
Abstract
Abstract
Basu, Minakshi, Anand Swarup Malhotra, Karan Pal, Tirthankar Chatterjee, Dishari Ghosh, Kaushik Haldar, Saroj Kumar Verma, Sanjeev Kumar, Yogendra Kumar Sharma, and Ramesh Chand Sawhney. Determination of bone mass using multisite quantitative ultrasound and biochemical markers of bone turnover during residency at extreme altitude: A longitudinal study. High Alt Med Biol 14:150–154, 2013.—A group of 221 male healthy volunteers of Indian Army were the subjects of the study. The baseline parameters of skeletal health were measured during their residency at an altitude of 3542 m. These subjects were then taken to an extreme altitude (EA, 5400–6700 m) where they stayed for about 4 months. The study parameters were repeated following their de-induction (DI) to 3542 m. On random selection, a subgroup was constituted from the above mentioned volunteers for detailed investigations on various bone turnover markers. Results of this study indicate a loss of body weight after DI from EA. The bone impairment was detected at the proximal phalanx, which is known to undergo early morpho-structural changes associated with bone resorption. The intact parathyroid hormone (i-PTH) levels showed a significant increase, while alkaline phosphatase (ALP) and bone specific alkaline phosphatase (BAP) activities declined significantly after DI from EA. This elevation in i-PTH might be required for maintenance of blood Ca level. 25 (OH) Vitamin D3 (25VitD) and calcitonin (CT) also showed a significant decline, which may suggest a negative impact on bone formation during sojourn at EA. The causes of deterioration of skeletal health at EA although are poorly understood but may be due to acute hypoxemia arising from extreme hypobaric hypoxia prevalent at extreme altitude.
Introduction
The adaptive processes to hypoxia imply complex alterations in the homeostatic steady state of several functions (Michiels et al., 2004). On the hormonal front, hypoxic stress stimulates secretion of many hormones such as thyroid hormones (Basu et al., 1995; Mordes et al, 1983; Rastogi et al., 1977), cortisol and catecholamines (Basu et al., 2002a, 2002b; Mazzeo et al., 1991), growth hormones (Sawhney et al., 1991), and erythropoietin (Basu et al., 2007; Milledge and Coats, 1985). These hormones are closely related to metabolic adaptation to oxygen deprivation and may have profound effects on bone mineral metabolism in man staying under hypoxic environments for prolonged duration. Increased secretion of glucocorticoids is known to inhibit bone growth and fracture healing, and cause osteoporosis by inhibiting osteoblast proliferation and function. Glucocorticoids can also cause a negative calcium balance by inhibiting intestinal calcium absorption and increasing renal calcium excretion (Baylink, 1983; Chyun et al., 1984; Reid, 1989). Similarly, increased secretion of thyroid hormones is known to stimulate bone resorption more than formation, which in turn may cause reduction in bone mass (Basset et al., 2007; Mundy et al., 1976).
Based on the foregoing information, we carried out a longitudinal study to investigate skeletal health of human volunteers during exposure to hypobaric hypoxia prevailing at EA in an ideal regimental practice of nutritional food intake and physical exercise. To the best of our knowledge, the current study is the first of its kind to investigate and find relationships among the skeletal health, dietary Ca intake, biochemical and endocrine indicators of bone mineral metabolism during pre-induction (PI) to and after de-induction (DI) from EA.
Methods and Materials
Volunteers
Two hundred and twenty-one male volunteers (21–47 years old) of mixed Indian ethnic population participated in the study. All the subjects were healthy controls with no obvious signs and symptoms of metabolic bone disease or any other illness, and were not taking any supplement affecting bone mineral metabolism. The study protocol was approved by the Institute's Ethics Committee. The experimental procedure was explained to all the subjects prior to experimentation and written consent was obtained.
Before initiating the study, all the subjects were asked about the personal data, exercise protocol, history of familial osteoporosis, medication history, any occurrence of stress fracture, and tenure at high to extreme altitude. The dietary intake of calcium was estimated by recalling the diet consumed by the individual during the last one week. The calcium intake was calculated using the published food composition table detailing the nutritive value of Indian foods (Pasricha et al., 1989).
