
Abstract
Background:
The increasing adoption of robotic-assisted surgery (RAS) platforms in minimally invasive gynecological surgery (MIGS) has exposed limitations in structured fellowship training. This study aims to discuss the advantages of dual-console training within robotic MIGS programs.
Methods:
We propose a training module for robot-assisted surgery for benign gynecological surgeries. The training includes formal online and hands-on training, simulation exercises, assistant practice, and dual-console operations, personalized according to the trainee's level of experience with the guidance of an experienced surgeon. The primary outcome of this article is to promote a dual-console training module for junior surgeons and to explain its advantage in the development of robotic surgical skills.
Results:
This approach enhances precision and efficiency while maintaining patient safety and avoiding increased surgical times or complications. Personalized mentoring allows for direct movement correction, exploration of anatomy, skill augmentation, and optimized application of various surgical instruments, leading to an improved and customized learning experience that sharpens performance.
Conclusions:
The incorporation of dual-console training in robotic surgery enhances the learning experience for MIGS trainees. This training approach should be considered for integration into MIGS fellowship training programs in Australia to prepare surgeons for the increasing prevalence of RAS.
Introduction
Robotic-assisted surgery (RAS) has become increasingly popular.1,2 Marking a transition from traditional open to laparoscopic procedures in gynecology.3,4 RAS addresses the limitations of laparoscopy by offering three-dimensional vision, greater magnification, tremor filtering, superior instrument mobility, and enhanced ergonomic design.5,6 These features have improved precision and efficiency in complex procedures. 7
Laparoscopic skills remain essential in minimally invasive gynecology training. Nevertheless, the increasing acceptance of RAS has necessitated its inclusion in such programs. Evidence shows more than 50% of first-year fellows are already familiar with robotic technologies and have experience in robotic bedside assisting. 8 Training programs can contribute to an enhanced learning curve leading to increased efficiency and cost savings, however, only a few exist. 9 In Australia, despite the growing integration of RAS into the health care system, structured training remains limited, with no national guidelines or standardized curricula currently in place for gynaecologic fellowship programs. This can result in variable training quality potentially affecting surgeon competency and patient outcomes. Information from the Netherlands concerning their training journey for robotic surgery across all disciplines exhibited inconsistency and included training conducted by Intuitive SurgicalTM, master-apprenticeship, fellowships, and self-designed programs. Their conclusion was that to ensure high-quality training for fellows, it is imperative to formulate and implement clear training goals. 10 Similarly, the Fundamentals of Robotic Surgery (FRS) curriculum, a multi-specialty, proficiency-based training framework validated in trials across 12 American institutes, aims to address such inconsistencies, though its adoption remains globally uneven. 11 Data on minimally invasive gynecology surgery (MIGS) programs indicate a trend towards integrating online courses with dry lab exercises and simulation programs including virtual reality simulators. 12 Further data on robotic trainers demonstrate their importance in the capacity to enhance speed and consistency while preserving precision across multiple repetitions. 13
The evolution of the dual console has been driven by the need for expanded training options. A study investigating the benefits of the dual console during a fellowship program in MIGS revealed that the dual console allows greater “hands-on” experience with extended console time, fostering increased interaction with the attending surgeon. 14 Dual-console training addresses these training gaps by providing personalized, hands-on experience under direct supervision, effectively bridging the transition from simulation to live surgery while maintaining patient safety. A recent review examining the status of training for the robotic surgical trainee proposed a range of methods including training curricula for the trainee and post trainee,11,15 robotic simulators,16,17 and dual consoles, 18 platforms. The data, however, is ambiguous, and a further understanding of how to create an effective training experience for gynecologic surgical trainees and robotics teams is needed. 19
In this study, we highlight the advantages of the dual console within our training program for robotic MIGS, under the guidance of highly skilled and experienced robotic surgeons.
Material and Methods
Dual-console surgery for trainees in their 5–6th year of training occurred for cases of hysterectomy, ovarian cystectomy, myomectomy, and excision of stage IV endometriosis.
