
Abstract
Abstract
Richalet, Jean-Paul. Operation Everest III: COMEX '97. High Alt. Med. Biology 11 121—132, 2010.—Eight male volunteers, aged 23 to 37, were selected to participate in a simulated ascent to 8848 m in a hypobaric chamber. They were first preacclimatized in the Observatoire Vallot (4350 m) before entering the chamber. The chamber was progressively decompressed down to 253 mmHg barometric pressure, with a recovery period of 3 days at 5000 m from days 20 to 22. They spent a total of 31 days in the chamber. Seventeen protocols were organized by 14 European teams to explore the limiting factors of physical and psychological performance and the physiological and pathological changes in various systems (cardiac function, control of ventilation, autoregulation of cerebral blood flow, energy balance and body composition, muscle performance, erythropoiesis, and cognitive functions). All subjects reached 8000 m, and 7 of them reached the simulated altitude of 8848 m. Three subjects complained of transient neurological symptoms, which resolved rapidly with reoxygenation. At 8848 m (n = 5), Pa
Introduction
Science in the field is a challenge, but possible to achieve. However, the exposure of humans to the environment of high altitude regions induces various physiological adjustments or pathological manifestations that are not always clearly attributable to one or another stressor associated with this particular milieu. Altitude hypoxia, cold, dryness of air, inadequate food or liquid intake, exhaustion, and psychological stress are the main factors that could modify human physiology and behavior at high altitude. The difficulty of interpretation of some results of our previous field studies led us to consider the organization of simulated chamber experiments. The first objective of hypobaric chamber studies is to isolate hypobaric hypoxia from the other stressors. The possibility of using advanced technology and sophisticated equipment, as well as ethical and safety considerations, gives a clear advantage to chamber studies as compared to field studies when the effect of hypoxia is the main question (Richalet et al., 1999). Our first experience in hypobaric chamber studies was in 1989: Operation Everest Turbo demonstrated the positive effects of preacclimatization in a hypobaric chamber before an expedition to Mount Everest (Richalet et al., 1992). Objectives of Operation Everest III were to use the advantages of chamber studies (pure hypoxia, advanced technology, safety) to address specific questions remaining unanswered by previous chamber or field studies.
Subjects
Eighteen male subjects volunteered to take part in the study (Fig. 1). Eight subjects and one reserve were selected to enter the study for baseline normoxic measurements. Finally, 8 of them underwent the altitude chamber program. Their mean characteristics were as follows: age 26.6 ± 4.3 yr, body weight 74.3 ± 6.6 kg, height 180 ± 6 cm.

The group of Operation Everest III volunteers at the end of the experiment, just after leaving the chamber.
Methods
Location and schedule of experiments
Subjects were studied at the COMEX S.A. facilities in Marseille, France. The hypobaric chamber consisted of three rooms: (1) a spherical study room (diameter 5 m, available volume 65 m3) connected to (2) a cylindrical living room with eight sleeping bunks and a table for meals (length 8 m, available volume 32 m3) via (3) an air-lock room usable for toilet and shower (available volume 8 m3). Food and drinks, urine and blood samples, and any necessary small object could be transferred between outside and inside the chamber via two air-lock devices. Subjects were constantly monitored through five video cameras and audio systems by two technicians who were continuously present to manage the chamber, day and night. During daytime, a medical doctor was present in the control room. During nighttime, a doctor could be called at any time and be present on the site within 15 min. Oxygen masks were available at each bed, in the dining room, and in the study room. An emergency pack was usable inside the chamber by one of the subjects, a doctor trained in high altitude emergencies. In case of severe problems necessitating emergency evacuation, a subject could be taken out of the chamber within 30 min from 8848-m equivalent altitude and more quickly from lower altitudes (Richalet et al., 1999; Richalet, 2003). Written informed consent was obtained from all subjects. The protocols were approved by the ethical committee of the University Hospital of Marseille. Special recommendations from the committee were to restrict blood gases to arterialized capillary blood sampling and maximal exercise no higher than 7000 m.
