
Abstract
Abstract
Zhang, Haiyan, Jianzhong Lin, Yingchun Sun, Yongxia Huang, Huiming Ye, Xiaochuan Wang, Tianhe Yang, Xingtang Jiang, Jiaxing Zhang. Compromised white matter microstructural integrity after mountain climbing: Evidence from diffusion tensor imaging. High Alt. Med. Biol. 13:118–125.—The aim of the present study was to investigate cerebral microstructural alterations after single short-term mountain climbing. Voxel-based morphometry (VBM) analysis of gray matter (GM) and white matter (WM) volumes and Tract-Based Spatial Statistics (TBSS) analysis of WM fractional anisotropy (FA) based on MRI images were carried out on 14 mountaineers before and after mountain climbing (6206 m). In addition, verbal and spatial ‘two-back’ tasks and serial reaction time task were also tested. No significant changes were detected in total and regional volumes of GM, WM, and cerebral spinal fluid after mountain climbing. Significant decreased FA values were found in the bilateral corticospinal tract, corpus callosum (anterior and posterior body, splenium), reticular formation of dorsal midbrain, left superior longitudinal fasciculus, right posterior cingulum bundles, and left middle cerebellar peduncle. In all the above regions, the radial diffusivity values tended to increase, except in the left superior longitudinal fasciculus the change was statistically significant. There were no significant changes in the two cognitive tests after mountain climbing. These findings indicate that short-term high-altitude exposure leads to disturbances mainly in cerebral WM, showing compromised fiber microstructural integrity, which may clarify the mechanisms underlining some cognitive and motor deficits tested previously.
Introduction
In this study, voxel-based morphometry (VBM) and Tract-Based Spatial Statistics (TBSS) based on MRI images were employed to measure GM and WM changes in mountaineers. VBM is an automatic quantitative volumetric technique over the whole brain using voxel by voxel analysis without prior specification of regions of interest for analysis and it does not rely on arbitrarily predefined structures. Recently, the preprocessing steps of VBM have been improved with the Diffeomorphic Anatomical Registration Through Exponentiated Lie algebra (DARTEL) registration method, which can achieve more accurate inter-subject registration of brain images, accomplish accurate realignment of small inner structure, and attain the best results (Ashburner et al., 2007). VBM-DARTEL has been widely applied in clinical studies (Chen et al., 2011). TBSS is a newly introduced method. Here we used TBSS to measure fractional anisotropy (FA), examining alterations in fibrous microstructure properties of WM tracts. TBSS projects the FA values of individual subjects in given spatial locations to “FA-skeleton” of major WM structures, and thus improving sensitivity, objectivity, and interpretability of analysis of multi-subject diffusion tensor imaging (DTI) data (Smith et al., 2007). Moreover, diffusion tensor eigen values were also analyzed since they can help interpret FA changes in WM tracts by providing information regarding likely alterations in the proportion of longitudinally versus obliquely aligned myelinated fibers (Versace et al., 2008). Since working memory and procedural learning deficits have been reported during or after acute ascending to high altitude (HA), we tested these two sorts of cognitive functions, expecting to further explore whether the regional brain changes could clarify the mechanism.
Materials and Methods
Subjects
Fourteen healthy mountain climbing amateurs (males: 8; females: 6; mean age 21 years; range 19–23 years) from Xiamen University during summer holidays in August, 2009 were studied. They are lowlanders born and living at sea level below 300 m and they are without any prior exposure to HA. All are of normal body weight and body mass index. They all have no documented neurological disorder or history of head injury with loss of consciousness. The whole group had successfully completed, without the use of supplementary oxygen. The medical follow-up during the expedition consisted of the daily observation of the Lake Louise score (Roach et al., 1993), which was used for the assessment of acute altitude illness at altitudes, with a Lake Louise score greater than 4 being defined as acute mountain sickness. Physical examinations were used to determine health status. All participants were given written informed consent to participate in the study which had been approved by the Ethical Committee of Xiamen University.
