
Abstract
Abstract
Latshang, Tsogyal D. and Konrad E. Bloch. How to treat patients with obstructive sleep apnea syndrome during an altitude sojourn. High Alt. Med. Biol. 12:303-307.—Considering the high prevalence of the obstructive sleep apnea syndrome (OSA), it is expected that many patients with the disorder are traveling to altitude. However, this may expose them to the risk of pronounced hypoxemia, exacerbation of nocturnal breathing disturbances by frequent central apneas, impaired daytime performance, and high blood pressure. Recently, randomized studies specifically investigated the effects of altitude (1630–2590 m) in OSA patients and the optimal treatment in this setting. The results indicate that patients should continue to use continuous positive airway pressure therapy (CPAP) when sleeping at altitude. Since CPAP alone does not control central sleep apnea emerging at altitude, combined treatment with acetazolamide and CPAP should be considered, in particular, in patients with severe OSA and co-morbidities. Supplemental oxygen combined with CPAP might be advantageous in patients with OSA and concomitant cardiopulmonary disease by preventing hypoxemia and central sleep apnea. In patients unable to use CPAP or if electrical power is not available, an optimally fitted mandibular advancement device might be an alternative treatment option that can be combined with acetazolamide during altitude sojourns. Acetazolamide alone is also beneficial and better than no treatment at all, since it improves oxygen saturation, breathing disturbances, and the excessive blood pressure elevation in OSA patients traveling to altitude.

Introduction
The main manifestations of OSA comprise excessive sleepiness, impaired concentration, unrefreshing sleep with habitual snoring, and witnessed apneas (McNicholas, 2008). OSA represents a risk factor for traffic accidents and cardiovascular disease (Bradley and Floras, 2009). The diagnosis is suspected on clinical grounds and confirmed by a sleep study (McNicholas, 2008). The main treatment is nocturnal continuous positive pressure (CPAP) applied through a nasal or oral-nasal mask (Gordon and Sanders, 2005). CPAP splints the upper airway, thereby preventing airway occlusion with apneas, oxygen desaturation, and sleep disruption. Daytime symptoms usually diminish within a few days. Alternatives to CPAP include mandibular advancement devices (MAD) and surgery in selected cases (Randerath et al., 2011). Weight loss in obese patients and avoidance of alcohol and smoking are important adjuncts (Ryan, 2005).
OSA Patients at Altitude
Physiological consequences
Prompted by the observation that occasional obstructive apneas in healthy trekkers ascending to 5050 m in Nepal disappeared with increasing altitude while frequent central apneas/hypopneas emerged, Burgess and colleagues studied effects of altitude exposure in 5 men with OSA (Burgess et al., 2004). During sleep studies in normobaric hypoxia simulating an altitude of 2750 m, obstructive apneas were replaced by central sleep apneas (Burgess et al., 2006). Patz and colleagues reported on 11 OSA patients living at >2400 m evaluated by polysomnography at home, in a sleep laboratory at 1370 m, and (in 5 of the 11 patients) near sea level (Patz et al., 2006). Altitude descent resulted in a significant decrease in sleep-related breathing disturbances due to a decrease in hypopneas and central apneas. In order to corroborate these findings, we performed a randomized cross-over trial in 34 OSA patients studied during a few days off CPAP at 490 m, 1860 m, and 2590 m, respectively, in the Swiss Alps (Nussbaumer-Ochsner et al., 2010). Altitude exposure induced pronounced hypoxemia and increased sleep-related breathing disturbances due to frequent central apneas/hypopneas (Fig. 1). Daytime evaluation at altitude revealed that the patients performed poorly in driving simulator tests, had increased blood pressure, cardiac arrhythmias, weight gain, and leg edema suggesting water retention (Nussbaumer-Ochsner et al., 2010). These data suggested unfavorable health effects of altitude in untreated OSA patients. Since cardiovascular diseases and diabetes are common in OSA patients and since altitude worsens intermittently and imposes sustained hypoxemia, the resulting excessive sympathetic activation may expose patients to a high risk of adverse cardiovascular events at altitude.