Protocols
Seventeen protocols were executed by 14 scientific teams from France, England, and the Netherlands to study the effect of prolonged hypobaric hypoxia on various systems (Richalet et al., 1999). The main questions addressed were the following:
Clinical aspects and high altitude pathophysiology (Schneider et al., 1998; Mason et al., 1999; Richalet et al., 1999; Bouquet et al., 2000; Barry et al., 2002; Cauchy et al., 2002; Molenat and Boussuges, 2002) Body composition, metabolism, nutrition, and energy balance (Westerterp et al., 2000; de Glisezinski et al., 1999; Westerterp-Plantenga et al., 1999; Joanny et al., 2001) Cardiac function and autoregulation of cerebral blood flow (Boussuges et al., 2000; Ter Minassian et al., 2001) Gas exchange, acclimatization, and control of ventilation (Pedersen et al., 2000; Richalet et al., 1999) Role of hemoconcentration on the impairment of aerobic performance, sensorimotor control of skeletal muscles (Caquelard et al., 2000; Robach et al., 2000; Richalet, 2003). Markers of erythropoiesis during prolonged exposure to increasing altitude (Robach et al., 2004). Psychological adaptation to prolonged hypoxia: cognitive aspects, influence of mood states and personality traits, decision taking, and solving group problems (Abraini et al., 1998; Bouquet et al., 1999; Nicolas et al, 1999; Bolmont and Abraini, 2001; Bolmont et al. 2000; Bolmont et al. 2001; Bolmont and Abraini, 2001; Nicolas, 2003; Tougne et al., 2008).
Schedule of experiments (see Fig. 2):
Basal normoxic measurements. Performed on the 9 subjects within the chamber with open doors, March 10–16, 1997.
Preacclimatization period. To shorten the time spent within the chamber, subjects pre-acclimatized in the Alps at Refuge des Cosmiques (3650 m) for 1 day and Observatoire Vallot (4350 m) for 7 days. This period was planned both to allow a rapid entrance to the chamber at 5000 m and to test the ability of the subjects to withstand high altitude and community life in a hostile environment. During this period, subject 6 suffered from high altitude pulmonary edema (documented by X ray after evacuation at Chamonix hospital). He was excluded from the study and the alternate subject (9) was then fully included.
Hypobaric chamber period. Subjects descended from Observatoire Vallot on April 1 at midday and entered the chamber on April 2 at midday. They spent their first night in the chamber at 4500 m and then went up to 5000 m, where they started the experimental procedures. The pressures were chosen as the real pressures for the latitude of Mount Everest, up to 253 mmHg for the altitude of 8848 m. At the lowest barometric pressure of 253 mmHg, the subjects spent 6 h on day 30 and 4 h on day 31. Subjects spent their last night in the chamber at 5000 m, after the last “summit” climb. During the days when no experiment was performed, subjects were strongly encouraged to exercise on the treadmill or the cycloergometer. Most of them did so (30 to 90 min/day), although their motivation decreased considerably with increasing altitude.
Recovery period. Subjects left the chamber on May 2 and underwent the return to sea level (RSL) experiments until May 5. This type of observation is unique: very few studies have explored the time course of physiological and psychological parameters after return to normoxic conditions.
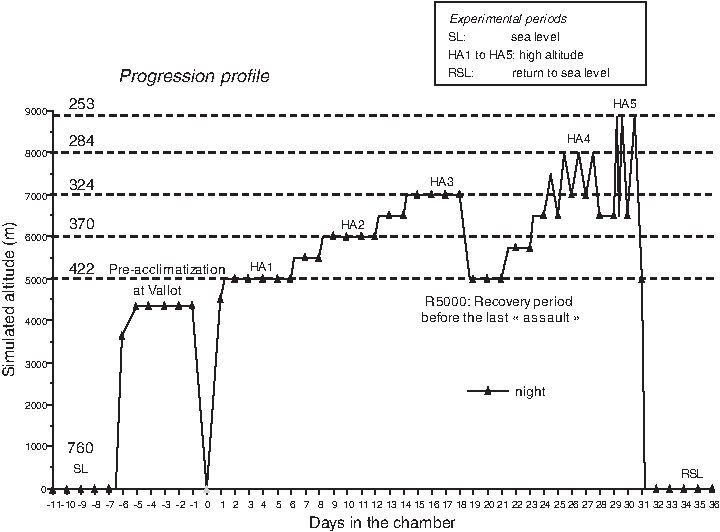
Simulated progression profile of. SL, HA1 to HA5, R5000, RSL: periods of experimental studies (Richalet et al., 1999).