Expedition to Tang-ku-la Mountains at Qinghai-Tibet Plateau
During days 1–5, the mountaineers left Xiamen for Lasa (3650 m) (the subjects stayed in Lasa for 2 days). Then the subjects spent 1 day reaching the first base camp (4600 m) at Tang-ku-la Mountains (the subjects stayed there for 1 day). On the tenth day, they started for camp 2 (5300 m) (the subjects stayed there for 10 days). On the twenty-first day, they came back to Lasa. After 5 days at Lasa (day 26), they completed the expedition and returned to Xiamen. All mountaineers reached the summit at 6206 m for 5 hours on day 14. The climbing schedule is shown in Figure 1.
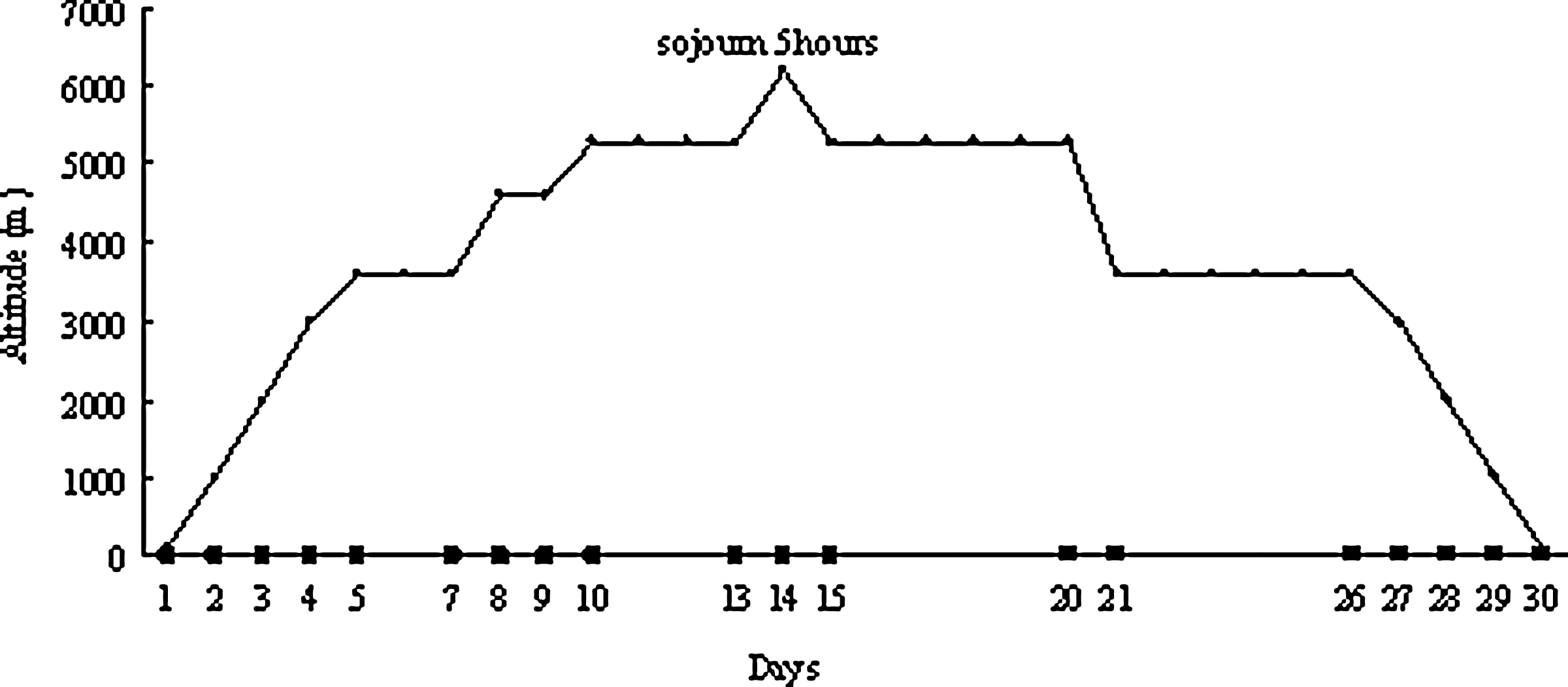
Climbing schedule of the expedition to Tang-ku-la Mountains.