The Sydney Women's Endosurgery Centre training program: (Fig. 1)
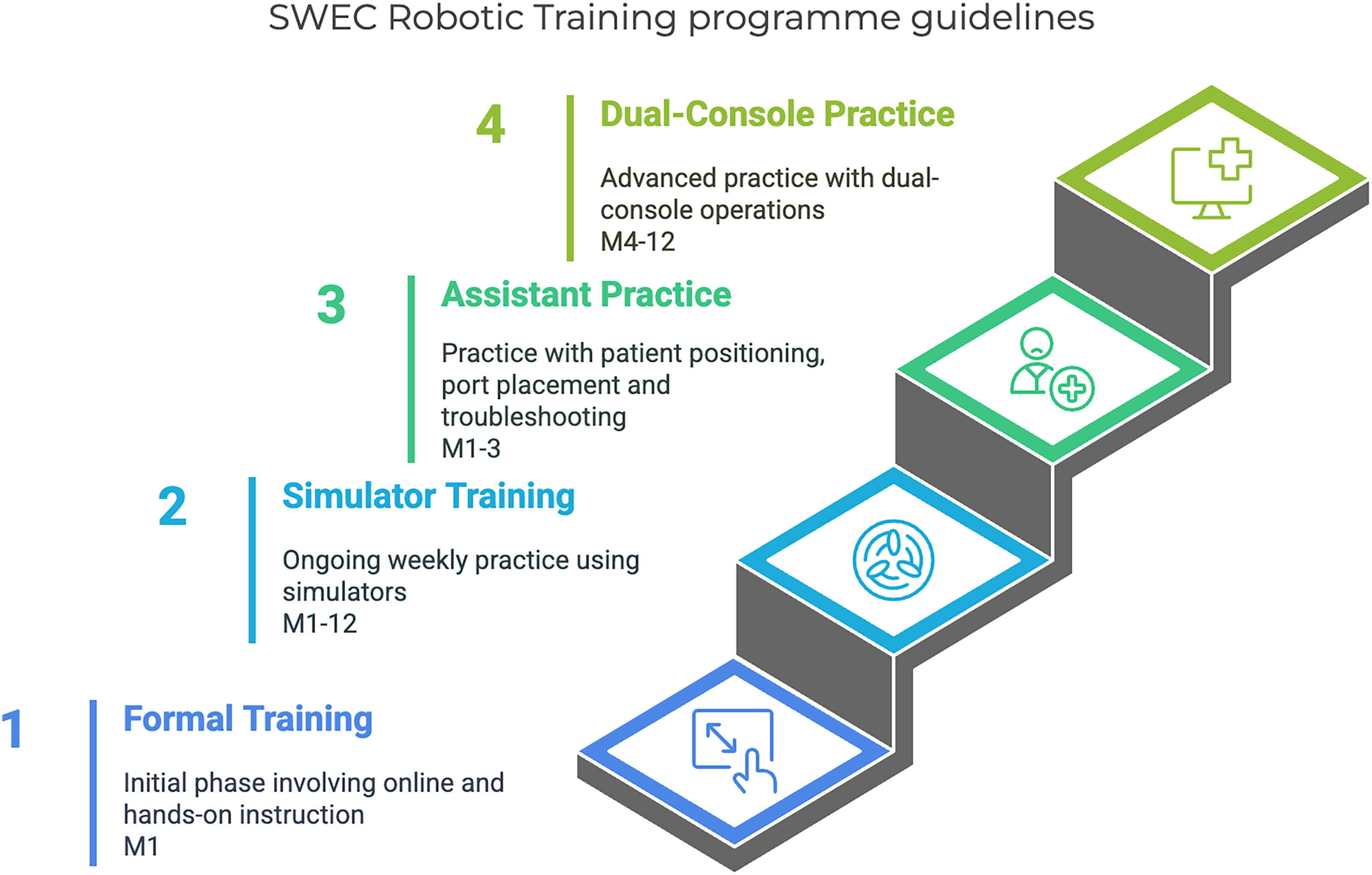
SWEC robotic training program guidelines. Month 1: Formal training (10 hours total). Online module (5 hours), hands-on instruction (5 hours); months 1–3: Assistant practice (in average 5 cases/week). Patient positioning, port placement, docking, troubleshooting, supervisor assessment: docking <10 minutes, error-free troubleshooting; months 4–12: A dual-console practice (One case/week). Start with 1 arm → Progress to 2–3 arms + scope. Months 1–12 (Ongoing): Simulator training (1–2 hours weekly) runs across all 12 months. SWEC, Sydney Women's Endosurgery Centre.