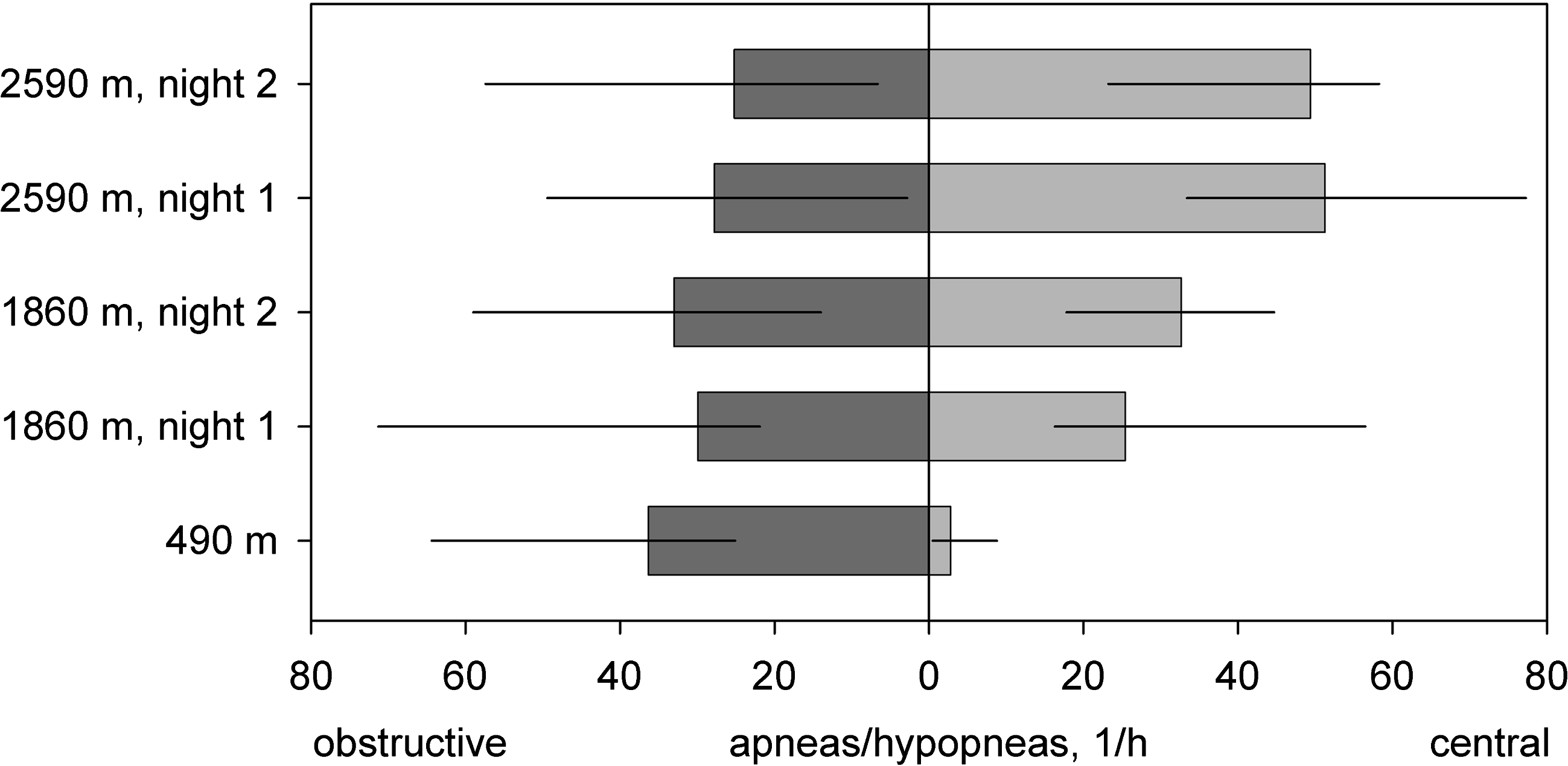
In patients with OSA syndrome studied at 490 m, 1860 m, and 2590 m, respectively, during a few days of CPAP withdrawal, altitude exposure was associated with a significant increase in the total AHI (represented by the total length of the horizontal bars). The increase was related to emergence of frequent central apneas/hypopneas (represented by bars to the right) while obstructive apneas/hypopneas changed little (bars to the left). Bars and lines are medians and quartile ranges from data in 34 patients reported by Nussbaumer-Ochsner et al. (2010).
