
Abstract
Background:
Hysterectomy is one of the most commonly performed gynecological procedures worldwide. Vaginal Natural Orifice Transluminal Endoscopic Surgery (vNOTES) is an innovative approach that combines the precision and enhanced visualization of endoscopic surgery with the well-established advantages of the vaginal route. The vNOTES hysterectomy procedure is performed in three distinct phases, with the initial and final phases completed vaginally. Insufficient uterine prolapse often presents a challenge during the vaginal phase, leading surgeons to opt for non-vaginal surgical approaches.
Methods:
This article revisits the uterosacral ligament massage technique, described in older gynecological literature, which involves stretching the uterosacral–cardinal ligament complex under steady cervical traction to improve uterine descent.
Results:
A step by step description, supported by figures and video, illustrates the uterosacral ligament massage technique and its application during the vNOTES procedure.
Conclusion:
Incorporating uterosacral ligament massage into vNOTES protocols could improve uterine mobility and enhance accessibility during the vaginal phase. This simple yet effective technique has the potential to expand the indications for vNOTES, making it a viable and accessible option for a broader range of patients, including those with limited uterine descent.
Background
Hysterectomy is one of the most frequently performed gynecological procedures worldwide. 1 Among the various surgical approaches, the vaginal route is preferred for benign indications due to its well-established advantages, including shorter recovery time, reduced postoperative morbidity, shorter operative durations, and decreased hospital stays compared with conventional laparoscopy or laparotomy. 2 Despite these benefits, the vaginal route remains underutilized, with surgeons often favoring alternative methods. 3 This is largely attributed to challenges inherent to vaginal hysterectomy, such as limited visibility and access, as well as inadequate surgical training.
The introduction of Vaginal Natural Orifice Transluminal Endoscopic Surgery (vNOTES) represents a transformative development in minimally invasive gynecological surgery. This innovative technique combines the precision and enhanced visualization of endoscopic surgery with the well-established advantages of the vaginal approach. 4 By addressing many of the limitations traditionally associated with vaginal hysterectomy, including restricted visibility and challenging access, vNOTES has the potential to expand the indications for vaginal surgery.
The vNOTES hysterectomy procedure is performed in three distinct phases, with both the initial and final phases completed vaginally. 5 The initial phase involves circumferential incision of the cervix, anterior and posterior colpotomies, and transection of the uterosacral ligaments. 5 These steps closely resemble those in traditional vaginal hysterectomy, and the vaginal route is particularly advantageous when conditions such as adequate uterine mobility, descent, and access are present. 6 Insufficient uterine prolapse presents a challenge during the vaginal phase, and is often encountered in patients with nulliparity or prior cesarean deliveries.
The uterosacral ligaments are integral to the structural support of pelvic organs. 7 In 1972, Cohen introduced the technique of uterosacral—cardinal ligament complex stretching, commonly referred to as “uterosacral massage,” to improve uterine descent and facilitate vaginal hysterectomy. 8 The efficacy of uterosacral-cardinal ligament stretching was validated in a 2012 prospective study, which demonstrated significant improvements in uterine and anterior vaginal wall descent among women undergoing vaginal hysterectomy. The study specifically included patients with preexisting uterine prolapse and a uterus not exceeding 12 weeks in size. 9
This paper aims to revisit the uterosacral massage technique, an approach described in older gynecological literature, and to advocate for its use in modern practice. By integrating this technique into their repertoire, surgeons may gain greater confidence in selecting vNOTES, even for patients with a non-prolapsed uterus.
Technique: Uterosacral Ligament Massage Prior to vNOTES
After the initiation of general anesthesia, the patient is positioned in the dorsal lithotomy position with her legs abducted and hips flexed at 90°, supported in boot stirrups. The buttocks are positioned at the edge of the table. 5 The perineal area is disinfected and draped. The abdomen is also prepared in case of the need for conversion to abdominal access. A Foley catheter is inserted for bladder drainage. 5
The uterine cervix is grasped with a tenaculum forceps and pulled with a constant, steady force. If a standardized metal coil force detector is available, ensure a pulling force of 0.5 kg (500 N) (Fig. 1).