Formal training including online and hands-on instruction.
Simulator training.
Assistant practice: Patient positioning, port placement, docking, surgical skills, anatomy knowledge, and system troubleshooting.
Dual-console practice.
Initial training focuses on patient positioning, port placement, docking, and assisting techniques across a broad range of surgical procedures, as well as troubleshooting. Subsequently, trainees progress to simulator and dry lab applications. Advanced methods involve the use of a dual console, providing greater opportunities for a gradual hands-on experience. The trainee can control one or more robotic arms, the scope, or no arms based on their learning curve and experience.
Competency was assessed informally through direct observation by the supervising surgeon, focusing on docking efficiency, surgical precision, and troubleshooting skills.
This study describes an educational method implemented at our institution. It did not involve the collection of personal data or interventions requiring ethical approval.
Results
During the initial months of training, each trainee was required to follow the aforementioned steps. Each underwent formal training encompassing online and hands-on instruction before commencing their first live patient training. Next phase consists of assistant practice for hysterectomy, myomectomy, endometriosis surgery, sacrocolpopexy, and cystectomy. This step includes port positioning, port placement, docking, assisting, and troubleshooting
Port positioning:
Routine port positioning for minimally invasive robotic surgery, such as hysterectomy and sacrocolpopexy, for a normal-sized uterus. Supra-umbilical port positioning for cases with an enlarged uterus. Low port positioning for endometriosis cases. The docking routine included achieving precise Trendelenburg positioning for the small bowel to be at the level of the pelvic brim and robot positioning. Presenting instruments in the right position in the abdomen, and arm adjustments for optimal distance. In order to minimize the time between the onset of anesthesia and the commencement of surgery, the focus is placed on the efficiency and precision of docking procedures by the surgical team. Assisting in each case was focussed on the specific surgery. Troubleshooting covered issues such as arm clashes, tower alerts, and alerts from other room instruments.
Following step: Practical exercises using the dual console, with the trainee operating with one, two, or three arms, with or without the scope, based on their level of experience. Gradual increase in primary surgical experience in smaller procedures, such as salpingectomy, or focus on the mastery of specific instruments, such as the vessel sealer.
This hands-on experience allows the fellow to refine precise surgical techniques and optimize tool utilization, including an introduction to writing techniques, as a new concept. The fellow is also actively involved in suturing during myomectomy. Exposure to these varied scenarios contributes to the development of precision, accuracy, and enhanced performance, particularly when the goal is to operate with three arms and a scope.
Throughout this period, each trainee dedicated time to training on the simulator under the guidance of the specialist team (Fig. 1).
The close interaction with the leading surgeon encourages personalized learning, resulting in a unique and targeted learning curve while prioritizing patient safety and maintaining the flow of the surgery. In our cases, despite the inclusion of additional training elements, surgical time remains unchanged, and no complications have been observed.
Due to the descriptive and pilot nature of this study, formal quantitative or qualitative data on trainee competency, patient outcomes, or surgical efficiency were not collected. However, informal feedback from trainees and supervisors indicated that the primary benefit of the dual-console approach was in control of the instruments, understanding their movement range within the pelvis, and learning the correct use and access for each surgery, which enhanced their procedural confidence and adaptability.
Discussion
Robotic-assisted surgery is playing an increasing role in the Australian health system. 20 Despite the high volume of laparoscopic surgeries in Australia and the demand for laparoscopic training, the rise in robotic surgeries calls for training in the robotic field as well. 21 This issue concerns many specialists who are responsible for the training programs and surgical progress of the upcoming Minimally Invasive Gynaecologic Surgeons in Australia and overseas. We addressed this issue during our fellowship program in response to changes in the prevalence of RAS and the integration of robotic systems into the public health care system as others in the United States and Europe. 22 In this article, we suggest the key steps a trainee should take to prepare for becoming a robotic surgeon and consider the dual console as part of the learning process.
