
Abstract
Abstract
Thomas, Kate N., Keith R. Burgess, Rishi Basnyat, Samuel J.E. Lucas, James D. Cotter, Jui-Lin Fan, Karen C. Peebles, Rebekah A.I. Lucas, Philip N. Ainslie. Initial orthostatic hypotension at high altitude. High Alt. Med. Biol. 11:163–167, 2010.–-There are several reports on syncope occurring following standing at high altitude (HA), yet description of the detailed physiological responses to standing at HA are lacking. We examined the hypothesis that appropriate physiological adjustments to upright posture would be compromised at HA (5050 m). Ten healthy volunteers stood up rapidly from supine rest, for 3 min, at sea level and at 5050 m. Beat-to-beat mean arterial blood pressure (MAP, Finometer), middle cerebral artery blood velocity (MCAv, Transcranial Doppler), end-tidal PCO2 and PO2, and heart rate (ECG) were recorded continuously. After 14 days at HA, baseline MAP and MCAv were not different to sea level, although HR was elevated. Neither the magnitude of initial (<15 s) responses to standing, nor the time course of initial recovery differed at HA compared with sea level (p > 0.05). By 3 min of standing, MAP was restored to supine values both at sea level (−3 ± 12 mmHg) and HA (4 ± 10 mmHg), although there was more complete recovery of HR at sea level (+13 ± 10 b·min−1, p = 0.02 vs. + 23 ± 10 b·min−1, p = 0.01). Reduced MCAv at 3 min was comparable at sea level and altitude (both −16%). These data indicate that initial cardiovascular and cerebrovascular responses to standing are unaltered when partially acclimatized to HA.
Introduction
Methods
Subjects
Ten healthy individuals [(7 men; 3 women) aged 32 ± 12 years (mean ± SD); body mass index 22.1 ± 1.9 kg/m2 volunteered for this study, which was approved by the Human Ethics Committee of the University of Otago and conformed to the standards set by the Declaration of Helsinki. Subjects were informed of the experimental procedures and possible risks involved in the study and written informed consent was obtained. Subjects were not taking any medication, all were non-smokers, and none had any history of syncope, or cardiovascular, cerebrovascular, or respiratory diseases. None had any traveller's affliction or other known illnesses. By the time of testing, all subjects were free of the symptoms of acute mountain sickness as judged by the Lake Louise (Roach et al., 1993) and Environmental Symptoms Questionnaires (Sampson et al., 1983). None of the subjects reported regular episodes of orthostatic hypotension and/or related symptoms in their normal daily lives.
Experimental design
Subjects performed a supine-to-stand maneuver both at sea level and at high altitude (5050 m; referred to as HA from here). All subjects trekked to the laboratory at 5050 m over an 8-day period from 2800 m. Testing was then performed after 14 days at HA. During this period there was no further ascent.
Following a standardized period of supine rest (5 min), volunteers were instructed to assume a standing posture for 3 min. T = 0 was taken to be the moment they started rising from the supine position. Subjects were asked to sit up, swing their legs around, and stand up in one smooth motion (all within 3 s). They were also instructed to not use their left hand for support as they stood up, so as to avoid disturbing the Finometer recording. During the stand, subjects were requested to breathe normally and not speak, and remain as still as possible to reduce any influence of the skeletal muscle pump.
Measurements
Blood flow velocity in the right middle cerebral artery (MCAv) was measured continuously using a 2-MHz pulsed Doppler ultrasound system (DWL Doppler, Sterling VA, USA). The Doppler probe was maintained in position, at a fixed angle, using a commercial headpiece (Spencer Technologies, USA). Beat-to-beat BP was measured by finger photoplethysmography (Finapres Medical Systems, Biomedical Instruments, The Netherlands). During both the supine rest and stand, subjects were instructed to keep their hand at waist level. The Finometer uses a height correction system, whereby any changes in vertical displacement of the finger cuff relative to the heart are corrected for by a reference probe placed on the chest at the fourth intercostal space in the midclavicular line (heart level), and reconstructed brachial artery pressure is reported. Manual BP measures were conducted to confirm the accuracy of the Finometer recordings. In addition, previous studies from our laboratory have supported the use of tracking arterial pressure changes using non-invasive photophethysmography during initial standing (Thomas et al., 2009).
