
Abstract

A 31-year-old G0 was referred for dysmenorrhea concerning for endometriosis in the setting of Mullerian anomaly with a rudimentary uterine horn on imaging.
Magnetic resonance imaging (MRI) noted a right unicornuate uterus with a left rudimentary horn without clear endometrial tissue. The left ovary measured 8 cm long, stretching into the left lower quadrant (Fig. 1).
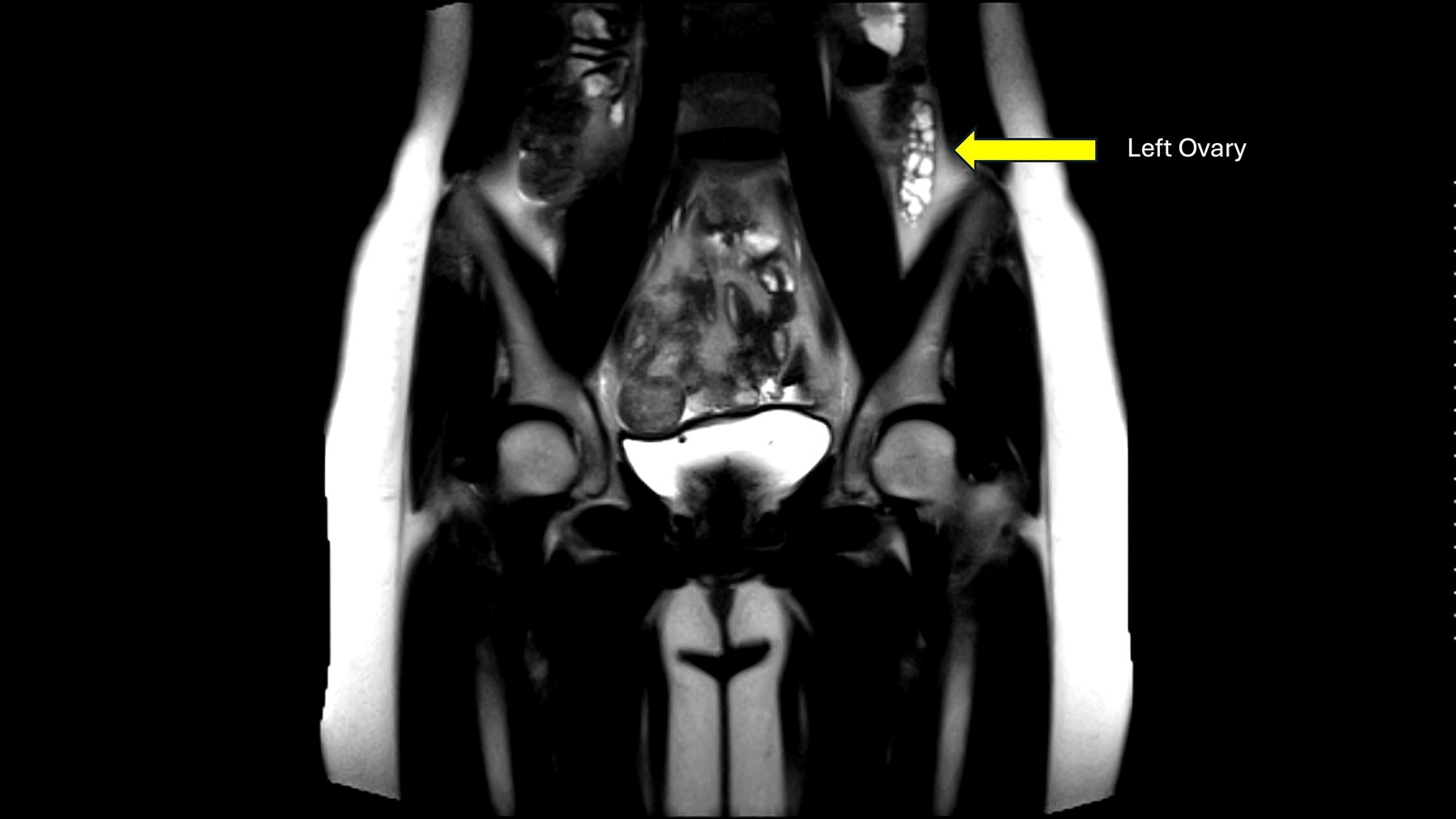
Coronal MRI image with elongated left ovary with many follicles.
Her infertility specialist recommended removal of the uterine horn. She was found to have an 8-week sized right unicornuate uterus and a non-communicating left rudimentary horn remnant (Fig. 2). The left ovary was profoundly elongated and the left tubal isthmus and ampulla were obliterated with only distal fimbria present (Fig. 3). The right tube and ovary were normal. Stage IV endometriosis per AAGL criteria was identified with a partially obliterated posterior cul-de-sac and extensive implants.
