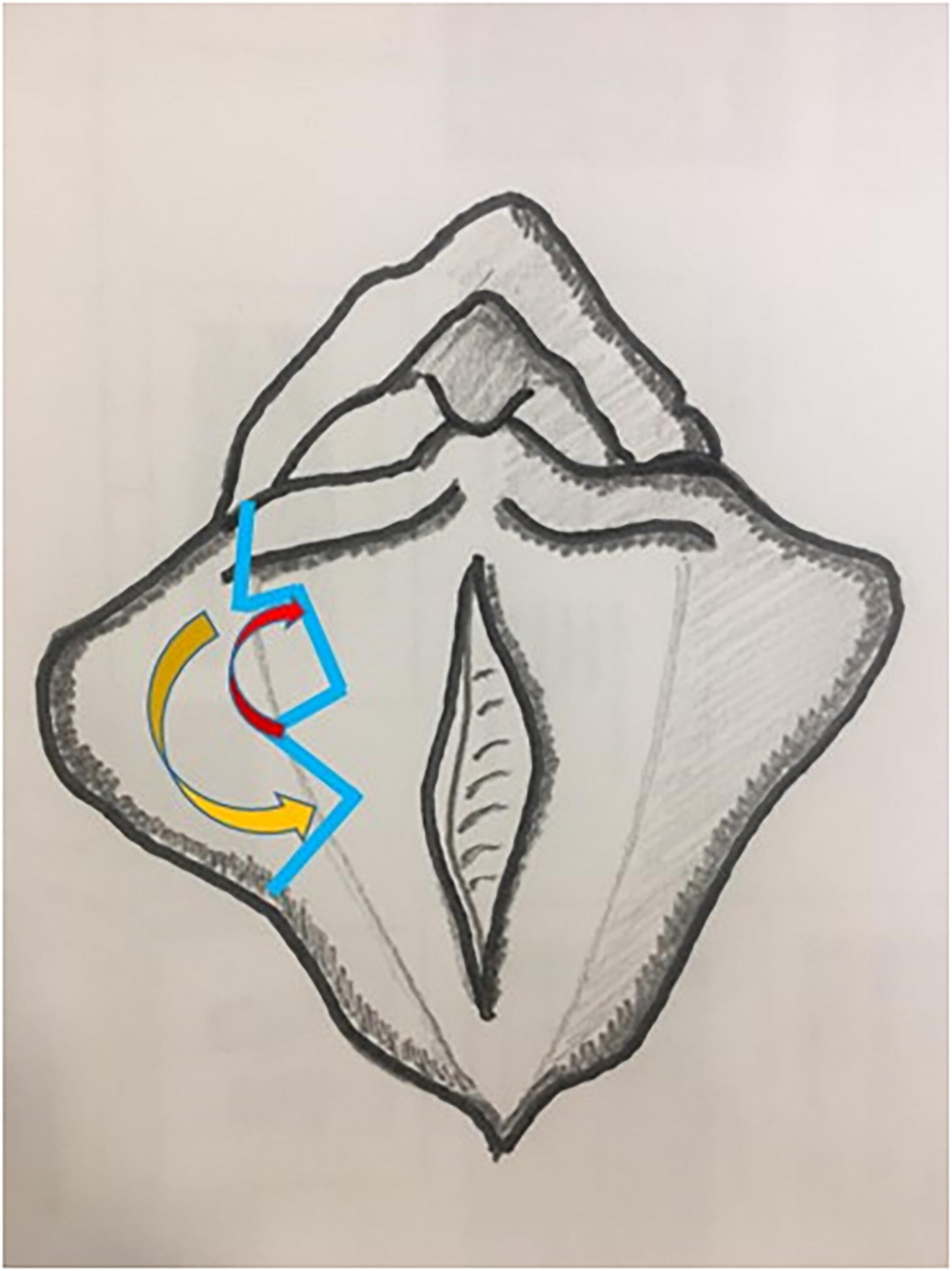
Z-plasty. Original work. Adapted from Willis et al. 23
While less frequently used, studies have shown good aesthetic and functional results with the Z technique. 21 However, the learning curve for this procedure is higher, and it is recommended for surgeons with advanced experience in labioplasty.