Treatment of OSA at altitude
We recently performed a randomized, placebo-controlled, double-blind trial evaluating acetazolamide as a treatment for OSA at altitude (Nussbaumer-Ochsner et al., 2011). The study confirmed that acetazolamide (250 mg twice a day) significantly improved nocturnal oxygen saturation, reduced central apneas/hypopneas and sleep disturbances at 1860 m and 2590 m, when compared to no treatment at all (Nussbaumer-Ochsner et al., 2011). In addition, acetazolamide prevented excessive blood pressure rise and weight gain. However, a considerable amount of obstructive apneas/hypopneas persisted. Thus, acetazolamide provides some benefit but is not an optimal treatment for OSA at altitude. Nevertheless, it might be a valuable option if CPAP therapy is not feasible.
In a subsequent randomized, placebo-controlled, double-blind study we evaluated whether combined treatment with acetazolamide and CPAP was superior to CPAP alone (Latshang et al., 2010). Fifty-one OSA patients living below 800 m were studied during a sojourn of a few days in a Swiss alpine village at 1630 m and 2590 m, respectively. On combined treatment with CPAP (RemStar M-series, Philips Respironics, Andover, MA) and acetazolamide (250 mg in the morning and 500 mg in the evening), the apnea/hypopnea index (AHI) was normalized at both moderate altitudes. On CPAP alone, residual central apneas persisted. CPAP devices were operated in the automatic mode with a pressure range of 5–15 cm H2O. The applied pressure at 2590 m exceeded values at 490 m by 2 cm H2O if acetazolamide was not used; on combined autoCPAP and acetazolamide treatment, no difference in mask pressure between values at 2590 m and 490 m was noted. The data from this study suggest that the combined treatment seems to be appropriate for OSA patients at moderate altitude.
Theophylline has been shown to improve high altitude periodic breathing in healthy subjects (Fischer et al., 2004) but it is not an effective therapy for OSA and has the drawback of being arrhythmogenic and sleep disturbing. Modafinil is a stimulant that improves reaction time and subjective sleepiness in OSA patients during a few days of CPAP withdrawal (Williams et al., 2010). It might be of some use in very special circumstances when a patient is unable to use an effective OSA therapy but needs to maintain a high level of alertness. Since modafinil does not improve nocturnal breathing and oxygenation and considering its potential to trigger cardiovascular events, it is not generally recommended, in particular not in hypoxic conditions.
Custom-fitted mandibular advancement devices (MAD) improve sleep-related breathing disturbances, daytime symptoms, and vigilance in OSA patients at low altitude (Fig. 2) (Bloch et al., 2003; Randerath et al., 2011). Studies at altitude have not been performed so far but MAD seem to be promising for persons traveling frequently to the mountains and ready to make the effort of getting a custom-fitted appliance. It usually takes several weeks to fabricate a MAD and become accustomed to its use. Efficacy should be verified prior to travel with a sleep study, wearing the dental device for at least 4 days. This treatment can therefore not be established within short time before departing to high altitude. Prefabricated devices can be purchased at a lower cost than custom-fitted appliances, but they are less effective and therefore not recommended (Vanderveken et al., 2008).