Neuropsychological and physiological tests
The tests were performed by the same researcher 2 days before mountain climbing and within 1 day after return to sea level. Neuropsychological tests included: (1) Verbal and spatial ‘two-back’ tasks used to assess working memory; (2) Serial reaction time task used to measure simple visuomotor implicit procedural learning. The procedures of the two tests were used in our previous study (Zhang et al., 2011). Physiological tests included the pulse rate, arterial blood pressure, hematological values, arterial blood gas analysis, and pulmonary function. Paired-samples t test (using SPSS 13.0) measured the differences between before and after mountain climbing. Statistical significance was set at p<0.05.
MRI data acquisition
The brain MRI studies were conducted 2 days before and within 1 day after mountaineers had returned to sea level. Structural images were acquired on a GE 1.5 T Signa Excite Gemse MRI system (GE Medical, Milwaukee, WI) at the Magnetic Resonance Research Center (Zhongshan Hospital, Xiamen, China). A 3D structural MRI was acquired from each subject using a T1-weighted MPRAGE sequence: TR/TE=7.2 ms/1.6 ms, FOV=240×240 mm2, matrix=256×256, slice thickness=1.4 mm. A DTI pulse sequence with single shot diffusion-weighted echo planar imaging was applied sequentially in 16 different directions with b values (0 and 1000 s/mm2): The diffusion b-factors were set 0 and 1000 s/mm2. The echo planar imaging sequence was: TR/TE=12000/79.4 ms, FOV=240×240 mm2, acquisition matrix 130×128 with reconstruction matrix 256×256, in-plane resolution, 0.94×0.94 mm, and slice thickness, 4 mm with no gap. The following data analyses were conducted by two researchers who were blind to the status of subjects.
VBM analysis of 3D T1 images
The 3D T1 images were used for GM analysis using VBM8 toolbox implemented in SPM8 (Wellcome Department of Imaging Neuroscience, University College London, London, UK). The steps included: (i) the images were inspected and set at the anterior commissure. Each reorientated image was segmented into GM, WM, and CSF in native space and Procrustes aligned GM images were generated by a rigid transformation; (ii) the DARTEL was used to create study-specific template by the aligned images from all the patients and controls to improve inter-subject registration of structural images (Ashburner, 2007). The procedure implicated in six iterations, which began with the averaging of aligned data to generate an original template. Then, the first iteration of the registration was done on each subject and a new template was created. After this, the second iteration began. When six iterations were finished, the template was generated, which was the average of the DARTEL registered data. During iterations, all images were warped to the template yielding a series of flow fields that parameterized deformations; (iii) the normalized images were transformed into MNI space. These GM images were then smoothed using a Gaussian kernel of 8 mm full-width at half-maximum. Paired-samples t tests were performed to examine between-group differences. The statistical parametric map was generated with threshold at t>1.7709, p<0.05 (FDR corrected).
TBSS analysis of DTI
DCM2MII was used to convert diffusion tensor images from the proprietary scanner format to the NIFTI format. Then images were processed using FSL 4.1.5 software package (http://www.fmrib.ox.ac.uk/fsl/). Images were realigned to the b-value (b0) image to remove eddy current distortions and motion artifacts using FDT (FMRIB's diffusion toolbox) (Jenkinson and Smith, 2001). A brain mask was created from the first b0 image using BET (Brain Extraction Tool). After these processes, images were calculated with the FDT to generate FA maps. The analysis of FA images was performed using the TBSS package in FSL (Smith et al., 2007). The steps include: (i) align the FA images of all subjects to a template which was arbitrarily selected from those FA images by nonlinear registrations; (ii) transform all the aligned FA images into 1×1×1 mm3 MNI152 space by affine registrations; (iii) create the mean FA image and filter to retain only the center of the WM tracts so as to create the mean FA skeleton; (vi) project individual subjects' FA was put onto their skeleton; (v) following these steps, data were fed into voxel-wise cross-subject statistical analyses with the following group comparisons: before vs. after climbing and after vs. before climbing. In all cases, the null distribution was built up over 5000 permutations, and significance analyzed using Paired-samples t tests at p<0.05 levels, corrected for multiple comparisons.