Subjects breathed through a respiratory mask (Hans-Rudolph 8980, Kansas City, MO) attached to a one-way non-rebreathing valve (Hans-Rudolph 2700). Both end-tidal PCO2 and PO2 were sampled continuously and measured using gas analyzers (model ML206 and ML240, ADInstruments, Colorado Springs, CO, USA). The gas analyzers were calibrated using known concentrations of O2 and CO2 prior to each testing session. HR was also recorded using 3-lead electrocardiogram via a Bio Amp (model ML132, ADInstruments, Colorado Springs, CO, USA). All data were sampled continuously at 200 Hz using an analog-digital converter (Powerlab/16SP ML795; ADInstruments) interfaced with a computer and displayed in real time during testing. Data were later analyzed using commercially available software (Chart version 5.4.2, ADInstruments).
Analysis
As described previously (Wieling & Van Lieshout, 1997), two main phases of each orthostatic response were considered: the initial response (during the first 30 s) and the “steady state” alterations (2–3 min). The blood pressure nadir was identified during the first 30 sec after standing (see Fig. 1) and a 1 sec average of each variable was taken around this point as this was thought to best represent the changes associated with initial standing. The “recovery” was taken as the point when each variable re-attained baseline following the nadir. The “steady state” was approximated by the average of the last 30 sec of the 3 min stand.
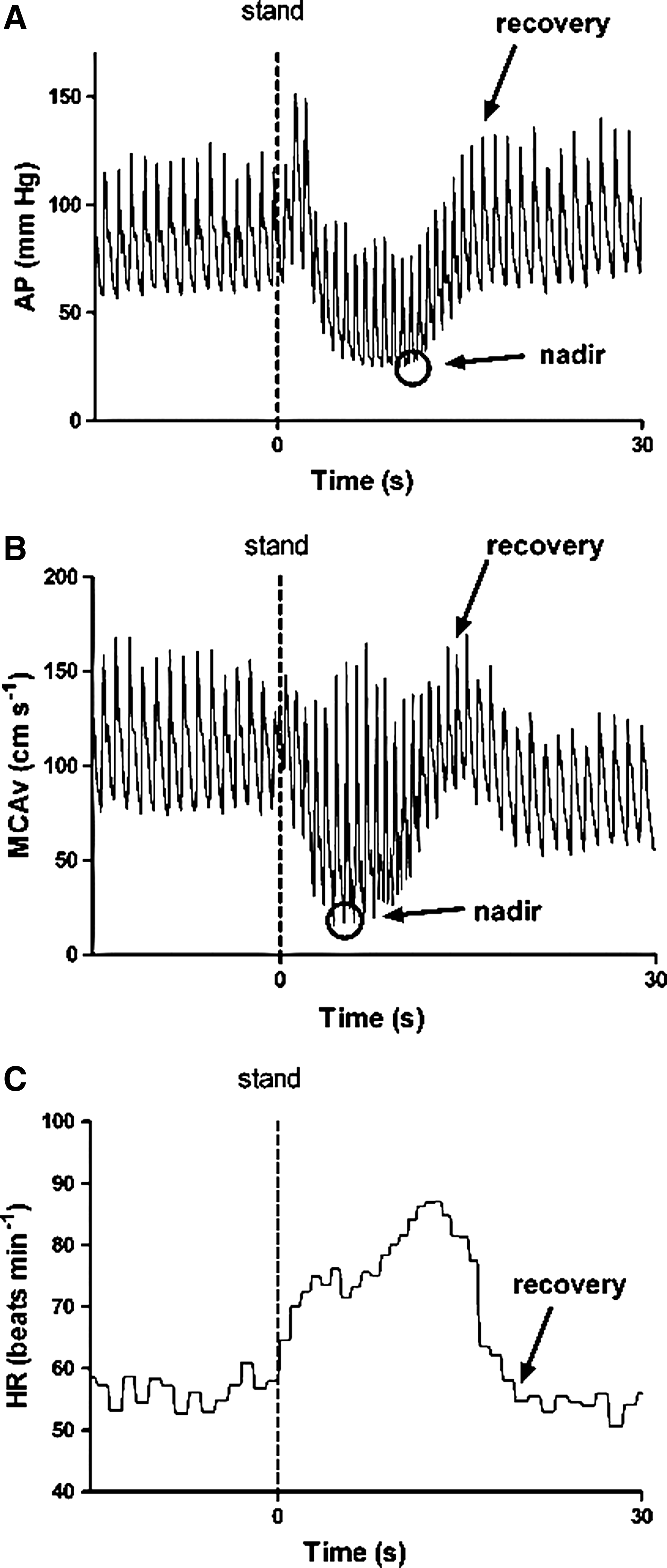
Representative trace of a 15 sec baseline and the first 30 sec of standing in one subject. AP, beat-to-beat arterial pressure; MCAv, middle cerebral artery velocity; HR, heart rate. The nadir and/or recovery on each is highlighted.
