
Abstract
Abstract
Pavelescu, Adriana, Vitalie Faoro, Herve Guenard, Claire de Bisschop, Jean-Benoit Martinot, Christian Melot, Robert Naeije. Pulmonary vascular reserve and exercise capacity at sea level and at high altitude. High Alt. Med. Biol. 14:19–26, 2013.—It has been suggested that increased pulmonary vascular reserve, as defined by reduced pulmonary vascular resistance (PVR) and increased pulmonary transit of agitated contrast measured by echocardiography, might be associated with increased exercise capacity. Thus, at altitude, where PVR is increased because of hypoxic vasoconstriction, a reduced pulmonary vascular reserve could contribute to reduced exercise capacity. Furthermore, a lower PVR could be associated with higher capillary blood volume and an increased lung diffusing capacity. We reviewed echocardiographic estimates of PVR and measurements of lung diffusing capacity for nitric oxide (DLNO) and for carbon monoxide (DLCO) at rest, and incremental cardiopulmonary exercise tests in 64 healthy subjects at sea level and during 4 different medical expeditions at altitudes around 5000 m. Altitude exposure was associated with a decrease in maximum oxygen uptake (V
Introduction
The measurement of lung diffusing capacity is usually done with CO as tracer gas. The Roughton and Forster equation states that 1/DLCO=1/Dm+1/θVc where Dm is the membrane component of the alveolo-capillary transfer of CO, θ the rate of combination of CO with blood, and Vc the capillary blood volume (Roughton and Forster, 1957). Provided θ for CO at the appropriate P
We therefore reviewed Doppler echocardiographic studies of the pulmonary circulation and measurements of lung diffusing capacity, as well cardiopulmonary exercise tests of 64 healthy subjects evaluated at sea level and subsequent exposure to high altitudes during four different expeditions. We tested the hypothesis that a low PVR could be related to pulmonary vascular distension and possibly also recruitment including the pulmonary capillaries, and that therefore both a low PVR and a high lung diffusing capacity would be related to exercise capacity. Altitude exposure-induced hypoxic pulmonary vasoconstriction would allow examination of the effects of increased PVR. This could lead to a decreased pulmonary vascular distension because of decreased resistive vessel compliance (Groepenhoff et al., 2012) or, alternatively, increased pulmonary vascular distension because of higher pulmonary capillary pressures (Maggiorini et al., 2001). We reasoned that it would also be of interest to examine the effects of associated changes in ventilatory responses expressed as ventilation (VE) at any given rate of carbon dioxide production (V
Materials and Methods
Study population
Sixty-four healthy European lowlanders, 33 men and 31 women, aged 20 to 61 years, mean 32 years, gave a written informed consent to the study, which was approved by the Ethical Committee of the Erasme University Hospital (Brussels), approval number P2010/164, reference Eudract/CCB B40620108839. All of them had an unremarkable previous medical history and normal clinical examination, chest X-ray film, and normal electrocardiogram. Only three of them were light smokers.
Experimental protocol
All the subjects underwent a clinical examination with measurements of blood pressure (BP), heart rate (HR), and trans-cutaneous ear pulse oximetry oxygen saturation (Sp
Echocardiography
The echocardiographic measurements were performed with a Vivid 7 ultrasound system at sea level and with its Vivid i portable version at altitude in Nepal and Peru (GE Ultrasound Horten Norway) or a Cypress Acusson portable ultrasound system (Siemens, Erlangen, Germany) in Ecuador and Bolivia. Recordings were stored on optical disks and analyzed by cardiologists experienced in echocardiography. Cardiac output (Q) was estimated from the left ventricular outflow tract cross-sectional area and pulsed-wave Doppler velocity-time integral (LVOTVTI), systolic Ppa (sPpa) was calculated from the maximum velocity of the continuous-Doppler tricuspid regurgitation jet (TRV), and mean Ppa (mPpa) from the acceleration time (AcT) of right ventricular outflow tract flow velocity as previously reported (Naeije et al., 2010). Mean Ppa was calculated from sPpa as mPpa=0.6×sPpa+2 (Naeije et al., 2010). All measurements were made in triplicate and results are presented as means. Total pulmonary vascular resistance (TPVR) was calculated as the ratio between mPpa and Q, and stroke volume (SV) as Q/HR. TPVR and SV were indexed to the body surface area (TPVRI, SVI). As hypoxic exposure does not increase left atrial pressure or wedged Ppa in normal subjects at rest (Maggiorini et al., 2001), TPVR was thought to provide a reasonable estimation of PVR. Therefore, PVR is used instead of TPVR in subsequent sections of this report.