The cervix is grasped and pulled with a tenaculum forceps.
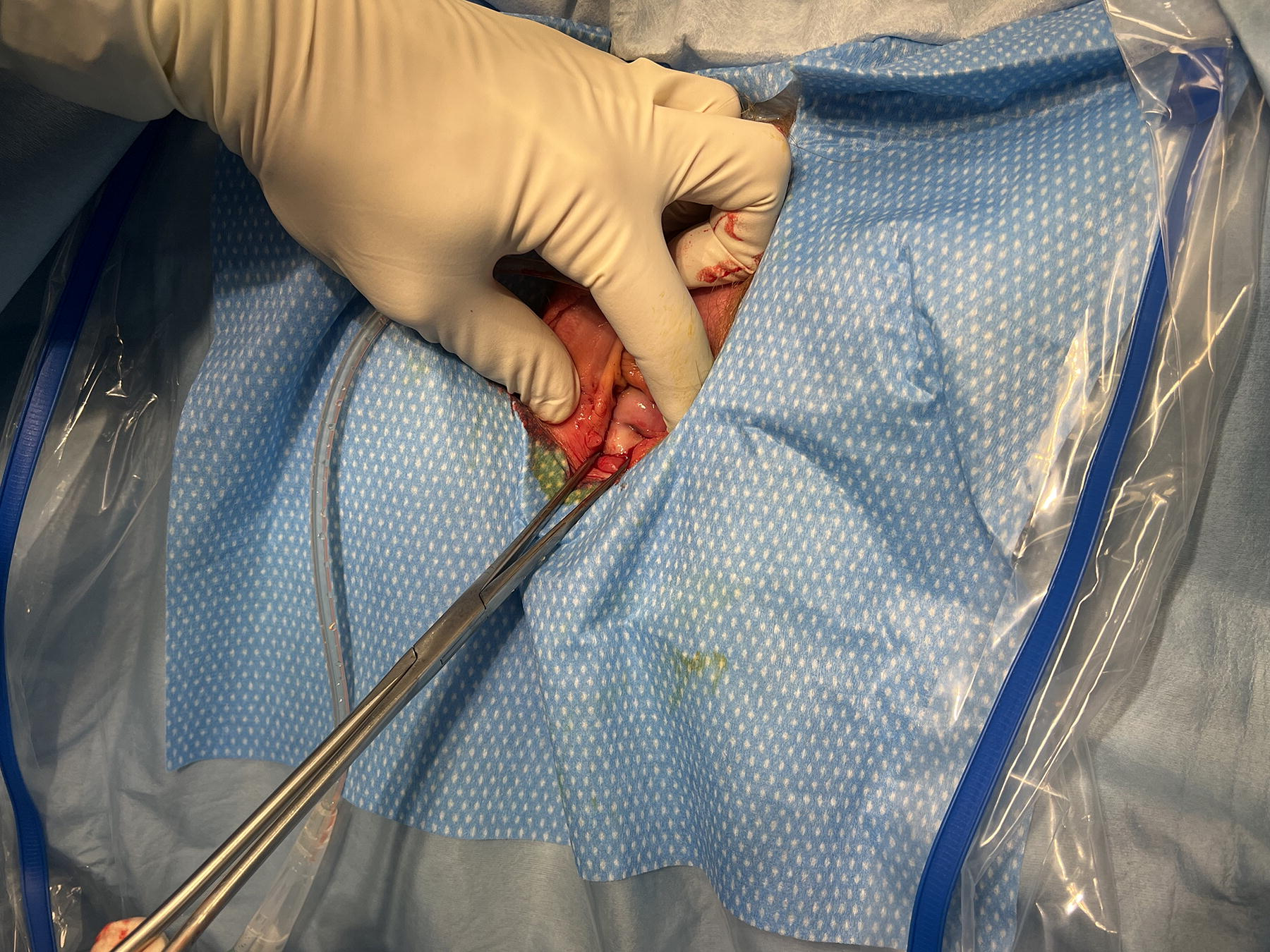
The surgeon then places their index finger on the paracervical tissue, lateral to the uterine cervix, and performs a massaging motion from front to back along the uterosacral–cardinal ligament complex on each side (Fig. 2).