Within the cluster of changed FA, the longitudinal (principal diffusion direction, λ1) and radial (transverse diffusion component, (λ2+λ3)/2) diffusivity values were also calculated.
Results
Physiological and psychological characteristics
The mean Lake Louise recorded at 5300 m was 3±1 (range 2–4) in all mountaineers. The symptoms included diarrhea (1 person), vomiting (2 persons), dizziness (5 persons), headache (5 persons), fatigue (2 persons), and common cold (2 persons). After mountain climbing, body weights were significantly decreased and pulse rates and vital tidals were significantly increased (all p<0.05). Hemoglobin levels and circulating red blood cell count were significant increased (both p<0.001); Base excess (BE) was significantly increased and pCO2 and HCO3- were significantly decreased (all p<0.05). No significant changes were found in arterial blood pO2 and SaO2.
There were no significant changes in working memory scores and reaction time after mountain climbing.
Total and regional volumes of GM, WM, and CSF
No subject showed visible abnormalities on T1-weighted structural images. VBM analysis showed no significant regional changes in GM and WM volumes after mountain climbing. Moreover, there were no significant changes in total brain volume and total GM, WM, and CSF volumes after mountain climbing.
FA and MD values
Whole brain voxel-wise TBSS analysis showed that mountaineers had significantly decreased FA values in a number of brain areas after mountain climbing (Fig. 2, Table 1). The regions included the bilateral corticospinal tract which was located in the left ventral pons and right posterior limb of internal capsule, corpus callosum (anterior and posterior body, splenium), reticular formation of dorsal midbrain, left superior longitudinal fasciculus located in inferior parietal lobule, right posterior cingulum bundles, and left middle cerebellar peduncle.
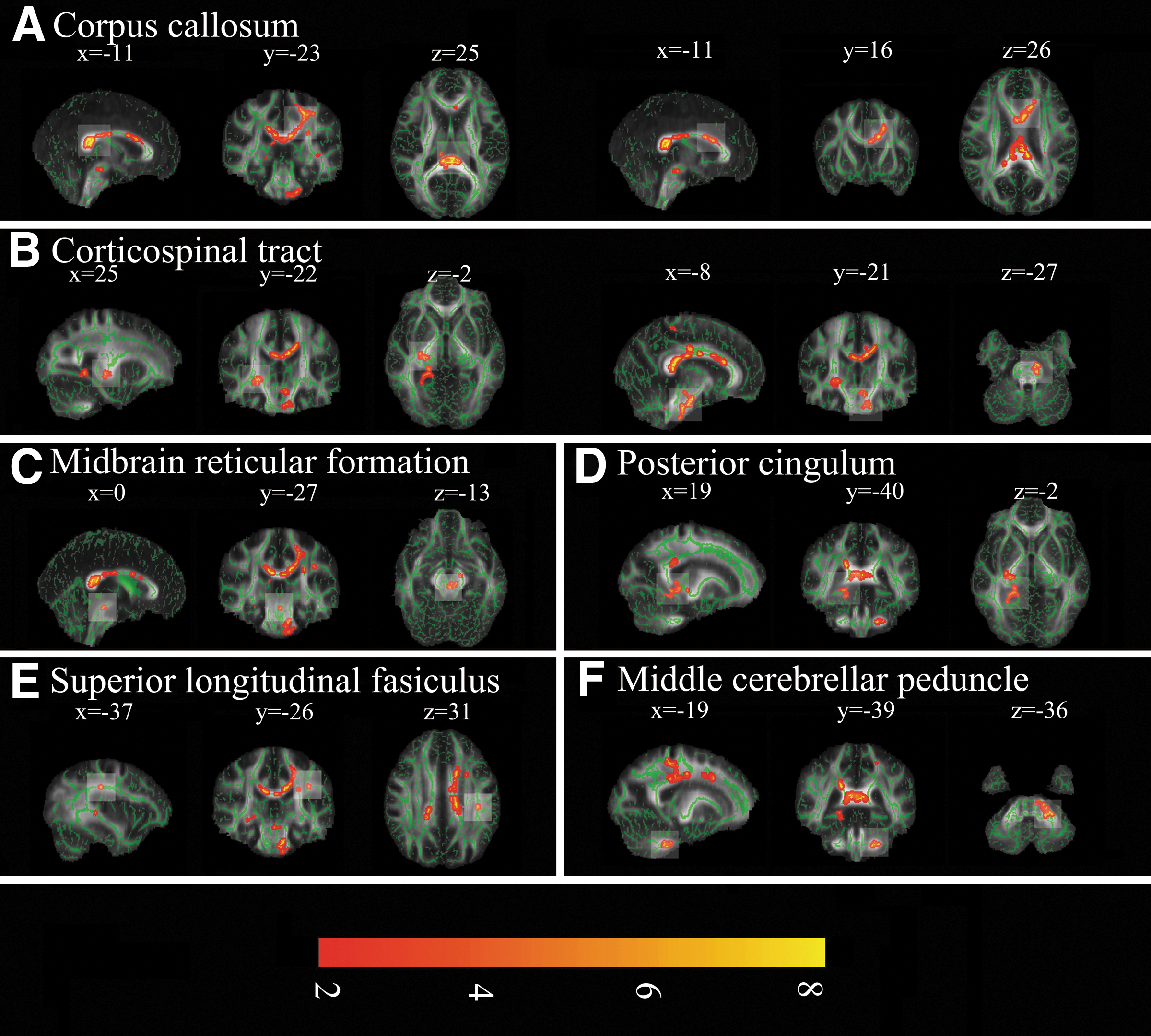
Regional decrease in FA in the mountaineers after mountain climbing (results of TBSS). The group's mean FA skeleton (green) was overlaid on the mean FA images. The threshold of mean FA skeleton was set at 0.2.
BA: brodmann area; CC: corpus callosum; CST: corticospinal tract; CP: middle cerebellar peduncle; PC: posterior cingulum; RF: reticular formation; SLF: superior longitudinal fasciculus. Data were present as mean (SD).
p<0.05.
The radial diffusivity values in the left superior longitudinal fasciculus located in the inferior parietal lobule showed significant increase after mountain climbing. However, in the other regions the radial diffusivity values tended to increase but the differences did not reach statistical significance. There was no significant change in longitudinal diffusivity value in any region showing decrease of FA after mountain climbing (Table 1).
Correlation of physiological measurements and neuropsychological performances with FA value
The changed FA value in the right posterior internal capsule showed correlation with the arterial blood pCO2 (r=0.655, p<0.05), BE (r=0.815, p<0.001), and HCO3- (r=0.778, p<0.001) after mountain climbing (Fig. 3).