Cardiopulmonary exercise test
Exercise capacity was estimated by a standard incremental cardiopulmonary exercise test (CPET) performed in an upright position on an electronically braked cycle ergometer (Monark, Ergomedic 818E, Vansbro, Sweden). The work rate was increased by 15–30 watts/min (according to previously known exercise capacity and predicted decrease by 35% at high altitude) so that the test would last 10–12 min until exhaustion. Maximal oxygen uptake (V
Lung diffusion measurements
DLNO and DLCO were measured in the sitting position with corrections for hemoglobin and inspired partial pressure of oxygen, using an automated device for calibrations, mixing of gases, and online calculations (Hyp'Air compact, Medisoft, Dinant, Belgium) as previously reported (Glenet S et al, 2007; de Bisschop C et al., 2012), with a breath holding time of 4 sec, concentrations of inspired gases 40 ppm of NO, 1600 ppm of CO, 8% of helium, and 19% of O2 in nitrogen, and first 0.8 L of expired gas discarded. Measurements were repeated two to three times, with the aim to obtain DLCO values within 5% and DLNO values within 10% of each other. The coefficient relating DLNO and Dm was set at 1.97 according to the solubility and molecular weights of both gases (Aguilaniu B et al., 2008). Assuming linearity between 1/θCO and P
where Pcap
Statistical analysis
Continuous variables were presented as mean±SD after checking for normality of distributions. A univariate linear regression was performed to determine the significant variables associated with V
Results
Effects of altitude on clinical state, echocardiography (Table 1), CPET (Table 2), and lung diffusion (Table 3)
Altitude exposure was well tolerated, with transient mild degrees of headache, fatigue, weakness, dyspnea and lethargy, but, at time of the measurements, Lake Louise scores were at 4±1, corresponding to no or only mild acute mountain sickness. No subject felt that mild acute mountain sickness could have affected exercise capacity. There were a decrease in rest and end-exercise Sp
Values are mean±SD.
HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure, Sp
estimated from the right ventricle outflow acceleration time; **estimated from the tricuspid regurgitation jet velocity.
Values are mean±SD.
HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure, SpO2, pulse oximetry oxygen saturation, VO2max, maximum oxygen uptake; VE/VCO2 at AT, ventilatory equivalent for carbon dioxide at anaerobic threshold; VE/VCO2 max, ventilatory equivalent for carbon dioxide at maximum workload; VE/VO2 max, ventilatory equivalent for oxygen at maximum workload; VE, ventilation; RER, respiratory exchange ratio.
DLNO, lung diffusing capacity for nitric oxide; DLCO, lung diffusing capacity for carbon monoxide.
Altitude was associated with increased TRV and decreased AcT. Sufficient quality TRV signals could be obtained in only 58 of the 64 subjects, so that only AcT were used for the calculation of mPpa. There was no significant difference between the Ppa estimated by the two methods in the subjects in whom quality signals were available (Table 1). Maximal oxygen uptake, V
DLCO and DLNO were increased by 16% and 11%, respectively, so that DLNO/DLCO decreased by 4%. VA increased from 6±1.2 L at sea level to 6.5±1.2 L at high altitude (p<0.001).