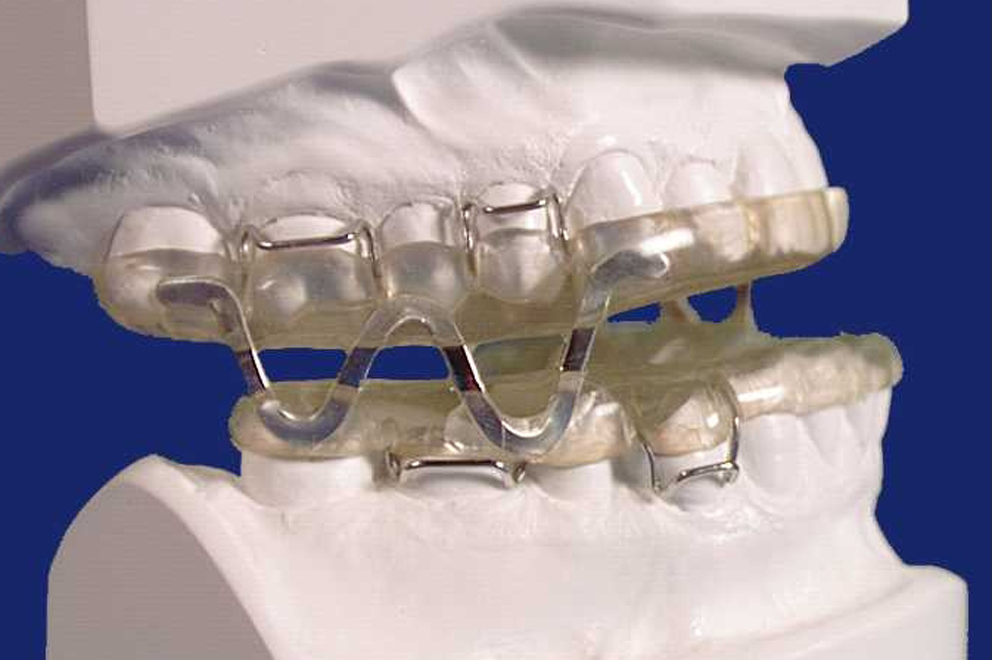
Mandibular advancement device. Monobloc device used for OSA therapy. Snapped onto the teeth during the night, this custom-fitted device holds the mandible in a protruded position thereby preventing upper airway occlusion with obstructive sleep apnea. A mandibular advancement device may be an alternative to CPAP therapy in frequent altitude travelers. Adapted from Bloch et al. (2000).
A nasal expiratory pressure device (Provent) consisting of valves inserted into the nares has been shown to improve OSA in highly selected patients (Berry et al., 2011). Further studies are required to evaluate whether Provent works at altitude. Nasal obstruction due to dry air at altitude might be a problem with this therapy. In OSA patients with coexistent chronic rhinitis, nasal decongestants (during an altitude sojourn of a few days) or topical steroids might be useful adjuncts that contribute to a better sleep quality and might also slightly improve OSA (Clarenbach et al., 2008; Kohler et al., 2009).
Surgical interventions have a limited role in the treatment of OSA and cannot be recommended in general. In particular, the effects of soft tissue surgery on snoring and OSA are unpredictable and might not persistent (Ryan, 2005).
Recommendations for OSA Patients Traveling to Altitude
Pre-travel considerations and preparation
Depending on the time until departure, the destination and duration of the planned travel, the sleeping altitude, the available infrastructure (electricity), co-morbidities, age, and other individual factors, preparations may vary considerably (Nussbaumer-Ochsner and Bloch, 2007; Nussbaumer-Ochsner and Bloch, 2010). General recommendations include sufficient and regular sleep, and avoidance of alcohol, sedatives, sleeping pills, and smoking. Concomitant illness such as cardiovascular disease, diabetes, and obstructive airway disease should be controlled and stable. Specific recommendations regarding diseases other than OSA have been reported elsewhere and are not further discussed (Dehnert and Bartsch, 2010; Luks and Swenson, 2007; Nussbaumer-Ochsner and Bloch, 2010). Patients should have sufficient supply of their regular medication and a reserve for emergencies. Counseling regarding susceptibility to, prevention, recognition, and treatment of altitude-related illnesses should also be provided (Bartsch et al., 2004; Maggiorini, 2010). If the use of acetazolamide during an altitude sojourn is planned, patients should be asked about allergies and previous use of acetazolamide. A short trial of the drug at home might be useful to get some experience, including with potential unpleasant effects (bad taste, paresthesias).
