
Abstract
Background:
Clinical stage IA endometrial cancer (EC) is associated with a medium to high risk of recurrence if the histological subtype is other than grades 1 and 2 (G1/2). Despite the wide use of laparoscopic surgery (LS) for intermediate- to high-risk early EC, its impact on prognosis remains unclear. This study aimed to compare the short-term outcomes of LS and open abdominal surgery (OAS) for intermediate- to high-risk clinical stage IA EC.
Methods:
This retrospective study included 51 patients with stage IA EC diagnosed as histological types other than endometrioid carcinoma G1/2 and initially treated at our institution between 2013 and 2021. Patient outcomes were compared between LS and OAS groups following total simple hysterectomy. Survival analysis was conducted using the Kaplan–Meier method, and group differences were assessed using the log-rank test.
Results:
Intra- and postoperative complications (grade 3 or higher) did not significantly differ between LS and OAS. However, LS reduced the frequency of early postoperative complications occurring within 30 days compared to OAS. LS did not cause a significant delay in the initiation of adjuvant therapy, as reflected by the comparable median number of days between surgery and the first adjuvant chemotherapy session in both groups. Moreover, the 3-year recurrence-free and overall survival rates did not significantly differ between groups.
Conclusions:
These results indicate that short-term outcomes do not significantly vary between LS and OAS when performing simple hysterectomy, bilateral salpingo-oophorectomy, omentectomy, pelvic lymphadenectomy, and para-aortic lymphadenectomy for early-stage stage IA EC at medium-to-high risk of recurrence.
Introduction
Endometrial cancer (EC) is often detected early, with endometrioid carcinoma grades 1 and 2 being the most common histological types. In Japan, stage IA accounted for 56.7% of all EC cases in 2020, with endometrioid carcinoma grades 1 or 2 comprising 71.9% of the total cases. 1
Stage IA endometrioid subtype G1/2 EC exhibits a low risk of recurrence, with surgery being the conventional treatment. The standard surgical procedure is a simple total hysterectomy and bilateral salpingo-oophorectomy. Omentectomy and pelvic and para-aortic lymphadenectomy are also performed for staging in some cases. Traditionally, open abdominal surgery (OAS) has been the preferred surgical approach; however, recently, the use of laparoscopic surgery (LS) has become widespread. National Comprehensive Cancer Network clinical practice guidelines state that the minimally invasive approach is the standard due to low rates of surgical site infection, blood transfusion, and venous thromboembolism, shorter hospital stays, and lower treatment costs. 2 In terms of prognosis, two prospective comparative studies, a large-scale retrospective study, and a meta-analysis have shown that LS is noninferior to OAS in patients with a low risk of recurrence.3–8 As a result, LS is becoming a popular surgical approach for patients at low risk.
In contrast, if the histology is not endometrial subtype G1/2, patients with stage IA EC are at moderate-to-high risk. The standard procedure for EC removal is total hysterectomy along with bilateral adnexectomy; although it has been suggested that lymph node dissection has therapeutic significance in addition to accurate staging for patients who are at moderate-to-high risk. 9 However, no prospective comparative trial has compared the prognosis of LS and OAS for intermediate- to high-risk EC; therefore, the prognostic impact of LS remains unknown. In addition, previous retrospective studies have limitations, such as the absence of para-aortic lymphadenectomy in some of the included patients and inconsistencies in the preoperative and intraoperative oncological background (e.g., preoperative histological type, depth of muscle layer invasion, and stage).10,11 Therefore, comparative studies with standardized surgical procedures and oncological backgrounds are required.
At our institution, we treat early-stage EC with an intermediate to high risk of recurrence (clinical stage IA and histological types other than endometrioid carcinoma G1/2) using a standardized surgical procedure (simple hysterectomy + bilateral salpingectomy [oophorectomy] + omentectomy + pelvic lymphadenectomy + para-aortic lymphadenectomy), unless there are complications or age-related limitations. Thus, the surgical procedure and oncological background of our cases are consistent. Furthermore, we introduced LS in 2018, which is performed by a team that includes physicians skilled in gynecological malignancies and LS. This enables us to compare the LS and OAS approaches. Although several reports have compared the safety of laparoscopic procedures, including para-aortic lymphadenectomy, with OAS, the prognosis remains unclear.