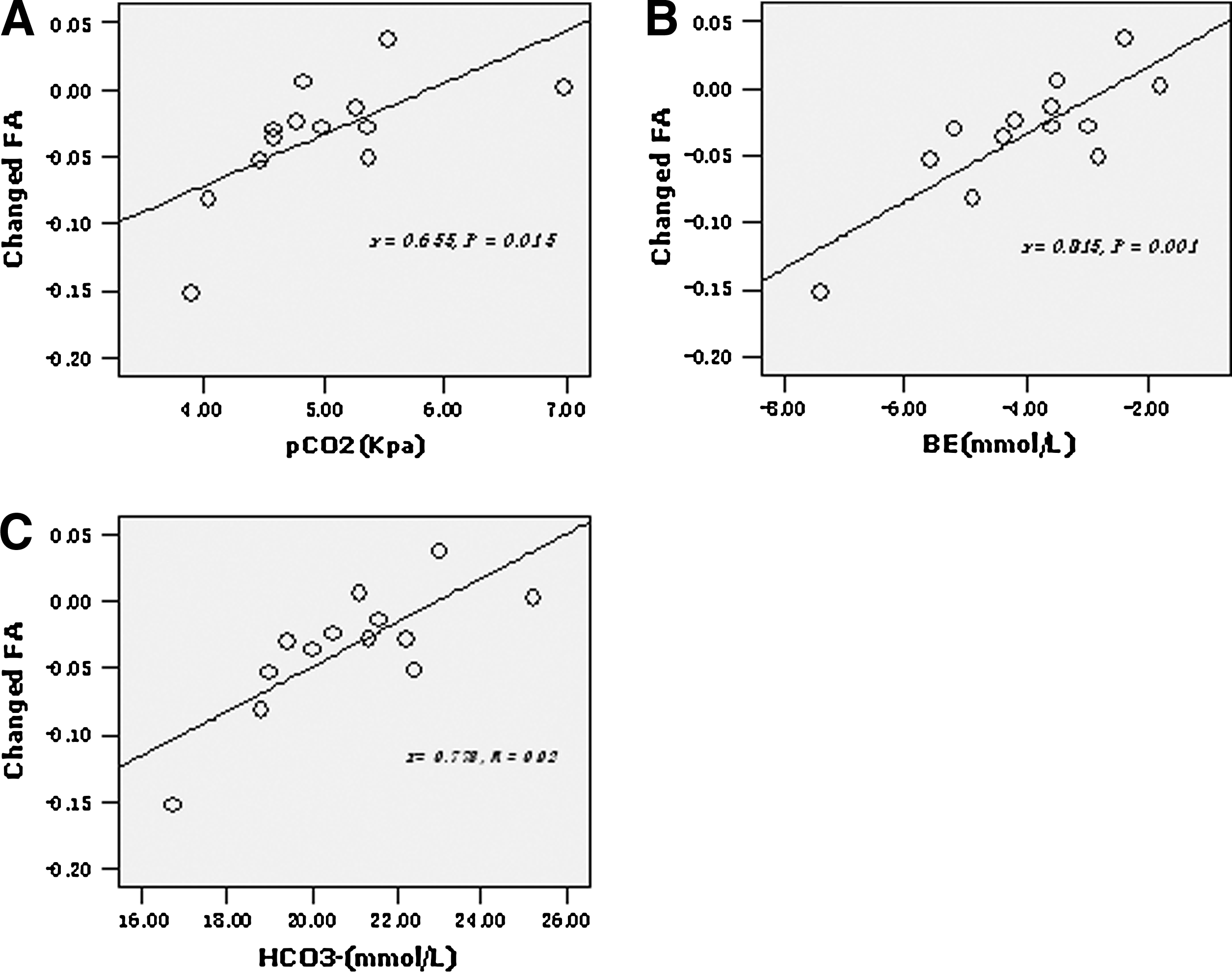
Changed FA value in the right posterior internal capsule showed correlation with the arterial blood pCO2
There was no strong correlation between neuropsychological performances and the decrease in FA value in any region.
Discussion
Mountain climbing has been proved to impair mountaineers' cognitions and motor performances. Moreover, previous PET and fMRI studies on single mountain climbing have revealed significant changes in cerebral glucose metabolism (Hochachka et al., 1999; Merz et al., 2006) and significant regional decrease in blood oxygen level dependent response in brain (Rostrup et al., 2005). In the present study, we performed MRI studies on short-term single mountain climbing and confirmed brain microstructural changes, which mainly showed regional decreases of FA in multiple sites of WM tracts.