Clinical outcome
Three subjects did not follow the complete schedule (Cauchy et al., 2002). Subject 1 experienced neurological symptoms at 8000 m (day 25): while performing a cognitive test, he suddenly could hardly speak and write. These symptoms rapidly disappeared when breathing pure oxygen, but a severe headache of migraine type could not be relieved by oxygen breathing and was not tolerated by the subject. A decision to evacuate the subject was taken and executed while breathing oxygen. Subsequent neurological examination, fundoscopy, and cerebral magnetic resonance imaging were entirely normal. Subject 8 suffered from neurological symptoms at 8848 m (day 29): he felt dizzy and could not recognize his friends within the chamber and had the sensation of floating in air. All signs disappeared with oxygen inhalation, but the subject and his colleagues were still anxious and, for safety reasons, he was evacuated from the chamber. Neurological examination and magnetic resonance imaging performed after evacuation were entirely normal. Subject 3 suffered from neurological symptoms at his second ascent to 8848 m (day 30): sudden pain in the back, paralysis of the left lower limb, with aphasia and facial paralysis. Symptoms disappeared rapidly with oxygen inhalation. He was brought down to 6500 m where he felt perfectly well. He was kept under oxygen inhalation while his colleagues underwent their third ascent to 8848 m and stayed with them at 5000 m during the last night in the chamber. Neurological examination and magnetic resonance imaging performed after leaving the chamber were entirely normal. All three cases shared a possible triggering factor in that each experienced hyperventilation alternating with straining against a closed glottis shortly before the onset of symptoms. An episode of decompression sickness could also be evoked (see discussion). Several weeks later, a persistence of open foramen ovale was investigated by transesophageal echography with contrast, but was negative (Cauchy et al., 2002). Altogether, all subjects reached 8000 m and 7 reached 8848 m, among whom 5 reached the “summit” three times.
Environmental conditions
Pressure variations were continuously monitored in the chamber. During experiments, temperature was, most of the time, kept between 18 and 24°C. Percentage of humidity in the chamber varied with outside ambient humidity and was mostly between 30% and 60 %. Day–night rhythm was maintained: subjects woke up at 07:00–07:30 and went to bed between 22:00 and midnight.
Investigators
There were no more than two investigators at the same time in the chamber. At very low barometric pressures (284 and 253 mmHg ), they breathed pure oxygen for 30 min before entering the chamber to avoid decompression sickness. They used supplemental oxygen at all altitudes. Oxygen was supplied through a type of space suit with a hood. Exhaled gas was pumped directly from the hood. The possibility for leakage of oxygen to the chamber was thus minimal, and the comfort of the investigator was maximal. However, at the lowest barometric pressure of 253 mmHg, some leakage occurred for a short period, such that the values of blood gases taken in two subjects during this specific period had to be discarded.
Equipment and methods
Daily questionnaire, body weighing, and basal physiological parameters were recorded in the morning just after waking up and before breakfast. Liquid and food intake was carefully measured daily by weighing all food and drinks entering and leaving the chamber. Daytime food intake, outside principal meals (breakfast, lunch, dinner), was noted by the subject himself by careful weighing using a table food scale within the chamber. Twenty-four hour urine was collected and weighed daily outside the chamber. Acute mountain sickness (AMS) score (Lake Louise Consensus) was self-recorded. Rectal temperature was taken every morning before getting up. Heart rate, systemic arterial pressure, and transcutaneous arterial saturation were measured daily in the morning before breakfast. Blood hemoglobin concentration was obtained through peripheral venous blood sampling and measured by a CO-oximeter (Chiron Diagnostics, model 270, Emeryville, California, USA). The CO-oximeter was kept inside the chamber and was calibrated for each chamber pressure. Blood gases were measured from arterialized capillary blood obtained from an ear lobe previously heated with capsaicin cream, which allows minimal error when compared to arterial blood gases in hypoxic conditions. The blood gas analyzer (Chiron Diagnostics, model 348) was outside the chamber, and capillary blood samples were passed through an air lock and analyzed within 2 min after sampling. Maximal oxygen uptake was measured using a step-by- step progressive exercise regime on a cycloergometer until exhaustion. Ventilation, oxygen, and CO2 concentrations were analyzed using a medical graphics system (CPX/D cardiopulmonary exercise system, Minneapolis, MN), modified for low partial pressures of CO2 and with a more powerful gas pumping system for high altitudes. The apparatus was kept within the chamber and functioned perfectly at 7000 m. Cardiac function and pulmonary artery pressure were assessed by transthoracic echocardiography. An echocardiograph machine (GE Ultrasound Vingmed CFM 750, Horsholm, Denmark) was kept outside the chamber, but the probe was inside the chamber and connected to the machine using a lead-through into the wall. All other equipment was kept inside the chamber.
Results
The main purpose of the present paper is to give a general description of the study and summarize the main results that have been published elsewhere.