Therefore, this study aimed to compare the short-term outcomes of LS and OAS for early-stage EC at intermediate- to high-risk of recurrence (clinical stage IA, histological types other than endometrioid carcinoma G1/2).
Materials and Methods
Study design and participants
This was a single-center, retrospective study. The inclusion criteria were patients with EC who underwent initial treatment at our institution between 2013 and 2021; clinical stage IA preoperatively and intraoperatively; and histology other than endometrioid carcinoma G1/2 preoperatively and intraoperatively. The exclusion criterion was initial surgery that did not include simple hysterectomy, bilateral salpingectomy, oophorectomy, omentectomy, pelvic lymphadenectomy, or para-aortic lymphadenectomy. Informed consent was obtained via an opt-out method on the institutional website, and patients who opted out were excluded.
We retrospectively reviewed patient medical records up to March 31, 2024. Patients were categorized into LS and OAS groups, and patient outcomes (overall survival [OS], relapse-free survival [RFS], postoperative complications, and site of recurrence) were compared. OS was defined as the time from the date of the initial surgery to the date of death from any cause or the last follow-up date, whichever came first. RFS was defined as the time from the date of the initial surgery to the date of first recurrence, progression, death from any cause, or the last follow-up date, whichever occurred earlier. Postoperative complications were assessed using the Clavien–Dindo classification for surgical complications.12,13
Ethics approval
The study adhered to the Declaration of Helsinki and was approved by the Institutional Review Board of Shizuoka Cancer Center (Approval No. J2024-30-2024-1-3).
Statistical analysis
We used Easy R (EZR, Jichi Medical University Saitama Medical Center, Japan), a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria), for all analyses.14 EZR is designed as an enhanced version of the R commander, specifically for biostatistical applications, which incorporates additional statistical functions commonly used in biostatistics. Categorical variables were analyzed using Fisher’s exact test, and continuous variables were analyzed using the Mann–Whitney U test. Survival analysis was conducted using the Kaplan–Meier method, and group differences were assessed using the log-rank test. p < 0.05 was considered statistically significant.
Surgical procedure
All patients in the LS and OAS groups underwent a simple total hysterectomy. Dissection of the anterior and posterior leaves of the vesico-uterine ligament was avoided. During LS, both fallopian tubes were ligated at their origins using clips before manipulating around the uterus. In addition, the vaginal cavity was irrigated with saline before the vaginal canal incision, and sutures were used to close the vaginal portion of the cervix. The uterine body was placed in a specimen retrieval bag during the vaginal canal incision and retrieved through the vagina after the procedure. In OAS, the fallopian tubes were grasped with Pean forceps until uterine body removal was completed; however, the vaginal portion of the cervix was not sutured. Any macroscopic lesions on the excised uterus were submitted for intraoperative histology to confirm the histological type and depth of myometrial invasion.
Pelvic lymphadenectomy involved dissection of the common iliac, external iliac, superior inguinal, internal iliac (those inside the triangle formed by the internal and external iliac arteries), obturator, and sacral lymph nodes. During LS, lymph nodes were retrieved using a trocar sleeve. In both LS and OAS, the distal part of the obturator lymph nodes was ligated with sutures or clips. In LS, the distal part of the superior inguinal lymph nodes was ligated with clips.
Para-aortic lymphadenectomy involved the dissection of lymph nodes from the lower edge of the renal veins to the level of the aortic bifurcation, including those around the aorta and inferior vena cava. Lymphatic vessels were ligated with sutures or clips at the lower edge of the renal veins.