FA reflects the structural integrity and geometry of axonal fibers (Gulani and Sundgren, 2006). Reduced FA is associated with local cerebral edema, compromised myelin structure, changed axonal morphologic structure, and/or altered interaxonal spacing of fiber bundles (Beaulieu, 2002; Drobyshevsky et al., 2007; Thomalla et al., 2004). Higher radial diffusivity reflects the lack of myelin and the increased freedom of cross-fiber diffusion in WM (Song et al., 2002). In the present study, the WM injury manifested as decrease in FA and a tendency to increase in radial diffusivity. The decreased WM FA found in our mountain climbers was consistent with the results from several previous studies on hypoxic/ischemic brains (Delsing et al., 2001; Kallenberg et al., 2007; Kusano et al., 2009; Thomalla et al., 2004). Previous studies have shown HA cerebral edema was caused by hypoxia that typically affected mountaineers who ascended rapidly to HA (Hackett et al., 1998; Hackett and Roach, 2004) and cerebral edema has traditionally been ascribed to vasogenic edema (Hackett and Roach, 2001). However, our results support the hypothesis of Bailey et al. (2009) that, in addition to vasogenic edema caused by hypoxia, cytotoxic edema might also be present. The limitation of this study is that we did not observe how long cytotoxic edema would take to resolve after mountain climbers returned to sea level. In laboratory study, Kallenberg et al. (2007) found that during 6 hours recovery in normoxia after 16 hours exposure to normobaric hypoxia, vasogenic edema resolved while cytotoxic edema persisted. They speculated that pO2-mediated inhibition of the decrease in the sodium-potassium pump might be a potential mechanism that cells used to reduce energy expenditure in hypoxia. In the present study, the reduction in pCO2 and HCO3- and the increase in BE persisted for a few days after descending from HA, which was consistent with the previous studies summarized by West (2004).
The decrease of WM volume in the corticospinal tract was measured in mountaineers who ascended to HA above 4000 m several times a year for at least 10 years (Di Paola et al., 2008) and in patients with obstructive sleep apnea (Macey et al., 2008), whereas the increase of FA in the corticospinal tract was found in our previous study on HA immigrants (Zhang et al., 2010), which suggests the corticospinal tract is particularly susceptible to hypoxia and different mechanisms may be involved in the effects of short-term and long-term hypoxia on the brain WM. Our findings of WM lesions in the corpus callosum, posterior cingulum bundles, cerebellum, and midbrain in the mountain climbers were in line with that found in the obstructive sleep apnea patients (Macey et al., 2008) and in the congenital central hypoventilation syndrome patients (Patwari et al., 2010).
Although no significant changes in regional GM volume were detected by VBM analysis, we cannot make a definitive statement about undamage of GM volume for the reason that cytotoxic edema in GM might occur. Cytotoxic edema affects both GM and WM, especially the GM (Hackett et al., 1998). Cytotoxic edema in GM, which DTI is not sensitive to detect, would have compensated the loss of neuronal cells. Our findings in regional and total brain volumes and CSF volume were not the same as that detected in other studies. For example, Di Paola et al. (2008) revealed a reduced GM volume in the left angular gyrus in mountain climber who had climbing for at least 10 years and were accustomed to reaching altitudes over 4000 m several times a year. Garrido et al. (1993) detected cortical atrophy and periventricular hyperintensity lesions in the T2-weighted images in almost half of the climbers who ascended to over 7000 m without supplementary oxygen. Usui et al. (2004) detected lesions in bilateral globus pallidus in two 63-year-old women after their arrival at HA of 3500 m. Fayed et al. (2006) found frontal subcortical lesions, cortical atrophy and enlargement of Virchow-Robin spaces in 35 climbers who went to mountains above 4810 m. In laboratory studies, Morocz et al. (2001) found an increased whole brain volume after subjects had been exposed to a simulated altitude of 4572 m (32 h) and Fischer et al. (2004) showed a decreased CSF volume after subjects had been exposed to a simulated altitude of 4500 m (10–12 h). The differences among us may be related to the HA exposure mode (intensity, pattern, and duration), because the other studies used a repetitive, acute, or more severe exposure.