Clinical aspects and high altitude pathophysiology
Total AMS score was almost zero at 5000 m thanks to the preacclimatization period on Mont Blanc. Symptoms appeared at 5500 and 6000 m, increased at 6500 m, and were maximal at 7000 m. During the recovery period at 5000 m, the AMS score went back to zero after 3 days, stayed very low upon reascent until 7000 m was reached again, peaked on the third ascent at 8000 m, but was lower during ascent to 8848 m. Among the four items included in the AMS score, the trend for each symptom was different (Richalet et al., 1999). The headache score was zero at 5000 m, peaked at 7000 m, and was relatively low at 8000 and 8848 m. At 6000 and 7000 m, there was a progressive decline with time as a result of clinical acclimatization. Gastrointestinal symptoms were zero up to 5500 m, increased on the first days at 6000 and 7000 m, and then declined rapidly with time at a given altitude. However, they increased with successive intermittent exposures to 8000 m. Fatigue increased with time and altitude up to 7000 m, progressively returned to zero after 3 days of recovery at 5000 m, and then rose again with altitude and reached its maximum on third exposure to 8000 m, whereas the exposure to 8848 m was better tolerated, probably because it was shorter. Dyspnea score always showed a peak on day 1 at a new altitude, progressively increased with altitude with a peak at 6500 m, did not completely return to zero on recovery at 5000 m, increased again with reascent, and reached its maximum at 8848 m. Ataxia score was very low during the whole period except at 7000 m, on the first exposure to 8000 m, and at both exposures to 8848 m. Quality of sleep was already impaired at 5000 m, progressively deteriorated with altitude up to 7000 m, took 3 days to restore on recovery at 5000 m, and increased again and peaked during the nights spent at 7000 m between days at 8000 m. Recovery after descent to sea level was immediate.
Sa
There was a progressive slight increase of mean rectal temperature with altitude (from 36.5°C at sea level to 37.0°C at 7000 m); but the most striking observation was peaks of temperature at 7000 m in some subjects (up to 38.5°C), with a concomitant rise in the clinical AMS score; high values of rectal temperature were seen only when the AMS score was high (Richalet et al., 1999).
Variation of color vision index in the red–green axis with altitude was monitored. Color index decreased with altitude at and above 6000 m, showing a slight relation with AMS: the color vision index was lower when AMS was different from zero (significant when score equals 2 or 3). Color discrimination was mainly altered in the red and blue ranges when a minimum threshold of difference between color stimuli is not present (Bouquet et al., 2000).
Nocturnal cough frequency (measured by voice-activated tape recorders during sleep) and cough-receptor sensitivity to citric acid challenge increased with altitude. This original observation refutes the common hypothesis that altitude cough is due to cold, dry air and suggests that other mechanisms, such as pulmonary interstitial edema, might be involved (Mason et al., 1999).
Previous descriptions of feelings of nasal blockade during inspiration at high altitude led us to measure nasal peak inspiratory flow (NPIF) at sea level, 5000 m, and 8000 m. NPIF increased with altitude exposure, but less than oral peak inspiratory or expiratory flow, suggesting flow limitation in the nose despite lower air density. This limitation could be because of swelling of the nasal structures obstructing the airway, similar to the edema observed in the subcutaneous tissue or in the lung interstitium. The impact of this limitation on ventilation and exercise performance remains to be established (Barry et al., 2002). The protective role of nitric oxide (NO) in hypoxic pulmonary vasoconstriction and pulmonary hypertension was evaluated by giving
The risk of decompression sickness (DCS) during experiments in hypobaric chambers is high, especially in investigators who are intermittently exposed to hypobaria. Signs of DCS (the bends, or joint pains) were observed in 3 subjects with a 15.6% overall incidence (50% above 8000 m), even with oxygen breathing before entering the chamber. Nitrogen venous gas emboli (VGE) were detected using two-dimensional echocardiography and pulsed Doppler ultrasonography; VGE were present in all but one subject with DCS symptoms and preceded the bends in all cases. It is therefore suggested that systematic detection of VGE by echography will be useful to prevent DCS since it allows an early detection of subjects at risk (Molenat and Boussuges, 2002).
Body composition, metabolism, nutrition, and energy balance
Body weight loss was maximal on day 29: 5.4 kg (7.3% of initial body weight). During the preacclimatization period on Mont Blanc, 1.4 kg was already lost. Then the loss was progressive up to 7000 m. As soon as day 1 of recovery at 5000 m, 0.7 kg was recovered and 0.15 kg more within two more days. Reascent to 8848 m led to a further loss of 1.7 kg in 7 days. The individual maximal weight loss varied from 2.9 to 10.0 kg and was related to initial body mass index (r = 0.877, p < 0.005). The rate of weight gain after return to sea level was dramatically high: after 4 days of recovery, mean body weight increased by 3.4 kg, that is, 63% of the total weight loss, suggesting fluid retention with return to sea level, which is consistent with an observed rebound in plasma aldosterone (Robach et al., 2000).