Results
Patient characteristics
During the study period, 915 patients with EC were treated at our institution. Among them, 80 patients were diagnosed with clinical stage IA and had histological types other than endometrioid carcinoma G1/2 preoperatively and intraoperatively, of which 51 patients were included in this study: 19 and 32 patients in the LS and OAS groups, respectively (Fig. 1). The two groups did not significantly differ in terms of characteristics (age at diagnosis, Eastern Cooperative Oncology Group performance status score, body mass index, American Society of Anesthesiologists physical status, obstetric history, menopausal status, history of abdominal surgery, uterine size, and tumor markers) (Table 1). Intraoperative rapid diagnosis was performed in 73.7% and 78.1% of patients in the LS and OAS groups, respectively (p = 0.74).
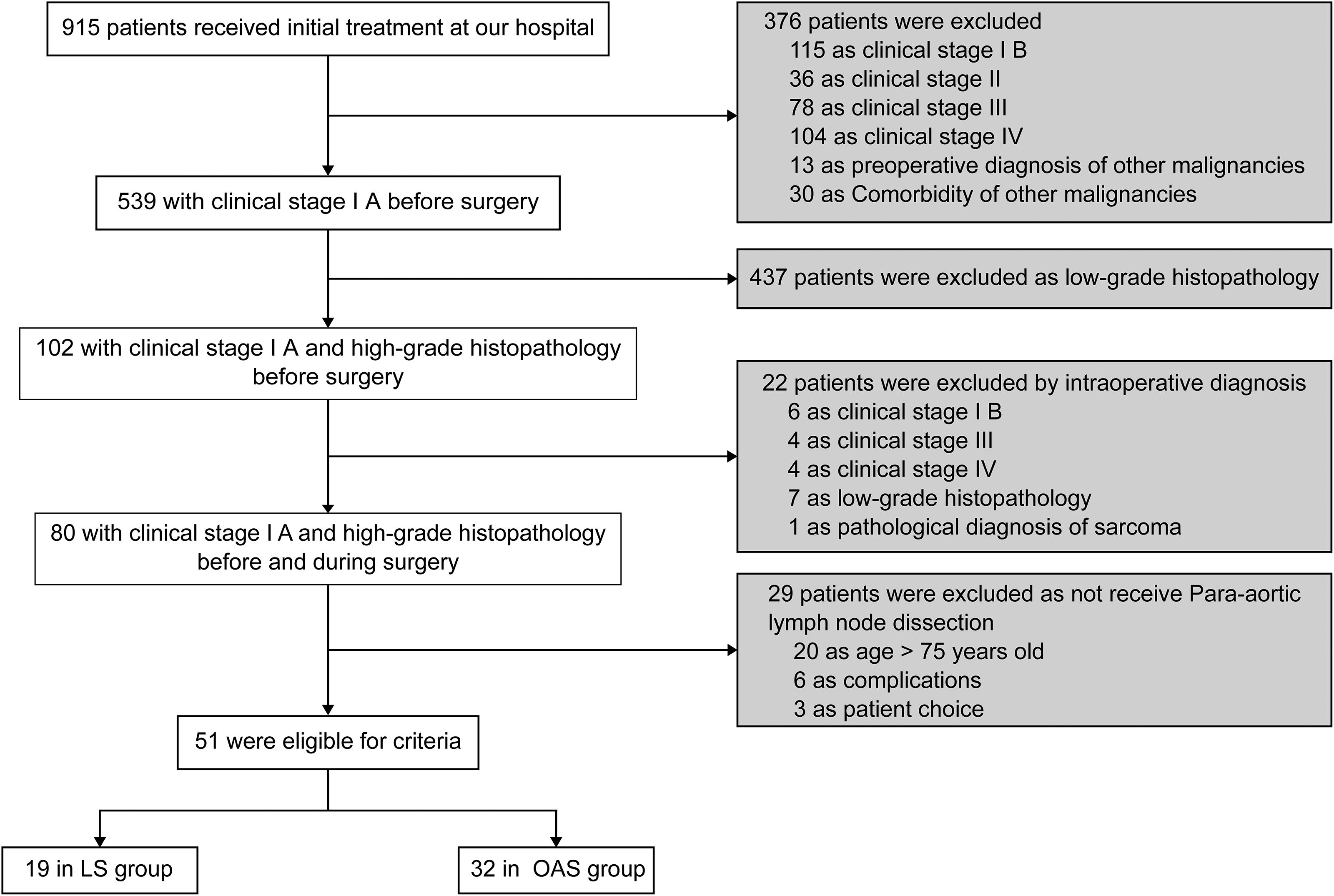
Recruitment flow diagram.