Statistical analysis
All group data are expressed as mean ± standard deviation (SD). To assess the effect of HA exposure and posture, dependant variables were compared using analysis of variance (ANOVA) (SPSS v17, SPSS, Chicago, IL). Post hoc analysis (paired t-test) of significant ANOVAs was performed (Bonferroni). A paired t-test was used to compare the relative changes between sea level and HA in the dependant variables induced by the postural change. Significance was established using an alpha level of 0.05.
Results and Discussion
While baseline MAP and MCAv were not different between sea level and after 14 days at 5050 m, HR was elevated (61 b·min−1 vs. 79 b·min−1, respectively; p = 0.006); and, as expected, both end-tidal PCO2 and PO2 were reduced [40 vs. 22 mmHg (CO2); 108 vs. 47 mmHg (O2); p < 0.0001) (See Table 1).
Values expressed as mean ± SD.
Denotes different from sea level (p < 0.05).
MAP, mean arterial blood pressure; SBP, systolic arterial blood pressure; DBP, diastolic arterial blood pressure; MCAv, mean middle cerebral artery velocity; SMCAv, systolic middle cerebral artery velocity; DMCAv, diastolic middle cerebral artery velocity; HR, heart rate; PCO2, end-tidal carbon dioxide; PO2, end-tidal oxygen.
Responses to standing upright
The magnitude of the initial change in the main dependant variables from supine to stand was comparable at sea level and HA (MAP: −38 ± 16 mmHg from baseline at the nadir vs. −40 ± 8 mmHg respectively; MCAv: −39 ± 11% vs. −42 ± 13% respectively; Fig. 2). However, the MAP nadir was reached significantly faster at HA than at sea level (8 vs. 10 s; p = 0.03) (Fig. 3). Times to initial recovery were not different between sea level and HA maneuvers. These data indicate that there is a similar initial response to standing up at sea level and HA. The faster drop in BP with standing at HA likely reflects a temporary mismatch between peripheral vascular resistance and cardiac output; however, the comparable magnitude of drop in BP and comparable time for correction of the hypotension indicates that the initial arterial baroreflex response to standing is well-preserved after 14 days at HA.
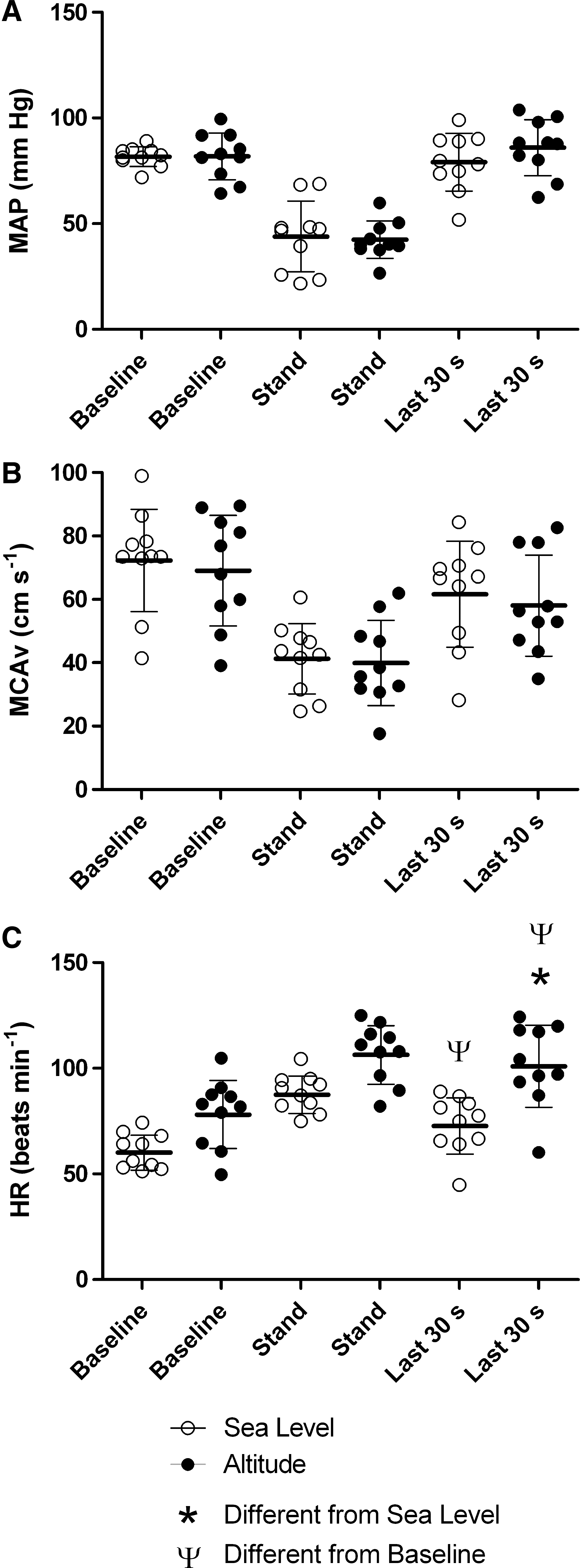
Baseline, the nadir of the initial stand and steady-state stand (mean of last 30 sec) at sea level and high altitude for MAP, MCAv and HR. Data are individual results with the bars representing mean ± SD. MAP, mean arterial pressure; MCAv, middle cerebral artery velocity; HR, heart rate; *denotes different from sea level, Ψ denotes different from baseline (p < 0.05).
