
Abstract
Background:
Cervical fibroid, due to its location and the vital structures present in the close vicinity, poses a surgical challenge during hysterectomy.
Case:
We report four cases of cervical fibroid managed by surgery. In one of them, ureters were dissected and lateralized from the uterus. Whereas, in the other case, enucleation of a fibroid was done before proceeding with the hysterectomy. The other two cases were managed with polypectomy.
Conclusion:
Good anatomical knowledge and clinical judgment are essential for successful surgical management of cervical fibroids.
Background
Fibroid is also called a leiomyoma. It is a benign tumor composed mostly of muscle tissue that commonly arises from the uterus. Rarely, it may arise from the cervix. Cervical fibroids may protrude anteriorly or posteriorly leading to pressure over urinary bladder or rectum and causing urinary or defecatory symptoms. It can prolapse through the cervix into the vaginal canal. Surgery remains the preferred treatment, myomectomy or hysterectomy based on the case scenario.
Technique
The cervix is an unusual location for the fibroid. It may be central in location anteriorly, posteriorly or on one of the sides or pedunculated into the vagina. It may distort the anatomy of the ureters and uterine artery. In the case of a pedunculated fibroid polyp with a stalk, arising from the ectocervix, simple polypectomy by cutting the stalk is enough. Whereas in the case where the stalk is arising from the endocervix, the anterior lip of the cervix may be cut to reach the stalk. In the case of hysterectomy for the cervical fibroids, the modification of routine steps is important. In a central cervical fibroid, the enucleation followed by hysterectomy may suffice. But if the fibroid is on one of the sides of the uterus, dissection of the ureters to lateralize them from the uterus is also important to prevent the injury. Staying inside the capsule of the fibroid is the key to prevent uteteric injury.
Case presentation
Case 1: A 34-year-old female, para 3, presented with a complaint of lump in the abdomen associated with pain and no menstrual complaints. Clinical examination revealed a firm, non-tender, abdominopelvic mass corresponding to a 30 week uterus. On bimanual examination, cervical lips were effaced and the mass was felt continuous with the cervix, the uterus could not be felt separately from the mass, and it could be felt through all fornices. Ultrasonography revealed a 22 × 18 × 12 cm large, lobulated, exophytic, predominantly hypoechoic lesion occupying the cervix. After preoperative evaluation, laparotomy was done by a median incision; large 20 × 20 cm cervical fibroid was present with the uterus elevated on top of it (Fig. 1). Bilateral ureters were running at the base of the fibroid laterally, which were identified. The fibroid was enucleated, and the ureters were well lateralized from the lower uterine segment. Hysterectomy was proceeded. Postoperative recovery was uneventful.
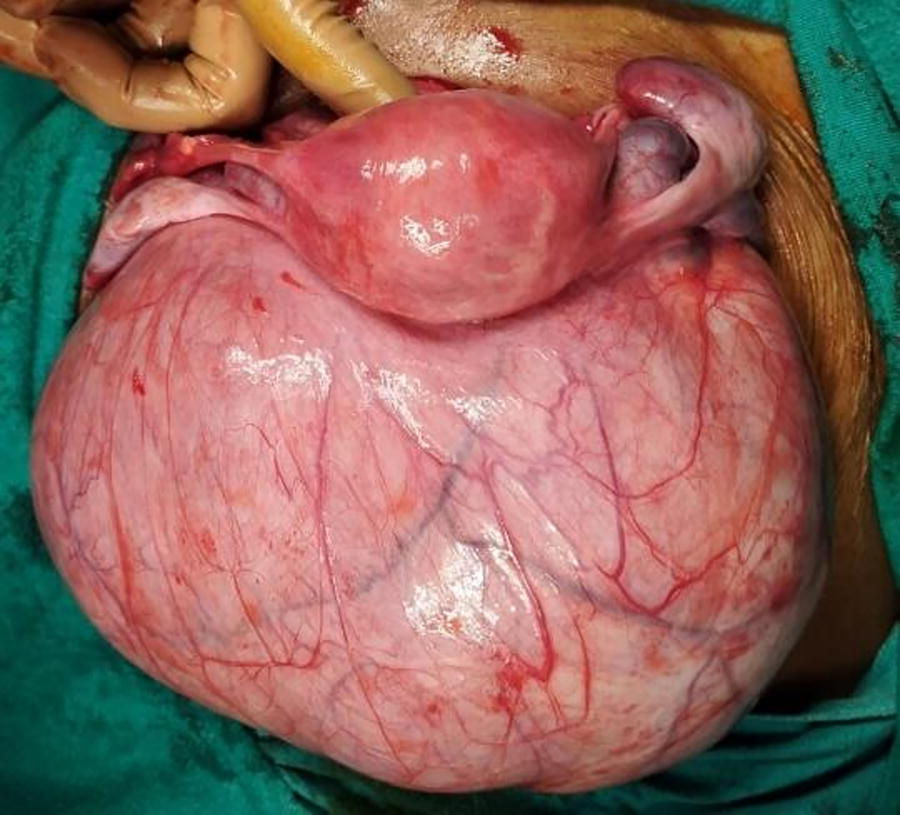
Intraoperative image showing large posterior cervical fibroid.