Patient Characteristics
Bold value indicate statistically significant differences (p < 0.05).
ASA-PS, American Society of Anesthesiologists Physical Status; ECOG, Eastern Cooperative Oncology Group; LS, laparoscopic surgery; OAS, open abdominal surgery.
Postoperative diagnosis and adjuvant therapy
In total, 15.8% (3/19) and 12.5% (4/32) of cases in the LS and OAS groups, respectively, were diagnosed as low grade in the postoperative pathological examination (Table 2). The postoperative stage was IA in 84.2% (16/19) and 81.3% (26/32) of patients in the LS and OAS groups, respectively. Lymph node metastasis was observed in 10.5% (2/19) and 6.3% (2/32) of patients in the LS and OAS groups, respectively. Overall, 84.2% (16/19) of patients in the LS group and 90.6% (29/32) of patients in the OAS group were classified as having medium- to high risk of recurrence (p = 0.66). A median of six cycles of platinum-based postoperative adjuvant chemotherapy was administered to eligible patients in both groups who consented. The median number of days from surgery to the first adjuvant chemotherapy session was 50 and 45 for the LS and OAS groups, respectively, with no significant difference (p = 0.19). In addition, the incidence of positive ascites cytology was significantly higher in the OAS group compared to the LS group (p < 0.05). This finding may reflect differences in tumor biology or intraoperative factors such as tumor manipulation and dissemination risk.
Postoperative Diagnosis and Adjuvant Chemotherapy
Bold value indicate statistically significant differences (p < 0.05).
LS, laparoscopic surgery; OAS, open abdominal surgery.
Surgical outcomes and complications
The median surgery time was significantly longer in the LS group at 471 minutes compared to 407 minutes in the OAS group (p < 0.05) (Table 3). The median blood loss was significantly lower in the LS group, at 100 mL, compared to 585 mL in the OAS group (p < 0.05), with four patients requiring transfusion in the OAS group and none in the LS group. A median of 47 pelvic lymph nodes were dissected in both groups (p = 0.84) (30 and 31 para-aortic lymph nodes in the LS and OAS groups, respectively; p = 0.83), with no significant differences. Intraoperative complications did not significantly vary between the two groups (p = 0.29), and no cases in the LS group required conversion to OAS. The longer operative time in the LS group may reflect the technical complexity of laparoscopic para-aortic lymphadenectomy and the surgical learning curve. However, the significantly lower blood loss in the LS group supports the minimally invasive benefits of the laparoscopic approach. Furthermore, the lower incidence of all-grade postoperative complications within 30 days in the LS group (p < 0.05) underscores its perioperative safety advantage.
Surgical Outcomes and Complications
Bold value indicate statistically significant differences (p < 0.05).
LS, laparoscopic surgery; OAS, open abdominal surgery.
Postoperative complications within 30 days were significantly more frequent in the OAS group (93.8%; 30/32 cases) than in the LS group (63.2%; 12/19 cases) for all grades (p < 0.05); however, no significant differences were observed when limited to grade 3 or higher complications (p = 0.52). For all-grade complications, there were more cases of leg and perineal edema in the LS group, while the OAS group had a higher incidence of elevated liver enzymes and ascites. Grade 3 or higher complications in the OAS group included one case of arytenoid cartilage dislocation and one case of appendicitis.
Postoperative complications beyond 30 days showed no significant differences between the two groups for all grades (p = 1.00) or for grade 3 or higher complications (p = 1.00). Grade 3 or higher surgical complications included one case of lymphedema in each group; both were treated with lymphaticovenular anastomosis. One case of chylous ascites was observed in the OAS group, which was managed with open abdominal drainage and lymphatic vessel ligation.