A biopsy of subcutaneous adipose tissue was performed before and at the end of hypoxic exposure to study in vitro changes in adipose tissue sensitivity. The lipolytic response to epinephrine, isoproterenol, growth hormone, and parathormone decreased, as did the plasma concentration of free fatty acid. The exposure to hypoxia led to a potent reduction in lipid mobilization through a decrease in the efficiency of adipose tissue α-receptors (similarly to what is observed in the heart), growth hormone, and parathormone lipolytic pathways, as well as an increment in the α-2-adrenergic antilipolytic effects (de Glisezinski et al., 1999). These observations suggest that, after an initial increase in fat mobilization owing to negative energy balance, the body tends to preserve its fat reserve after prolonged exposure to severe hypoxia, similar to the desensitization of cardiac α-receptors that preserves cardiac function in spite of low O2 availability.
Energy and water balance were studied by weighted dietary records and doubly labeled water (2H218O). Energy intake decreased by 11% at 5000 m, by 22% at 6000 m, by 44% at 7000 m, and by 55% at 8000 m. Mean energy intake over the whole period decreased by 40% and energy expenditure, by 9%. Overall, insensible water loss was unchanged because the increase in respiratory evaporative water loss was counterbalanced by a decrease in metabolic rate. The well-known altitude-induced body-weight loss is therefore, in the present study, clearly attributable to the decreased energy intake, even with free access to food in a hypobaric chamber (contrary to field conditions) (Westerterp et al., 2000).
Despite highly palatable food, subjects switched to a nibbling eating pattern. Meal size was reduced through a more rapid increase in satiety. Daily meal frequency increased from 4 to 7 eating occasions. At 7000 m, uncoupling between hunger and desire to eat occurred and prevented the food intake necessary to meet energy balance requirements. Finally, exposure to hypobaric hypoxia per se induced a change in attitude toward eating and a decrease in appetite and food intake (Westerterp-Plantenga et al., 1999).
Gas exchange, acclimatization, and control of ventilation
Resting values of P

Diagram relating resting Pa
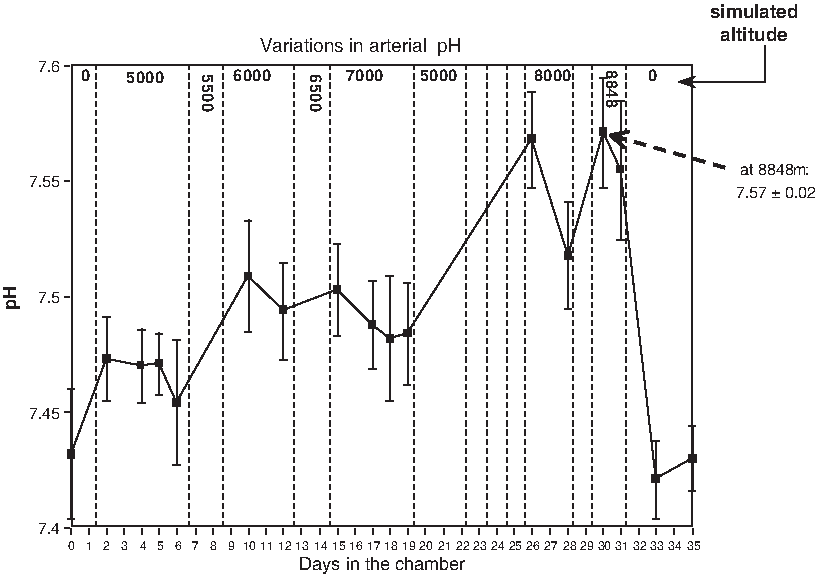
Variations in pH during Operation Everest III. Note a progressive increase in pH with altitude (respiratory alkalosis) and, for a given altitude, a progressive decrease of pH with time (partial renal compensation of alkalosis): see, for example, at 7000 and 8000 m.
The persistent hyperventilation that remains after ventilatory acclimatization to hypoxia (VAH) is partly owing to changes in acid–base status (alkalosis), but also to an altered activity of the carotid body (CB). To assess this hypothesis, subjects were acutely exposed to hyperoxia (30 min) at various simulated altitudes. For the second 10 min of this exposure, subjects were given a CB inhibitor, dopamine (3 μg/min/kg). Although there was both a rise in ventilation and a decrease in end-tidal P
Cardiac and ventilatory responses to hypoxia (breathing hypoxic mixtures from P
Cardiovascular function
Cardiac function was evaluated by echocardiography at rest up to 8000 m. Aortic and left atrial diameters, left ventricular (LV) diameter, and right ventricular end-systolic diameter fell progressively with increasing altitude. Mitral peak E velocity (early LV filling) decreased, peak A velocity (filling due to auricular contraction) increased, and E:A ratio (an index of early–late LV filling) decreased (Fig. 5A). Systolic pulmonary arterial pressure increased: the right ventricular–right atrial gradient increased from 19 ± 2.4 mmHg at sea level to 40.1 ± 3.3 at 8000 m and remained elevated 2 days after return to normoxia (Fig. 5C). All indexes of LV contractility were normal (Fig. 5D). However, there was a modification of the LV filling pattern, with a decreased early filling and a greater contribution of the atrial contraction, without elevation of LV end-diastolic pressure (Fig. 5B). These modifications of LV filling, assessed for the first time in hypoxia, could be an adaptive response to tachycardia and reduced preload, or they could be the consequence of an impaired LV relaxation owing to ventricular interdependence or hypoxia per se (Boussuges et al., 2000).