The impairments of WM in the cerebellum and corpus callosum may clarify the mechanisms underlining cognitive deficits that tested in mountain climbers (Hornbein et al., 1989; Lieberman, 1994; Regard et al., 1989; Tripathi et al., 2005). Experimental and clinical evidence has shown that the cerebellar structures played a role in procedural learning, language, visual-spatial, executive, and working memory (Konczak and Timmann, 2007; Stoodley et al., 2011; Torriero et al., 2007). However, the impairments of the procedural learning and working memory after return from HA were not observed in our study. Similar to our results, a few publications reported no evidence of cognitive impairments after mountain climbing (Anooshiravani et al., 1999; Clark et al., 1983; Jason et al., 1989; Merz et al., 2006). In our study, decreased FA and increased radial diffusion were observed in corpus callosum, which suggests some behavioral impairment for the reason that the fibers in corpus callosum transfer inter-hemispheric information related to reading, calculation, and working memory (Ewing-Cobbs et al., 2006). Previous studies have shown that FA decreased in the anterior part of the corpus callosum in vascular dementia patients (Hanyu et al., 1999) and smaller sizes in the anterior and posterior part of corpus callosum were associated with greater decrease in the Mini Mental State Examination (Ryberg et al., 2011).
Several studies showed motor speed and precision were reduced in a hypoxic environment (Bolmont et al., 2000; Hornbein et al., 1989). The American Medical Research Everest Expedition showed impairment in finger-tapping (West, 1984). The cerebellum plays a major role in the planning, initiation, and organization of a movement (Oliveri et al., 2007) and the middle cerebellar peduncles are part of the cortico-ponto-cerebellar tract. Therefore, the impaired fibrous microstructure properties in the middle cerebellar peduncle could lead to deficient signal transmissions from prefrontal cortices to the cerebellum, resulting in the symptoms of motor and attention deficits in mountaineers. Previous study has shown that attention-deficit hyperactivity disorder children with motor and attention deficits had a lower FA in the right middle cerebellar peduncle (Bechtel et al., 2009). The corticospinal tract is the major neuronal pathway that mediates voluntary skilled movements in brain and the posterior limb of internal capsule is important location (Jang, 2009). Moreover, the corpus callosum is an important WM structure with regard to motor response control (McNally et al., 2010). Motor-specific corpus callosum subregions are fairly well established as the rostral body and anterior midbody subregions of the corpus callosum primarily having premotor, supplementary motor, and motor cortical fibers transversing through them (Ryberg et al., 2011). Based on the above data, we supposed that WM lesions in those regions may be responsible for motor deficits previously tested (Bolmont et al., 2000; Hornbein et al., 1989; West, 1984). In the present study, no significant changes in working memory and reaction time were tested after mountain climbing, which may be due to the practice effect because the same tasks were tested again during a short time interval.
In summary, using two recently developed MRI data analyses, we found single mountain climbing mainly impaired the WM but not GM. Moreover, the impairment existed in the microstructural integrity of WM tracts rather than the WM volume. Our present results suggest cytotoxic edema is present in HA cerebral edema. We did not observe cognitive changes in the verbal and spatial memory and the visuomotor implicit procedural learning. The decreases in WM FA values in several brain regions may clarify the mechanisms involved in some cognitive and motor deficits that previously tested. Future research is needed to clarify whether WM lesions would have recovered to normal after return to sea level for a long period of time.
Footnotes
Acknowledgments
This work was funded by National Science Foundation of China (Project No. 31071041).
Disclosure Statement
No competing financial interests exist.