Prognosis
The 3-year RFS rate was 88.5% (95% CI: 61.4–97.0) and 90.2% (95% CI: 72.6–96.7) in the LS and OAS groups, respectively, with no significant differences (p = 0.36) (Fig. 2). Recurrences occurred in 15.7% (3/19) and 9.4% (3/32) of patients in the LS and OAS groups, respectively. Intra-abdominal recurrences were not observed in the LS group but were noted in two patients in the OAS group (Table 4). No recurrences occurred in the regional lymph nodes in the LS group; however, there was one patient with recurrence in the OAS group (Table 4). The 3-year OS rate was 94.4% (95% CI: 66.6–99.2) in the LS group and 93.4% (95% CI: 76.2–98.3) in the OAS group, with no significant difference (p = 0.99) (Fig. 2).
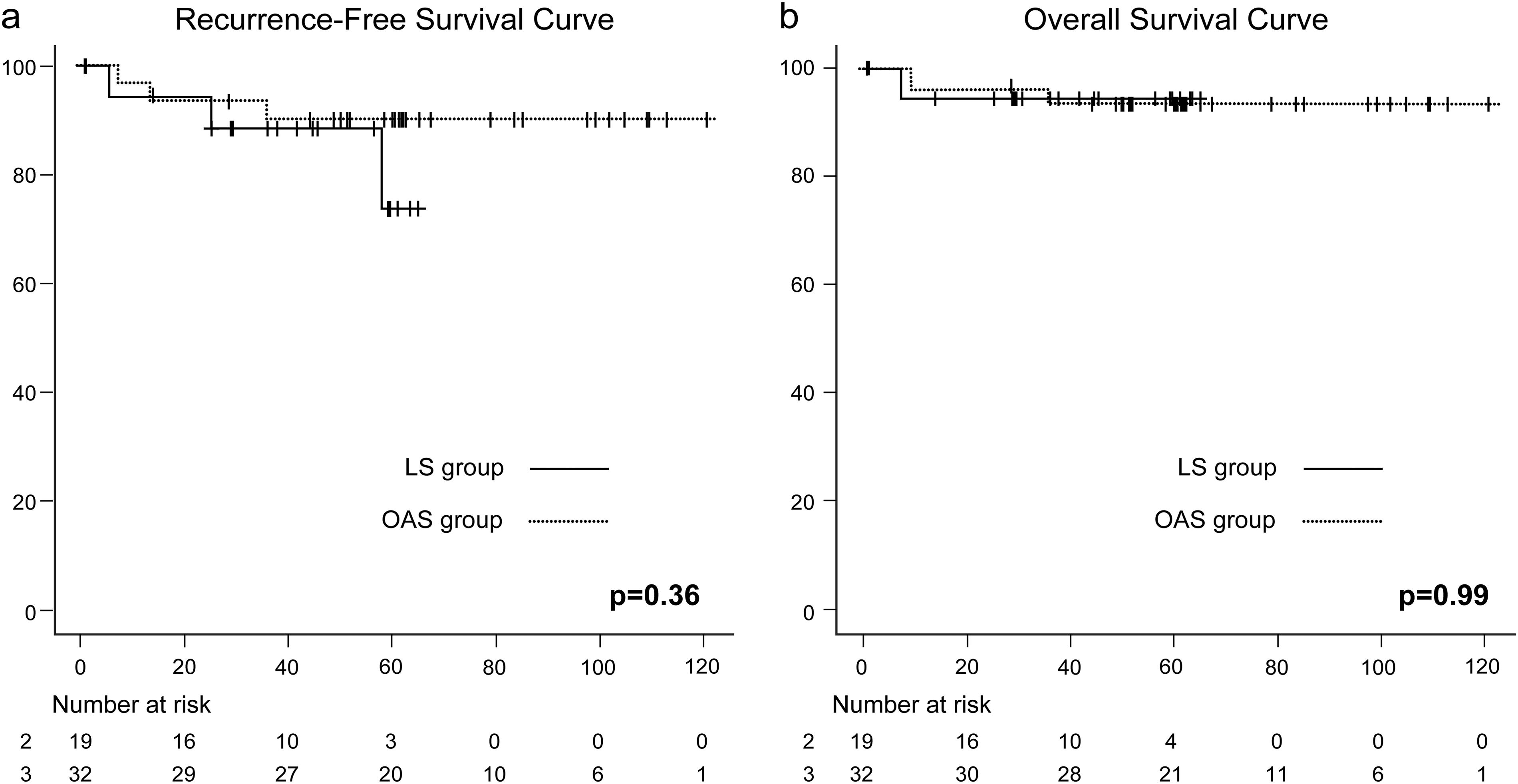
Overall and recurrence-free survival curves.