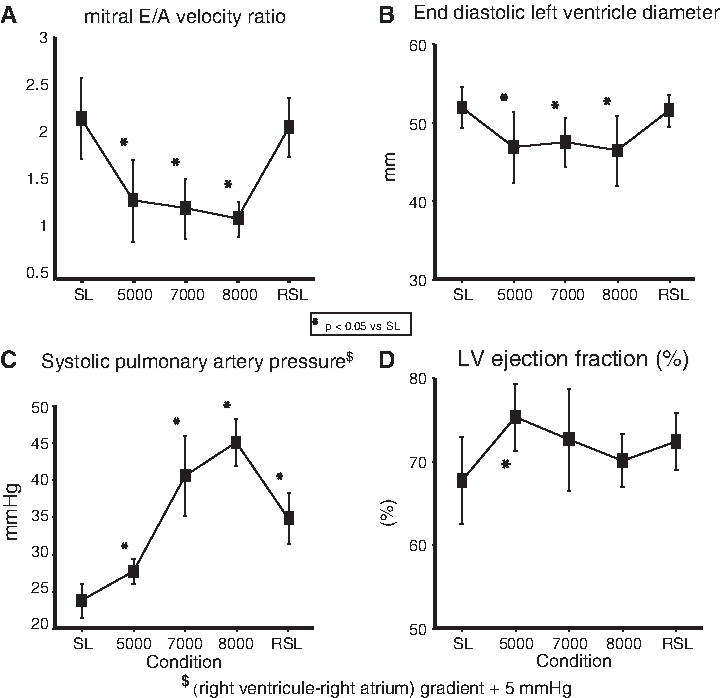
Cardiac function during Operation Everest III. (
Because cerebral hemodynamics may play an important role in circulatory adaptation to high altitude and in the pathophysiology of high altitude cerebral edema (HACE), transcranial Doppler measurements were performed up to 8000 m in basal conditions and after 3- to 5-sec compression of the left common carotid artery to evaluate the transient hyperemic response of the middle cerebral artery (MCA). MCA blood flow velocity increased only at 8000 m, and the corresponding pulsatility and resistivity indexes decreased over 5000 m. The transient hyperhemic response of MCA to compression was depressed at 8000 m, suggesting an impaired autoregulation of cerebral blood flow at extreme altitude. Through this mechanism, the brain could be more sensitive to rapid changes in arterial pressure and exposed to vascular damage (Ter Minassian et al., 2001).
Exercise and muscle performance, blood volume and erythropoiesis, and lipid peroxidation
As expected, maximal oxygen consumption decreased with altitude: −44% at 5000 m, −58% at 6000 m, and −59% at 7000 m. Maximal performance recovered almost completely with return to sealevel (not significant between SL and RSL).
The role of plasma volume changes in the decrease in maximal oxygen consumption (V
The responses of soluble transferrin receptor (sTfR), serum erythropoietin (Epo), red cell volume (RCV), and ferritin were investigated as markers of erythropoiesis during the simulated ascent, and sTfR was related to EPO response. The progressive decompression from SL to 8000 m induced a large parallel rise in EPO (33.8-fold) and sTfR (5.9-fold), whereas ferritin was dramatically decreased and iron intake reduced. RCV was increased by 29% after 31 days of decompression. We compared these variations in subjects acutely exposed to 4350 m for 1 week (Observatoire Vallot): EPO peaked at day 3 at 4350 m, then declined later at altitude, and returned to baseline values when returned to sealevel (RSL), whereas sTfR progressively rose at altitude (+86%) and remained elevated during RSL (+64%). Ferritin progressively declined at 4350 m, whereas iron intake was unchanged. RCV was not enhanced after exposure to 4350 m. We can conclude that sTfR mirrors EPO response for a given level of altitude hypoxia, but differs from EPO response during transitory phases, such as early acclimatization or reoxygenation. Analysis of sTfR may therefore account for altitude-related erythropoiesis at a time when EPO is blunted (Robach et al., 2004).