Preoperative training
Formal Intuitive training includes online training, hands-on instruction, as well as formal simulator training. The idea of ‘practicing’ on the patient should be timed appropriately and minimized as much as possible. There are only a few curricula in the United States and more recently the Society of European Robotic Gynecological Surgery considers this as the first important stage in the training process.15,23 Formal validation has yet to be conducted, and no Australian guidelines are currently known. However, validation for the effectiveness of the FRS skills curriculum, which includes simulation, has been demonstrated to be a valuable component in the training process. 11 Furthermore, it has been previously established, through machine learning and real-time video feedback, that simulator modalities can be employed to teach and evaluate robotic surgical skills, demonstrating positive effects on robotic skills proficiency. 19
Assistant training
Watch and learn: Aspiring to become the best surgeon is a common goal for surgical professionals. Striving for excellence involves observing and learning from accomplished surgeons. This includes watching videos and live surgeries of experienced mentors. 24 Interestingly, even mentors themselves review their own videos to enhance their performance and skills. 25 While assisting, you can achieve several crucial components. Acquiring knowledge of anatomy and surgical procedures is facilitated through active observation. A deeper understanding of robotic operations evolves over time by actively engaging in questioning with the mentor. Furthermore, actively participating in tasks such as docking, port positioning and placement, and troubleshooting in collaboration with the mentor enhances the learning experience, contributing to a comprehensive understanding of the role of a robotic surgeon.
Dual console
Some data are already available regarding the importance and benefits of the dual console. This mode of learning allows the MIGS fellows more time on the console compared to a single console, allowing the accomplishment of more steps by the trainee. The real-time feedback during surgical cases is an enormous benefit, all without a significant change in the total case time or complication rate. 14 Another study has shown that the use of the dual console led to improvement between cases, with a proven lower level of stress and frustration during surgical procedures. 26 Based on our experience and on previous studies the dual console offers benefits in robotic surgery training. It facilitates a customized learning curve, allowing trainees to progress at their own pace. With a balanced learning curve, trainees can gradually take on more tasks, avoiding an all-or-none approach. The dual console provides the opportunity to gain expertise in different concepts at different times, allowing for a comprehensive understanding. Trainees can integrate their training over time, culminating in live observations ensuring a well-rounded and effective learning experience. As a descriptive pilot study, we did not statistically compare the data on surgical time and complications however this observation is supported by existing literature on dual-console training. 18 Key barriers include the high initial cost of dual-console systems, which can be prohibitive for public hospitals, and limited access to equipment due to scheduling constraints and availability in training centers. In addition, the need for experienced surgeons to supervise dual-console sessions may strain existing resources. To overcome these, we propose strategies such as partnering with industry stakeholders (e.g., Intuitive Surgical) for equipment loans and developing a training cascade model where experienced fellows train new trainees, reducing the reliance on senior surgeons.
Challenges encountered during the implementation of dual-console training included coordination difficulties between the trainee and supervising surgeon due to unfamiliarity with simultaneous control and scheduling conflicts with equipment availability. These were addressed through pre-surgical briefings to align roles and responsibilities and by prioritizing dual-console sessions during off-peak operating times to ensure access to the robotic system.
Conclusions
This training concept, especially valuable in the absence of a recognized national program, can be considered an integral part of minimally invasive fellowship training programs and hopefully serve as a basis for future robotic programs. Formal validation of the curriculum using standardized assessment tools to objectively evaluate trainee competency should be conducted. In addition, comparative studies assessing dual-console versus single-console training, measuring outcomes such as operative time, complication rates, and trainee skill acquisition are needed to provide robust evidence of the dual-console approach's superiority or equivalence.
Footnotes
Authors’ Contributions
Y.Y.: Conceptualization, data curation, writing—original draft. M.A. and O.D.: Investigation methodology project, writing—review and editing. J.R. and S.C.: Writing—review and editing. D.R.: Writing—review and final draft editing. D.C.: Conceptualization, writing—review and editing.
Author Disclosure Statement
All authors declare no conflict of interest.
Funding Information
No funding was received for this article.