Recurrence Rates and Sites
LS, laparoscopic surgery; OAS, open abdominal surgery.
Discussion
This study compared the short-term prognosis of LS to OAS for patients with early-stage EC at high to intermediate recurrence risk (clinical stage IA, histological types other than endometrioid carcinoma G1/2) and revealed two key results. First, the findings suggest that the laparoscopic approach does not compromise short-term prognosis for patients with early-stage EC at high to intermediate recurrence risk treated with standard surgery (simple hysterectomy + bilateral salpingo-oophorectomy + omentectomy + pelvic lymphadenectomy + para-aortic lymphadenectomy). Second, postoperative complications were reduced with the laparoscopic approach. The lack of difference in short-term prognosis aligns with the findings of several retrospective studies suggesting that the laparoscopic approach for high- to intermediate-risk early-stage EC may yield a prognosis comparable to that of the open abdominal approach.15–17
A retrospective comparison of the prognoses of LS and OAS for patients with EC estimated to be stage I–II preoperatively but diagnosed with high-grade histological types postoperatively found no significant difference in prognosis between the two groups when postoperative stages were considered. 15 The proportion of patients with postoperative stage I–II was 72.1% in both groups. Similarly, a retrospective comparison of the prognoses of LS and OAS for patients estimated to be stage I–II preoperatively but diagnosed with high-grade histological types postoperatively found that the OAS group had a higher number of lymph nodes dissected and included more patients with advanced cancer postoperatively, while no significant prognostic differences were observed between the two groups. 16 Therefore, prognosis potentially does not differ for patients preoperatively estimated to be stage I–II, even if they are diagnosed with high-grade histological types postoperatively. However, these two studies analyzed patients diagnosed with high-grade histology postoperatively, rather than patients estimated to be high-grade histologically preoperatively and intraoperatively. In addition, the preoperative stages varied widely from stage I to II, resulting in variability in oncological backgrounds. In contrast, our study focused on patients who were estimated to be stage IA preoperatively and intraoperatively and diagnosed as high-grade histologically to ensure consistency in the oncological background.
All patients underwent para-aortic lymphadenectomy up to the level of the renal vein. However, the therapeutic significance of lymphadenectomy for EC remains debatable and inconclusive. In a large comparative trial of LS versus OAS for EC, Laparoscopy compared with laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group Study LAP2 (the LAP-2 study), the cephalad extent of para-aortic lymphadenectomy primarily reached the inferior mesenteric artery, which is narrower in scope compared to the lymphadenectomy performed up to the renal vein level by Tanaka et al. and in our study.3,4,18 Approximately 77% of positive para-aortic lymph nodes in ECs were located above the inferior mesenteric artery, and 46% had no metastasis below the inferior mesenteric artery. Therefore, several studies advocate for para-aortic lymphadenectomy up to the renal vein level.19,20 In addition, both OS and RFS outcomes in our study were more favorable compared with previous reports, which we attribute to our focus on early-stage cases. Thus, our results suggest that the laparoscopic approach does not compromise short-term oncological outcomes in cases where clinical stage IA EC is diagnosed preoperatively and intraoperatively with histological subtypes other than endometrioid carcinoma G1/2.