Exposure to prolonged and severe hypoxia alters exercise capacity, but the specific effects of severe hypoxia on muscle contraction had never been explored before. Maximal voluntary contractions (MVCs) of the flexor digitorum and static handgrips sustained at 60% MVC were performed up to 7000 m and 1 day after RSL. A decreased amplitude and increased duration of the M-wave (muscle EMG response to nerve stimulation) were observed, suggesting an alteration of muscle membrane properties that persisted after return to normoxia. This alteration could be due to lipoperoxidation, as shown by a companion study performed in the same conditions (Joanny et al., 2001). In contrast, modest alterations of the muscle strength were observed. A decreased endurance time to sustained fatiguing contractions was observed only at 7000 m. The most striking observation is that the contraction-induced fall of the median frequency of the EMG power spectrum (shift to the left) was attenuated in hypoxia. To explain the phenomenon of muscle fatigue, it was suggested that a long-lasting activation of group IV muscle afferents may in turn inhibit motoneurone discharge and command to the muscle; hypoxia would exacerbate this phenomenon. In fact, further studies (Dousset et al., 2003) have shown that hypoxia suppresses the activation of these afferent fibers; so the hypothesis of a decrease in the central command owing to activation of afferent muscle fibers in hypoxia (“central governor theory”) can be rejected (Caquelard et al., 2000).
Lipid peroxidation and antioxidant defense systems were evaluated in whole blood at rest (up to 8848 m) and after maximal exercise (up to 6000 m and 2 days after return to normoxia) by thiobarbituric acid-reactive substances (TBARS), reduced glutathione (GSH), reduced glutathione:oxidized glutathione ratio (GSH/GSSG), and reduced ascorbic acid (RAA). At rest, whole blood TBARS, as markers of lipid peroxidation, increased by 23% at 6000 m, 79% at 8000 m, 94% at 8848 m and still by 81% after return to normoxia. After maximal exercise, TBARS increased at high altitude, but a more striking increase was observed after return to normoxia (+232%). GSH/GSSG decreased with altitude exposure and reexposure to normoxia, as well as to ascorbate. These findings suggest that oxidative stress is induced by prolonged hypoxic exposure, exacerbated by exercise, and maintained (or enhanced) after rapid reexposure to normoxia. These phenomena may be implicated in the decrease in neuromuscular and cognitive performance at extreme altitude (Joanny et al., 2001).
Psychological and cognitive aspects
Cognitive performance was evaluated by visual choice reaction time, Pegboard psychomotor test, and number ordination Rey test. A group of subjects remaining at sea level during the same amount of time served as control to eliminate the learning effect. Pegboard test was used in three versions: (1) using a single psychomotor task exploring a simple psychomotor ability, (2) using a complex psychomotor task by adding a recognition task of either a color stimulus (high semantic level) or (3) an abstract sign (low semantic level). The number ordination test was used to explore mental efficiency, and reaction time was used to explore simple stimulus–response skills. Simple tasks were altered at 8000 and 8848 m and remained altered 3 days after the return to normoxia. Complex tasks were altered above 5500 m and also remained altered after return to normoxia (Fig. 6). No change was found in the reaction time. Mental efficiency deteriorated only at 8000 and 8848 m, as well as 3 days after return to normoxia, when compared to the control group. None of these alterations was correlated to the clinical signs of AMS, whatever the altitude. Overall, these results indicate that prolonged exposure to hypoxia produces learning deficits and disrupts the development of stable task-specific motor processes. Simple tasks are not altered below 8000 m, suggesting that sufficient compensatory mechanisms to hypoxic stress occur, at least below a certain threshold. When complex tasks are involved, the deterioration happens at lower altitudes. Finally, the impairment observed could be the consequence of disruptions in the strategic learning and working memory processes, which are cognitive functions that are well known to involve frontal lobes (Abraini et al., 1998; Bouquet et al., 1999).
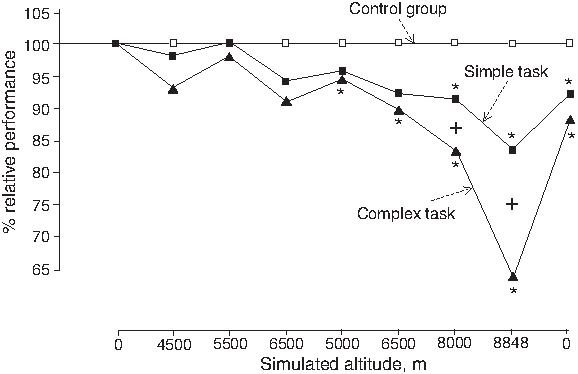
Cognitive performance during Operation Everest III. Variations of performance during a simple task (Pegboard test) and a complex task (adding another stimulus) compared to a control group staying in normoxia as reference. Note that performance is significantly altered at 8000 m and above and much more altered in complex than simple tasks (Bouquet et al., 1999).