The uterosacral–cardinal ligament complex is massaged on each side.
Five repeated stretching movements on each side are performed to effectively stretch the uterosacral ligament complex. The process should take approximately one to three minutes to complete while keeping constant, steady pressure on the cervix. A video demonstrating the technique, including pre- and post-massage measurements, is provided.
Discussion
Decision-making regarding the route of hysterectomy is typically guided by clinical algorithms that consider factors such as vaginal access, uterine descent, and uterine size. 10 Current modified clinical decision algorithms primarily focus on four surgical approaches: vaginal, abdominal, laparoscopic, or robotic. The initial step in these algorithms often involves assessing whether vaginal access is sufficient. 10 If vaginal access is deemed inadequate, patients are redirected toward abdominal, laparoscopic, or robotic methods. A lack of sufficient uterine descent remains a significant barrier, frequently leading to the selection of non-vaginal surgical methods.
However, these existing algorithms do not yet incorporate vNOTES as a surgical option. By addressing limitations such as restricted visibility and access, vNOTES has significantly expanded the scope of vaginal surgery. This approach has the potential to enable more patients to undergo minimally invasive surgery, even in cases of non-prolapsed uteri. However, the lack of sufficient uterine descent remains a technical challenge that can complicate the initial vaginal phase of vNOTES. The technique of uterosacral ligament massage, as described, offers a potential solution to overcome this barrier. As demonstrated by the 2012 prospective study by Krissi H et al., uterine traction combined with uterosacral–cardinal ligament complex stretching significantly increased the distance of the lowest edge of the cervix (Point C on the pelvic organ prolapse quantification scoring system) from 2.7 ± 2.2 cm to 4.6 ± 2.1 cm (p < 0.001). 9 By improving uterine descent, it facilitates the vaginal phase of the procedure, particularly in patients with non-prolapsed uteri. This simple yet effective technique, rooted in the principles of vaginal hysterectomy, has the potential to be seamlessly integrated into vNOTES procedures.
Non-descent of the uterus has been identified as one of the primary reasons for conversion from vaginal surgery to laparotomy in a study of 1,736 vaginal hysterectomies performed at a single center. 11 Incorporating uterosacral ligament massage into the intraoperative protocol for vNOTES could help reduce conversion rates to alternative surgical approaches by improving uterine accessibility. The authors routinely perform this procedure in patients with minimal uterine descent, as it facilitates the anterior and posterior colpotomies to be performed with greater ease.
While the benefits of uterosacral ligament massage have been demonstrated in facilitating traditional vaginal hysterectomy for prolapsed uteri, its application on non-prolapsed uteri remains underexplored. 9 Future studies should evaluate the clinical application of uterosacral ligament massage in improving surgical outcomes, including its impact on operative time, surgical complications, and the conversion of vNOTES to alternative surgical routes.
Conclusion
Revisiting this age-old technique provides surgeons with an opportunity to confidently select the vaginal route, even for patients traditionally considered less favorable candidates for vaginal surgery. The incorporation of uterosacral ligament massage could refine and expand the indications for vNOTES, making it a more accessible option for patients who might otherwise be excluded due to anatomical limitations.
Footnotes
Authors’ Contributions
J.B. and C.Y.Y.H.: Conception and design of study, drafting of article and critical revision, approval of final article.
Author Disclosure Statement
J.B. discloses consultancy for Applied Medical. C.Y.Y.H. has no conflict of interest to disclose.
Funding Information
No funding was received for this project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.