All the subjects were sea level residents staying at an altitude of 3000–3754 m for the last 3–6 months. After recording their baseline parameters at 3542 m, these subjects were then deployed at an altitude of 5400–6700 m for 4 months. Under the field conditions of EA, almost 80% of the subjects operated in different terrains and performed various strenuous duties such as clearing snow, maintaining vigil in the defensive positions, carrying rations from one altitude to another, long distance route marches, and loading and unloading of materials.
Physical measurement
The physical data were obtained with minimum clothing and without shoes. Height (cm), body weight (BW) (kg), and body mass index (BMI) (kg/m2) were measured of all the subjects before induction and after their de-induction from EA using a “Seca” electronic human weighing balance (Model, Seca 767, SecaGmBh, sensitivity 100 g).
Speed of sound measurement
The Sunlight Omnisense (Omnisense, Sunlight Ltd, Tel-Aviv, Israel) a quantitative ultrasound system with the ability to perform speed of sound (SOS) measurements at multiple skeletal sites with hand-held probes designed for specific sites was used to measure SOS and Z-scores. The equipment has facility for correction of soft tissue thickness, giving a true SOS measurement of bone (Sunlight Omnisense User Manual 1998, Njeh et al., 1999).
SOS measurements were performed at one-third of distal radius (R), the proximal third phalanx (P) of the nondominant hand, the fifth metatarsal (M), and the mid-shaft tibia (T). The bone SOS, together with T-score and Z-score values were recorded. Assessment of T-score and Z-scores was compared with a reference Caucasian population. WHO has defined the standard criteria for determining bone (health) status. The criteria are defined as “the T-score” and “Z-score” between −1 to −2.5 termed as “osteopenia” and less than −2.5 termed as “osteoporosis”.
Biochemical markers and hormone levels
A subgroup of the above mentioned subjects selected randomly was investigated in detail for various bone turnover markers. Fasting blood sample was drawn from each subject in the morning between 0730 and 0830 h. Whole blood was centrifuged at 2000 g for 15 min at room temperature to obtain the serum which was stored at −80°C. Serum level of calcium (Ca), phosphorous (Pi), and alkaline phosphatase (ALP) were estimated within 6 hours of collection of blood samples, using commercially available kits obtained from M/S Randox, UK. Urinary Creatinine (Cr) was estimated by the alkaline picrate method (Bartels et al., 1972).
The intact parathyroid hormone (i-PTH) was estimated using enzyme-linked immunoassays (ELISA) kits obtained from DRG International, USA. 25-Hydroxy vitamin D3 (25Vit D) and calcitonin (CT) were estimated by radioimmunoassay (RIA) using kits obtained from M/S Bioline, Belgium. Serum bone specific alkaline phosphatase (BAP) was estimated using Ostase immunoradiometric assay kits obtained from Immunotech, France. Urinary DPD was measured by RIA using kits from M/S Immunodiagnostic System Ltd, USA.
Statistical analysis
Paired t-test was used to compare PI with DI for all the age groups. P values less than 0.05 was considered significant.
Results
Anthropometric parameters and general characteristics
The BW and BMI showed significant decrease after DI from EA as compared to PI values (Figs. 1 and 2). This decline in BW and BMI was more marked in subjects of the lower age group as compared to the higher age group. At PI, 14% of the subjects were smokers, whereas after DI the percentage of smokers decreased to 7%. Similarly, at PI, 26% of the subjects consumed moderate alcohol and after DI only 5% of the subjects were found to consume moderate alcohol. The 95th percentile values of dietatary calcium intake in this population during PI was 798.8 mg/day and after DI from EA was 645.0 mg/day.

Body weight (Mean+SEM) changes in subjects of different age groups during residency at extreme altitude.