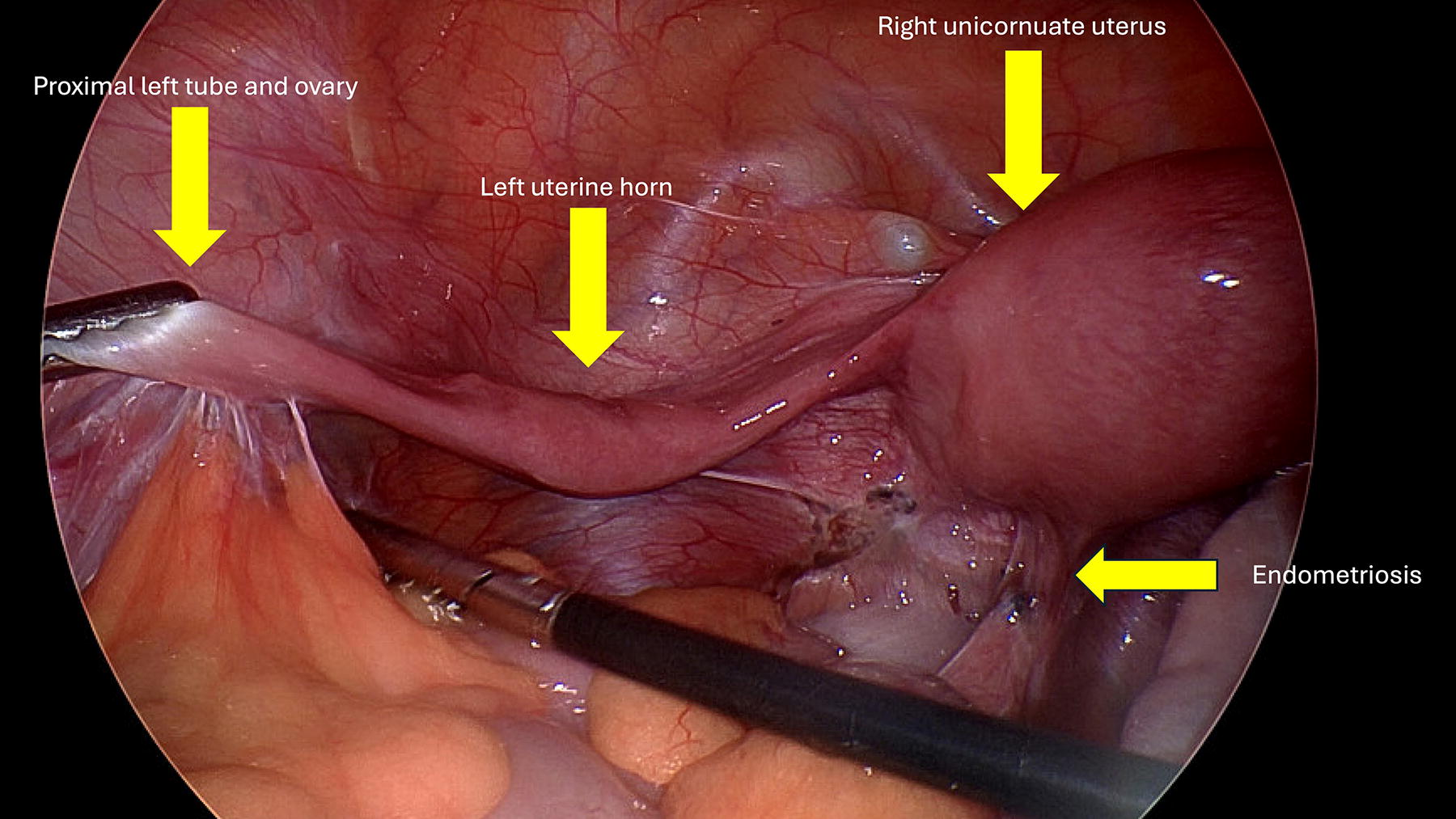
Right unicornuate uterus, left rudimentary uterine horn, and proximal left tube/ovary.

Elongated left ovary.
After placement of a uterine manipulator, chromopertubation was performed without fill or spill of methylene blue in the left tube. Excision of the left fimbriated tubal remnant was performed. The left rudimentary horn round ligament was transected and the retroperitoneal space was opened to identify the left ureter and uterine artery. The rudimentary horn was dissected without disruption of the uterine vascular supply, noted to bypass the horn. She underwent extensive excision of endometriosis. The case and postoperative course were uncomplicated and estimated blood loss was 5 mL.
Pathology returned as (1) myometrium consistent with uterine horn, (2) fallopian tube, and (3) endometriosis.
Mullerian anomalies may present in several ways, including primary amenorrhea, abnormal bleeding, dysmenorrhea, and infertility. Uterine anomalies impact 5.5% of women, increasing to 8.0% in women with infertility, and 24.5% in women with both a history of miscarriage and infertility. 1 Mullerian anomalies often coexist with endometriosis and surgeons should be prepared to identify and excise endometriosis, even if the MRI is negative for endometriosis such as in this case.2,3
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.