Mood states were assessed using the Profile of Mood States (POMS) questionnaire, which explores six principal mood factors: tension, depression–dejection, hostility, vigor, fatigue, and confusion. Personality traits were assessed using the Sixteen Personality Factor Questionnaire (16PF), especially Factor C of the 16PF, which explores emotional stability: (individuals who face reality, calm, mature) vs. emotional instability (subjects affected by feelings, easily upset). Vigor and fatigue were the only two factors significantly affected by altitude, and not below 8000 m. A significant correlation was found between fatigue and emotional instability. Personality traits that reflect incapacity to face and control external realities and happenings would play a crucial role in the occurrence of adverse psychological reactions that may lead to life-threatening decisions at extreme altitude (Bolmont et al., 2000; Nicolas et al., 2000). When all mood scores were added, they correlated with state-anxiety, confirming the Spielberger hypothesis, which states that the development of state-anxiety responses to a stressful environment will closely parallel the occurrence of adverse changes in mood states (Bolmont and Abraini, 2001).
Personality traits related with anxiety were explored by the Spielberger State-Trait Anxiety Inventory and related to cognitive performance. Trait anxiety was positively correlated with mean reaction time, whereas no correlation was found with psychomotor performance or mental efficiency. These results suggest that anxiety could mediate the processing of information of stimulus–response tasks, but not of more complex and controlled tasks that require strategic processes (Bolmont et al., 2001). State-anxiety followed the same time course as the cerebral signs of AMS (adding scores of headache, difficulty sleeping, and ataxia), but not the respiratory signs. However, personality traits were not related to signs of AMS (Nicolas et al., 1999).
Any climber experiencing a real-life situation has to deal with complex decision making and problem solving, taking into account not only mapping and technical issues, but also available time, weather, and food supplies. Therefore, individual and group efficiency in problem solving was explored up to 8000 m. Individual performance in problem solving decreased at and above 5000 m, simultaneous to the increase in state-anxiety. On the contrary, collective performance was not altered by altitude exposure, suggesting that the collective success could be owing to the emergence of a positive appraisal of the situation. The high level of motivation allowed the group to compensate for most of the individual errors to cognitive impairment that occurred during the problem-solving sessions. The authors also emphasize the role of the first encounter of each subject with a problem to solve, which may provoke an irreversible increase in anxiety, as being responsible for a degradation of individual problem-solving abilities until the end of the expedition (Tougne et al., 2008). These findings may have considerable interest when analyzing the accidents occurring at extreme altitude, the incidence of which appears much greater when climbers are alone than when they can exchange their experiences in the face of a danger or difficulty.
Discussion
Detailed results of each protocol are presented and discussed elsewhere. However, general observations and comments can be made. This operation was a great success, both from a scientific and human point of view. Approximately 80% of the expected studies were completed. Seven out of eight subjects reached the maximal equivalent altitude of Mount Everest. No major accident occurred. The only comparable study previously organized along similar lines was Operation Everest II (OEII) in 1985 (Wagner, 2010). No major difference in the main clinically and physiologically measured parameters was found between the two studies. However, some interesting variations resulted from the different profiles of ascent. Preacclimatization at Observatoire Vallot allowed a much better clinical status at 5000 m during OEIII than during OEII: symptoms of AMS first appeared at 6000 m only. However, with exposure above 7000 m, headache, dyspnea, and lethargy were similarly present in both Operations. Body weight losses, owing mainly to a dramatic decrease in food intake, were similar, although slightly less in OEIII (7.3% vs. 8.9% of initial body weight). Great care was given to the choice of palatable food that was adapted every day to the mood and cravings of the subjects. This may explain part of the difference. The decrement in V
Footnotes
Acknowledgments
We express our gratitude to the crew of COMEX S.A. for its assistance to the investigators and to the subjects during the whole experiment. This experiment was made possible by grants from the Région PACA and Minist]ère Jeunesse et Sports, France. We are very grateful to the nine volunteers for their patience and courage throughout this exceptional experience: Kim Bodin, Emmanuel Cauchy, Guillaume Despiau, Jean-François Finance, Mathieu Gayet, Vincent Marchand, Guillaume Sabin, Philippe Serpollet, and Alexandre Héritier.
Disclosures
The author has no conflicts of interest or financial ties to disclose.