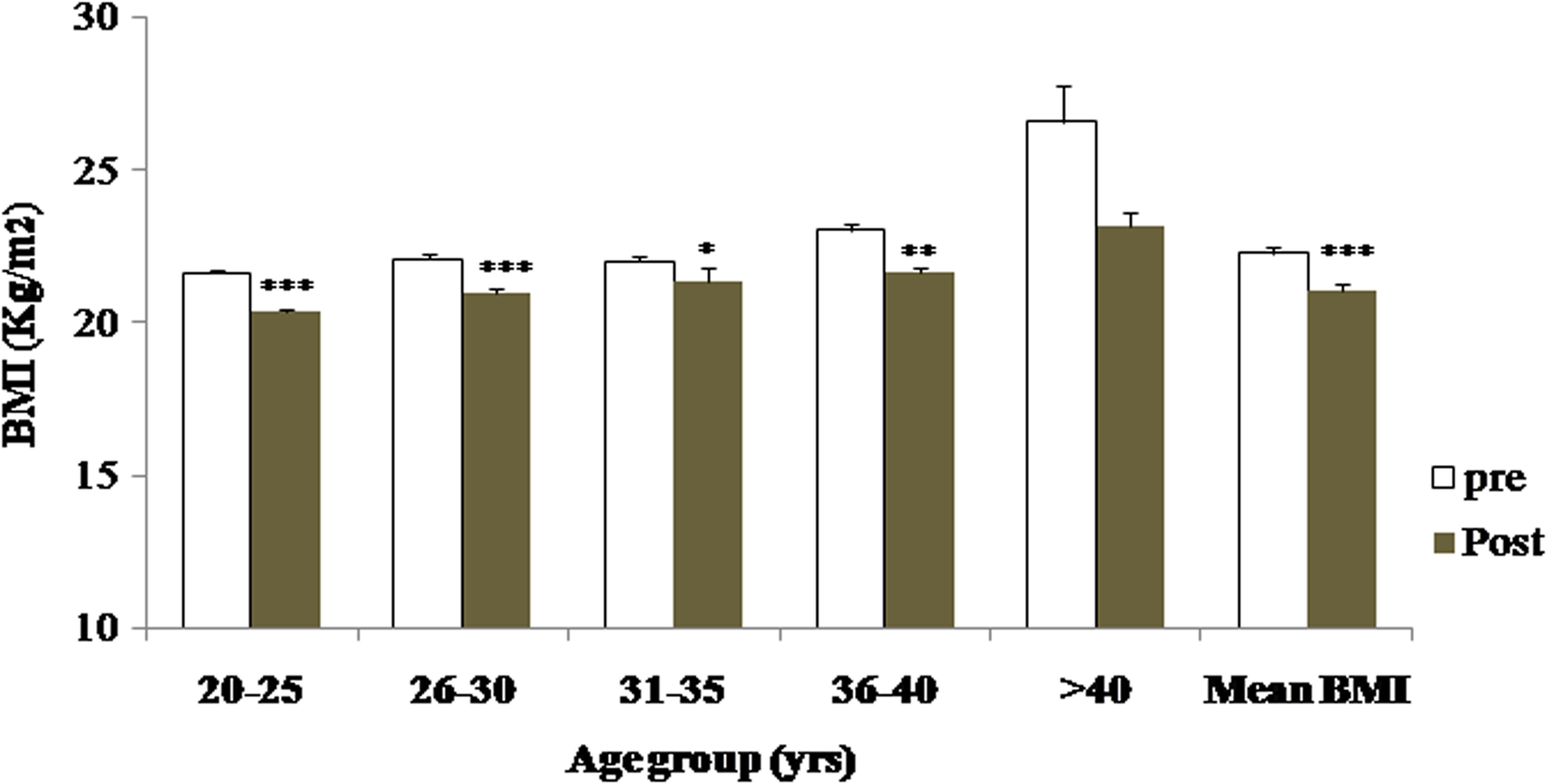
BMI (Mean+SEM) changes after 4 months of residency at extreme altitude.
SOS and Z-score measurements
The SOS and Z-score values of radius and tibia did not show any significant change in all the age groups, but metatarsal SOS and Z-scores showed significant changes only at lower age groups after DI from EA (Table 1). However, the phalanx SOS and Z-score values in all the age groups were significantly decreased after DI from EA. This decline in phalanx SOS and Z-score values was more significant in the younger age group as compared to the higher age group (>40 years). When phalanx SOS and Z-scores were computed for all the subjects as a group (n=221), the bone strength parameters showed a significant decrease (Table 2). After deinduction from extreme altitude, 62% of the subjects could be classified as having osteopenia and 2.8% showed osteoporosis.