Comparative studies between RLP techniques show that both wedge and longitudinal resections are viable options, but each has specific indications. Wedge resection, while technically more complex, offers a significant advantage in maintaining the natural appearance and reducing the risk of visible scarring.1,19 Longitudinal resection is preferred in cases of severe hypertrophy or where the simplicity of the procedure is a priority.1,19 The Z technique, though less common, offers an option in cases of asymmetry and when minimizing scarring is prioritized. 21
Criteria for technique selection
The choice of the appropriate surgical technique for RLP depends on a series of anatomical factors and the patient’s expectations.22,24 Key anatomical factors include the length of the labia minora, symmetry, the relationship with the clitoral hood, and the texture of the tissue.24,25 Additionally, it is essential to discuss the patient’s aesthetic and functional expectations, as these can significantly influence the surgical decision. 25 Patients with moderate hypertrophy who seek a natural appearance may benefit more from wedge resection, while those with significant hypertrophy may require longitudinal resection.1,25
The surgical approach should always be individualized, considering not only the anatomical characteristics but also the psychological and emotional expectations of the patient to ensure a satisfactory and functional outcome.22,25
Complications and Postoperative Management
RLP, while generally a safe procedure, carries the risk of postoperative complications, both minor and major. 1 Proper management of these complications is essential to ensure optimal recovery and minimize the impact on the quality of life for patients.
Minor complications
Minor complications are relatively common but are typically easy to manage if diagnosed and treated promptly.1,19
Infections: Despite aseptic techniques during the procedure, infections can arise, especially if postoperative care regimens are not properly followed. Infections typically present within the first week postoperatively, with signs such as redness, swelling, pain, and purulent discharge. Early antibiotic treatment and proper hygiene are key to resolution. Dehiscence: Wound opening or dehiscence is a common complication, particularly in wedge resection, where tissue under greater tension may fail. To minimize this risk, postoperative control of physical exertion and avoidance of premature sexual activity are essential. In cases of mild dehiscence, conservative management with secondary healing is preferred, but severe cases may require surgical revision. Abnormal healing: The formation of hypertrophic or keloid scars is rare but can occur in genetically predisposed patients. The use of scar creams, silicone dressings, or steroid injections may help improve the appearance of abnormal scars. Surgical revision of scars is reserved for cases where scars compromise vulvar aesthetics or functionality.
Major complications
Major complications are infrequent but can significantly impact the quality of life for patients if not managed correctly.1,19
Loss of sensitivity: Loss of sensitivity in the labia minora or periclitoral area is a complication that affects both sexual function and overall quality of life. This complication is often related to excessive manipulation of nerve endings during surgery. While sensitivity usually recovers over time, there are cases where damage is irreversible. Scar retraction: Scar retraction can lead to excessive reduction of the labia minora, causing discomfort or sexual dysfunction. This issue is more common with the longitudinal resection technique, where contractile scars can alter anatomy. Management includes advanced healing therapies or, in more severe cases, corrective surgery. Long-term functional issues: Labiaplasty can sometimes result in functional complications, such as dyspareunia (pain during sexual intercourse) or alterations in vaginal lubrication. These problems may arise from tense or retracted scars or excessive damage to the vaginal mucosa during the procedure.
A review of the literature reveals that overall complication rates for labiaplasty are relatively low, ranging from 2% to 5%,13,19 with suture dehiscence being the most common complication. 19
Recommended postoperative measures
Postoperative measures play a crucial role in preventing complications and optimizing outcomes1,19:
Strict hygiene: Adequate hygiene of the surgical area with mild antiseptic solutions is recommended to prevent infections. Rest and physical exertion control: Any intense physical activity, use of tight clothing, or sexual activity should be avoided for at least 6 weeks postsurgery to reduce the risk of dehiscence and abnormal healing. Healing therapies: The use of moisturizing and healing creams, as well as silicone dressings, may help prevent the formation of pathological scars.