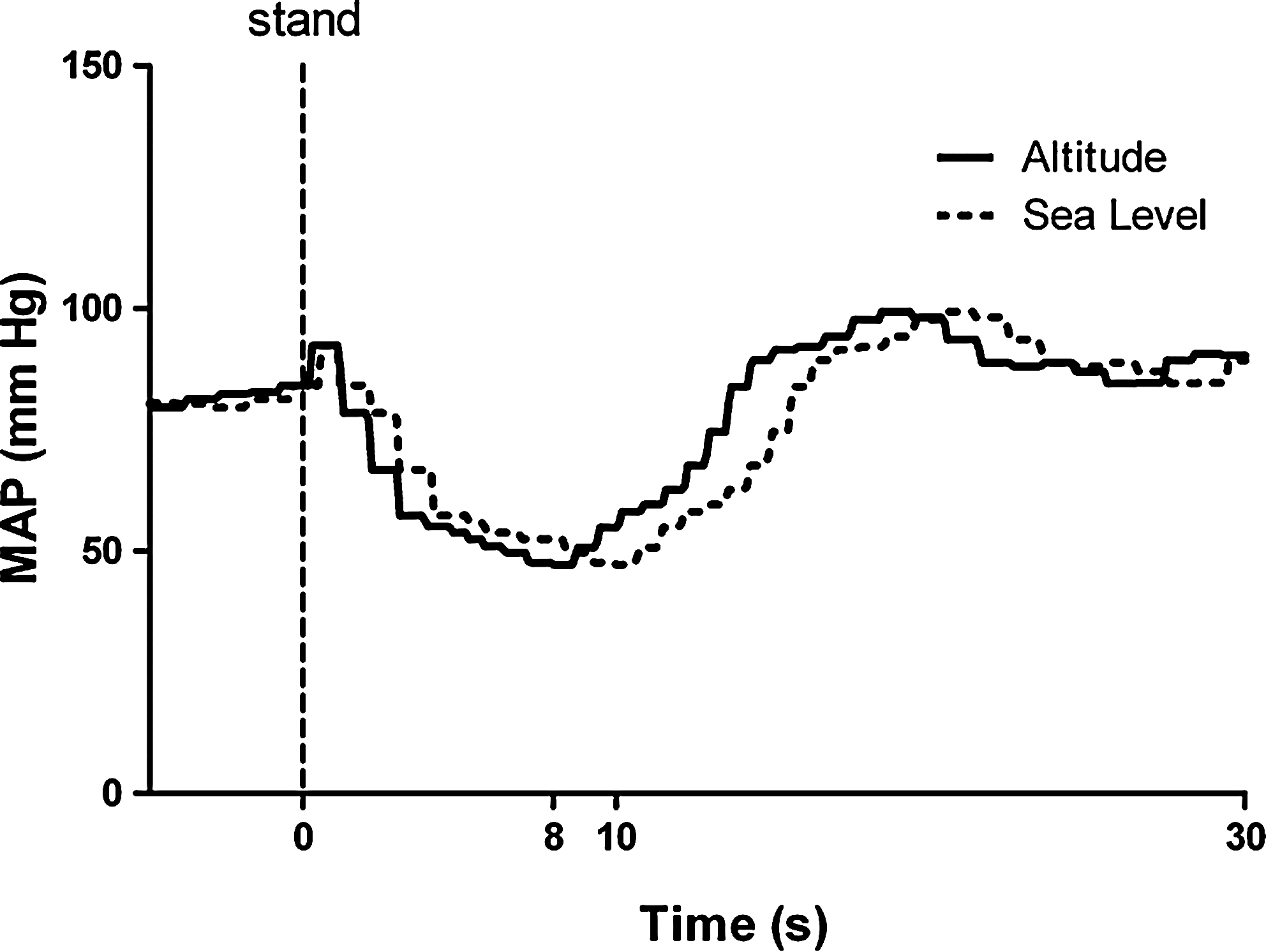
Mean arterial pressure (MAP) over 5 sec of baseline and the first 30 sec of standing at sea level and high altitude. The blood pressure nadir was reached significantly faster at high altitude than at sea level (8 vs. 10 sec; p = 0.03). Times to initial recovery were not different between sea level and altitude maneuvers.