P=PI Vs DI; *0.05, **<0.01, ***<0.001
P=PI Vs DI; *<0.05, **<0.01, ***<.0001
Biochemical and hormonal parameters
Serum calcium did not show any significant change but Pi was significantly increased after deinduction from extreme altitude (Table 3). However, serum Ca and phosphorous levels during PI and after DI are within the normal range. Significant decline of both ALP and BAP was recorded after DI from EA. Serum 25Vit D and CT showed a significant decrease whereas i-PTH showed a rise from 37.5 to 48.5pg/mL, but serum DPD/Cr ratio did not show any significant change after deinduction from EA (Table 3).
P=PI Vs DI; *<0.05, **<0.01, ***<0.001
Discussion
The results from the present unique study with maximal exposure to EA demonstrate that BW and BMI are significantly decreased almost in all the age groups after DI from EA. This decline in BW and BMI may be due to decreased or inadequate food intake as a result of hypoxia-related anorexia and satiety (Hamad and Travis 2006; Selvamurthy and Singh, 2003; Westerterp and Kayser. 2006) during prolonged residency under extreme altitude environment.
After 4 months of stay at EA, the most affected peripheral bone was phalanx, which is known to undergo early morpho-structural changes associated with bone resorption because of its high trabecular compound contents (Cadossi and Cane, 1996; Ekman et al., 2001, Kleerekoper et al. 1994). The third distal radius and third proximal phalanx are the sites clinically proven to predict fracture risk. Measurement at the phalanx, when combined with measurement from the radius, is particularly useful since differences in cortical thickness at the two sites provide more information, creating a more comprehensive picture of bone health (Barkmann et al., 2000; Knapp et al., 2001; Weiss et al., 2000).
Changes in skeletal health at EA are coupled with specific endocrine adaptations. Serum 25 VitD, CT, ALP and BAP showed significant decline, whereas i-PTH showed a significant rise, indicating that tenure/residency at EA causes changes in bone turnover parameters, which in turn may affect the bone health. Although carboxy-terminal collagen crosslink (CTX) is the most specific bone resorption marker, its estimation could not be carried out as sufficient volume of serum sample was not available. However, urinary estimation of DPD was carried out, which also represents the bone resorption marker. Urinary DPD/CR ratio did not show any significant change after DI from EA. The increased i-PTH might be required to increase conversion of 25(OH) D to 1,25(OH)2D to stimulate intestinal absorption of Ca. In addition, PTH also aids in the production of bone destroying osteoclasts and consequently speeds up the bone remodeling and release of Ca and other minerals in usable form (Bingham et al,. 1969, Raisz et al., 1990). ALP and BAP are pivotal part of bone growth and development in producing an alkaline environment and allowing calcium to crystallize and finally to achieve their strength. Though after 4 months of stay at EA, the change of bone mass occurred only in proximal phalanx, decline in ALP, BAP, and CT indicate activation of bone resorption process at extreme altitude in man.
The findings of this study must be considered in the context of several limitations. First, during the last 2 decades, dual-energy X-ray absorptiometry (DXA) has been used extensively, and has been accepted as a gold standard. But for HA and EA studies, a device which is multisite, portable, light, relatively rapid was required, so use of DXA was not possible. Second, volunteers in this study were all presumably healthier than the general population. Moreover, assessment of SOS in Indian men by comparing them with reference Caucasion population may have limited validity, primarily because of the influence of skeletal size on such measurements. Locally derived reference values are important to avoid false-positive or false-negative findings.
Conclusion
These observations suggest that residency under hypoxic environment at extreme altitude is associated with significant changes in hormonal, biochemical, and morphological indicators of bone remodeling parameters. Although the radius and tibia SOS and Z-scores did not show any significant change, the phalanx bone strength parameters were significantly decreased at extreme altitude. The causes of deterioration in skeletal health at EA are poorly understood, but climatic variables as well as dietary factors might be playing important roles.
Footnotes
Acknowledgments
The study was funded through Project No RD-P1-DIP-246 from Defence Research and Development Organisation (DRDO), Ministry of Defence, Government of India. The authors express their sincere gratitude to Dr. SB Singh, Director, DIPAS for her guidance and support. We also thank Dr. Kshipra Misra, Sc F and Dr. S.N.Singh, Sc E for their support.
The data collected under the present study are from soldiers working at extreme altitude with its toughest environmental vagaries and was only possible due to their sincere participation. We also thank all the commanding officers and other ranks of respective army units for their whole hearted cooperation and logistic support.
Author Disclosure Statement
No competing financial interests exist.