Our results indicate that LS reduces perioperative complications compared with OAS without increasing the risk of long-term surgical complications or delaying the initiation of adjuvant therapy. The absence of significant differences in intraoperative complications between the two groups is consistent with previous reports.21,22 Notably, no intraoperative complications or conversions to OAS were noted in the LS group at our facility. Furthermore, our finding of significantly fewer early postoperative complications in the LS group aligns with existing literature.21,22 Regarding specific all-grade complications, we observed higher incidences of elevated liver enzymes, ascites, and peritonitis in the OAS group, while perineal and lower leg edema were more common in the LS group. The increased incidence of elevated liver enzymes may be related to differences in postoperative management, such as the prolonged use of enoxaparin sodium for thromboprophylaxis; enoxaparin sodium is administered as subcutaneous injections from the day after surgery for 3–4 days in LS and for 6–7 days in OAS. Unfortunately, the precise reason for perineal and lower limb edema being more common in the LS group compared with the OAS group remains unclear, despite similar findings in both scenarios. In LS, the potential for improved access to broader and deeper surgical fields may allow for more aggressive lymph node dissection, possibly extending to more distal lymph nodes. 23 In addition, clearance of superior inguinal nodes, which are rich in lymphatic vessels, could potentially increase the risk of leg lymphedema symptoms postoperatively due to the possibility of lower limb lymphatic obstruction. 24 However, in our practice, regardless of the surgical approach, we perform skeletonization of the external iliac vessels and clear the external superior inguinal lymph nodes, which are regional, when performing pelvic lymph node dissection. We also use clips for ligation during LS. Thus, not only the surgical approach but also differences in surgical techniques may have influenced the frequency of perineal and lower limb edema.
Nevertheless, we observed no significant difference in postoperative complications after 30 days. In addition, we observed no significant difference between the two groups in the time from surgery to the initiation of adjuvant therapy, with most patients in both groups commencing treatment within 8 weeks. Thus, our results indicate that LS reduces early postoperative complications compared with other approaches; however, complications after this period occur at a consistent frequency regardless of the surgical approach. In both groups, lymphedema was a frequent complication after 30 days, with one case in each group requiring lymphaticovenular anastomosis due to grade 3 complications. To mitigate these complications, future research should focus not only on surgical approaches but also on differences in surgical techniques and perioperative management strategies.
This study has some limitations, which should be considered when interpreting the results. First, because this was a retrospective study at a single regional cancer center, selection bias cannot be excluded. Second, this study was exploratory, with a small sample size. Third, the observation period for the LS group was significantly shorter than that of the OAS group. This is due to the later adoption of laparoscopic surgery at our institution in 2018, resulting in inherently shorter follow-up periods for the LS group. While both groups had three cases of recurrence, each group also had one case of recurrence occurring more than 60 months post-surgery. Therefore, a longer observation period is necessary to compare long-term outcomes. In addition, a multicenter prospective trial is necessary to validate the significance of LS for early-stage EC with a high risk of recurrence (clinical stage IA, histological type other than endometrioid grade 1/2).
Conclusions
The short-term outcomes associated with total hysterectomy, bilateral salpingo-oophorectomy, omentectomy, pelvic lymph node dissection, and para-aortic lymphadenectomy for early-stage EC (stage IA, histological type other than endometrioid grade 1/2) showed no significant difference between LS and OAS approaches.
Footnotes
Authors’ Contributions
R.N.: Conceptualization, methodology, resources, data curation, formal analysis, writing—original draft preparation. N.T.: Conceptualization, methodology, writing—reviewing and editing. M.I.: Resources. M.S.: Resources. C.E.: Resources. S.M.: Resources. N.K.: Resources. A.K.: Methodology, writing—reviewing and editing. A.F.: Methodology, writing—reviewing and editing. N.K.: Methodology, writing—reviewing and editing. A.M.: Methodology, writing—reviewing and editing. M.T.: Supervision. Y.H.: Supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.