Case 2: 37 years lady, P2L2, presented with severe dysmenorrhea. On examination, the uterus was corresponding to 16 weeks in size with a bosselated surface. Ultrasound suggested multiple uterine fibroids, with largest fibroid located in the cervical region. An endometrial biopsy was done, which suggested secretory endometrium. Surgery was planned. Intraoperatively, 9 × 6 cm central cervical fibroid was present with the uterus and other multiple fibroids elevated on top of it giving it, an appearance like the Lantern on St. Paul's Cathedral. A longitudinal incision was made over the myoma, and enucleation was done, but due to excessive bleeding, she required a hysterectomy.
Case 3: 36 years lady, P2L2, presented with something coming out of the vagina and foul-smelling vaginal discharge. On examination, a large, firm, solid, necrotic mass was present arising from the anterior lip of the cervix and extending outside the vagina with surface necrosis (Fig. 2). Differential diagnosis of cervical fibroid polyp with surface necrosis, incarcerated procidentia, and chronic uterine inversion was kept. Ultrasound examination findings showed a sizable fibroid polyp (20 × 15 × 10 cm) arising from the anterior lip of the cervix with uterocervical descent. Vaginal myomectomy was performed. The postoperative recovery period was uneventful, and the uterocervical descent was relieved on follow-up examination after 15 days of the surgery.

Large incarcerated cervical fibroid polyp with surface necrosis.
Case 4: 38 years, P1L1 with cervical fibroid polyp of 6 × 5 cm with small stalk arising from the posterior endocervix. The anterior lip of the cervix was cut to reach the stalk, and cervical myomectomy was done. The postoperative period was uneventful.
Discussion
Uterine fibroids are the most common benign smooth muscle tumors of the female genital tract.1–3 Fibroids can be intramural, submucous, or subserous, mostly arising from the body of the uterus. Due to the paucity of smooth muscles in the cervical stroma, cervical fibroids are rare, with an incidence of 1%–2%. 1 Cervical fibroid may present with complaints of abnormal uterine bleeding, chronic pelvic pain, dysmenorrhea, constipation or frequent micturition, dyspareunia, lower abdominal pain, tenesmus, pregnancy loss, and some cases of infertility.4,5 The cervical fibroid can disturb the anatomy of the ureters, bladder, and uterine arteries, making them more prone to injury and hemorrhage, proving to be a challenge to the surgeon. 6 Thus, steps of standard hysterectomy technique are not appropriate for the cervical fibroid. 7 A cervical fibroid may present as a variable-sized polyp; the larger one can mimic incarcerated procidentia or chronic uterine inversion or can cause uterocervical descent due to traction. 8 Ultrasonography is a commonly used method to differentiate fibroids from other pelvic pathologies, as it is cost-effective and easily available. It also gives information on the location, size, and International Federation of Gynaecology and Obstetrics (FIGO) type of the fibroid. 2 Magnetic resonance imaging should be done in case of doubt, as it can help in evaluating the adjacent structures such as the ureter, bladder, rectum, and endometrial cavity. Intravenous pyelography can further demarcate the course of the ureters.9,10
All of our cases of cervical fibroid were managed surgically. In one of them with posterior wall fibroid, ureters were well lateralized by dissection, while in another case with central cervical fibroid, enucleation was done before hysterectomy was proceeded. The other two cases were managed with polypectomy. In conclusion, due to the atypical location of the cervical fibroid, standard hysterectomy procedures may need to be modified. Enucleation of the fibroid or ureteric dissection should be performed prior to proceeding with the hysterectomy. A thorough understanding of pelvic anatomy and sound clinical judgment are crucial for successful surgical management.
Footnotes
Authors’ Contributions
A.S. and M.D. managed the cases and collected relevant data (data curation, formal analysis, investigation). A.S. drafted the article with direction from M.D. (conceptualisation, methodology, resources, supervision, project administration, software, writing). A.S. and M.D. critically evaluated the article (writing—review and editing). Both the authors approved the final version of the article (validation and visualization).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Consent from the Patient
Taken, to submit her de-identified images.