Patient Satisfaction and Functional Outcomes
Patient satisfaction following labiaplasty is evaluated in terms of both aesthetic results and functional improvements.19,20 Both aspects are crucial for a comprehensive assessment of the success of the surgery.
Aesthetic results
Studies report that aesthetic satisfaction is generally high after RLP. In recent studies, more than 90% of patients expressed satisfaction with the aesthetic outcomes. 20 Wedge resection has shown slightly higher rates of aesthetic satisfaction compared to longitudinal resection due to the preservation of the natural edge of the labia minora. 21
Functional improvements
In addition to aesthetic benefits, patients report significant functional improvements. The reduction of the labia minora alleviates symptoms of irritation, discomfort during sports, and difficulties when wearing tight clothing. Improvements in sexual function have also been reported, as many patients experience greater comfort during intercourse and an enhancement in their self-esteem.26,27 Recent studies resulted in a significant improvement in genital self-image and sexual function of women, according to assessments from the Female Sexual Function Index (FSFI) and Female Genital Self-Image Scale (FGSIS), with notable increases in scores from both questionnaires, reinforcing the positive impact of surgery on sexual and psychological quality of life. 26
Satisfaction studies
In a meta-analysis of 53 studies, overall satisfaction rates were high for all RLP methods. 20
What about the “not operating” option?
It is important to consider that, in some cases, the option of “not operating” is the most appropriate. 28 A careful analysis of the patient’s expectations, along with a psycho-sexological evaluation, may reveal that the patient’s symptoms do not justify surgical intervention. 28 Labiaplasty should not be performed solely based on aesthetic standards influenced by sociocultural factors or external pressure. 28 In cases of uncertainty or unrealistic expectations, conservative management may be preferable to surgery, thereby avoiding unnecessary complications or postoperative dissatisfaction.23,29
Limitations
The limitations of this nonsystematic review of the literature on RLP techniques include the lack of consensus on the definition of labia minora hypertrophy, which generates variability in diagnostic criteria and complicates the comparison of studies. Additionally, there is no gold standard surgical procedure, which adds complexity to the evaluation of the reviewed techniques. The heterogeneity in the methods of evaluating aesthetic and functional outcomes, along with limited postoperative follow-up in many studies, also affects the interpretation of findings. Most of the reviewed studies are retrospective, with small sample sizes and limited statistical analyses, highlighting the need for more rigorous and long-term comparative research to improve the available evidence and guide clinical practice.
The strengths of this review include a comprehensive assessment of the most used surgical techniques in RLP, providing an integrated view of the available procedures and their outcomes. Furthermore, a comparative analysis of complications and patient satisfaction is presented, facilitating better clinical decision-making. The review emphasizes the importance of surgical customization based on the patient’s anatomy and expectations, which is key to optimizing aesthetic and functional outcomes in this type of surgery.
Conclusions
RLP has established itself as one of the most requested interventions in the field of aesthetic and functional gynecology. Surgical techniques for RLP, while varied, provide good outcomes in terms of efficacy and safety, with a low rate of complications. It is essential to conduct a personalized evaluation for each patient, tailoring the surgical technique to the anatomical characteristics and individual expectations. Despite advancements, there are still areas for improvement, such as the standardization of criteria for technique selection and the management of postoperative complications. Continued research is suggested to optimize outcomes and reduce long-term complications.
Footnotes
Authors’ Contributions
The following contributions were made by the authors: J.J.E.T., M.S.-P., and R.S.B.: Project conceptualization. J.J.E.T., M.S.-P., G.R.G., and F.L.S.: Writing—original draft preparation. J.J.E.T., M.S.-P., and R.S.-B.: Writing—review and editing. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
The authors declare that they have no potential conflicts of interest regarding the research, authorship, and publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and publication of this article.