During the steady-state stand (last 30 sec), MAP values were restored from the initial change both at sea level [79 (supine) vs. 82 mmHg (stand)] and at HA (86 vs. 82 mmHg). However, HR at HA remained elevated (102 vs. 79 b·min−1; p = 0.01), whereas at sea level the disparity was less (73 vs. 61 b·min−1; p = 0.02). The reduction in MCAv at the end of 3 min was comparable at sea level and at HA (16% lower than baseline in both). Thus, comparable to the initial responses to standing (<15 sec), it would seem that the physiological adjustments over a longer period in the upright posture are also maintained at HA.
The unaltered MCAv response to the transient hypotension and related recovery indicates that dynamic cerebral autoregulation and baroreflex-correction of dynamic cerebral autoregulation (Ogoh et al., 2008), respectively, are well maintained. Although previous studies have indicated that dynamic cerebral autoregulation is impaired during supine rest at HA (Levine et al., 1999; Jansen et al., 2000; Ainslie et al., 2007), it would seem that this impairment does not lead to a translated compromise in cerebral perfusion in the upright posture.
Technological considerations
Comparisons with other studies are difficult as previous work has used the head-up tilt test (HUT) to study orthostatic hypotension at HA (Malhorta et al., 1976; Malhorta & Murthy, 1977; Fulco et al., 2001). HUT has emerged as a reproducible test for diagnosing unexplained syncope in clinical practice (Brignole et al., 2004) despite huge variations in specificity and sensitivity (Kapoor et al., 1994). However, the hemodynamic alterations associated with IOH and syncope have been shown to differ considerably (Thomas et al., 2009). Our question revolves around orthostatic tolerance upon initial standing, since it is the most relevant physiological measure for trekking and climbing at HA. Our findings are contradicted by an earlier study (Mytton et al., 2008), in which the initial fall in SBP was greater after 4–5 days at 5200 m. However, that study measured BP via auscultation 15 sec after standing and therefore may have missed the nadir and misrepresented the trend of the blood pressure response. In fact, as a more integrative assessment of cerebral perfusion was not recorded, the authors acknowledged that the time course of BP may have been different at HA, as we found, and this may partly explain their results. Unfortunately, although it would seem unlikely, no data are available which have examined whether hypoxia per se (without the confounding factors of the field conditions associated with experimentation at HA) affects IOH.
Since transcranial Doppler measures flow velocity and not CBF per se, we prefer to assess and analyze relative changes in CBF velocity rather than absolute values. Nevertheless, research indicates that CBFv is a reliable and valid index of CBF (reviewed in Secher et al., 2008; Ainslie & Duffin, 2009) and mirrors the reported increases in CBF upon initial exposure to HA (<24 hours, peaking around 8 hours) as determined by the direct Fick method (Severinghaus et al., 1966; Roy et al., 1968).
In summary, our findings indicate that initial cardiovascular and cerebrovascular responses to standing are unaltered following partial acclimatization to HA. Thus, at least under the conditions tested, particularly following partial acclimatization, it would seem that the ability to maintain adequate balance and stability during such situations is not compromised by an impairment in cerebral perfusion.
Footnotes
Acknowledgments
This study was carried out within the framework of the Ev-K2-CNR Project in collaboration with the Nepal Academy of Science and Technology as described in the Memorandum of Understanding between Nepal and Italy and thanks to a contribution from the Italian National Research Council. We extend our thanks to ADInstruments and Compumedics Ltd for the use of their laboratory equipment. This study was supported by the Otago Medical Research Foundation, SPARC New Zealand, The Peninsula Health Care p/l and Air Liquide p/l.