During the pre-travel consultation, effectiveness of OSA treatment, CPAP adherence, and any related problems should be assessed. Patients should be asked about residual sleepiness, unrefreshing sleep, and other symptoms suggesting incomplete control of sleep apnea. Application of the CPAP equipment in the office may identify an imperfect mask fit, leaks, and skin lesions that should be taken care of. Patterns of CPAP use and the AHI recorded in the internal memory of the CPAP device during home therapy should be downloaded to assess effectiveness of treatment (Ueno et al., 2010). Depending on the results, further evaluations including a sleep study on CPAP should be considered. In patients on fixed pressure CPAP, a 1–2 week autoCPAP titration period might help to determine the current effective mask pressure. In the absence of further scientific studies, it seems that autoCPAP works at altitude (at least with the one device used in the cited study) and might have the advantages over a fixed CPAP setting by continuously adjusting mask pressure according to the actual needs of the patient (Latshang et al., 2010). Virtually all modern CPAP devices can be operated at altitude, but manufacturer's documentation should be studied (according to the manufacturer's specification verified at the time of manuscript preparation, the most recent CPAP devices from ResMed, Philips Respironics, Breas, Weinmann, and Covidien incorporate altitude adjustment). Patients planning to use CPAP during travel should be made aware that an extension cord and adapters to connect the device to the power outlet might be required when traveling to foreign countries. CPAP devices can also be operated from the 12 V electrical circuit of a car or from portable 12 V batteries (which requires an inverter for some CPAP devices). However, the weight of batteries and the need for recharging are drawbacks. The use of a CPAP device with a humidifier should be considered to enhance comfort in dry altitude environments, although this increases power consumption and equipment weight. In patients with chronic rhinitis, nasal decongestants or topical steroids might be prescribed (Kohler et al., 2009). In regular altitude travelers with OSA, analysis of data stored in the CPAP device during use at altitude with pulse oximetry interfaced to the CPAP device might help to assess the control of sleep apnea and requirements for treatment adjustments during subsequent altitude sojourns.
For patients frequently traveling to altitude on treks away from electricity and who have sufficient time to establish this treatment, a custom-fitted MAD (Fig. 2) might be prescribed. MAD treatment generally requires a minimum of 6–8 upper and lower teeth (although cases of MAD therapy in edentulous patients have been reported) and absence of periodontal disease and temporomandibular joint pain. A pre-evaluation and subsequent adaptation of a MAD by a dentist with special expertise in this field is strongly recommended. MAD therapy usually requires a preparation during several months and is therefore not an option for patients immediately departing to altitude (Bloch et al., 2003; Randerath et al., 2011).
In patients with severe OSA and cardiovascular or pulmonary co-morbidity, supplemental oxygen applied into the CPAP tubing might be advisable and will reverse the adverse effects of being at altitude. The indication has to be assessed individually according to recommendations for the underlying disease (Luks and Swenson, 2007). Appropriate infrastructure has to be available and the oxygen dose has to be titrated according to the individual needs. Monitoring of pulse oximetry might be advisable. In patients with COPD, restrictive chest-wall or lung disease, or with neuromuscular disease, ventilatory stimulation by acetazolamide might impose an excessive load on respiratory muscles. It is therefore not generally recommended in these conditions at altitude.
Recommended OSA Treatment During Altitude Sojourns
OSA patents living at lowlands and sleeping at an altitude >1600 m without treatment are likely to experience pronounced hypoxemia, aggravated breathing disturbances, elevated blood pressure, and vigilance impairment during daytime (Nussbaumer-Ochsner et al., 2010). Patients should try to have the lowest sleeping altitude possible and be encouraged to continue using their CPAP therapy if feasible. Both auto-adjusting and fixed pressure modes are acceptable. The use of a humidifier might enhance comfort. As an alternative to CPAP, patients might use a custom-fitted and optimally adjusted MAD. General recommendations regarding prevention of high altitude-related illnesses, including a moderate ascent rate, avoidance of overexertion should be respected (Nussbaumer-Ochsner and Bloch, 2007). Depending on the sleeping altitude, severity of OSA, age, and co-morbidities, the use of acetazolamide might be advisable in combination with CPAP (Latshang et al., 2010) or a MAD. In healthy subjects, acetazolamide at a dose of 2×125 mg per day is sufficient to prevent acute mountain sickness. However, in OSA patients, a higher dose of 2×250 mg or 250 mg in the morning and 500 mg in the evening is recommended to treat sleep apnea at altitudes (Latshang et al., 2010). In settings where CPAP therapy is not feasible, OSA patients may benefit from acetazolamide alone since it is better than no treatment at all and mitigates hypoxemia and sleep-related breathing disturbances and improves subjective well-being at altitude (Nussbaumer-Ochsner et al., 2011).
A summary on pre-travel assessment and treatment of OSA patients at altitude is provided in Table 1. The proposed measures should allow patients to enjoy a refreshing sleep and wonderful daytime experiences in the mountains despite their OSA.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.