Univariate and multivariable analysis of variables associated with Vo 2max
At sea level, the univariate analysis showed that V
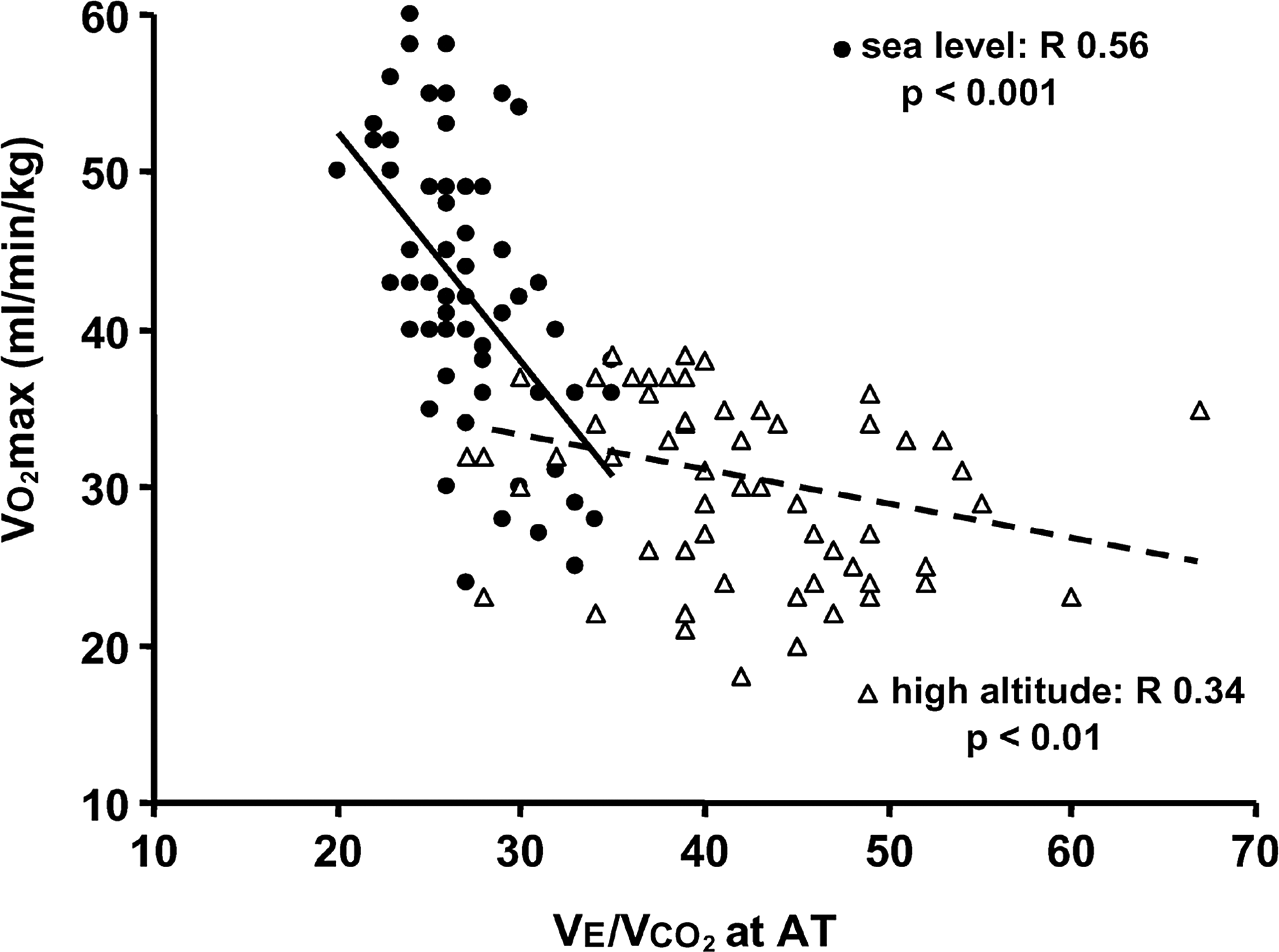
V

V
V
At sea level, the multivariable analysis showed that only lower VE/V
At high altitude, the univariate analysis showed that V
At high altitude, the multivariable analysis showed that only lower VE/V
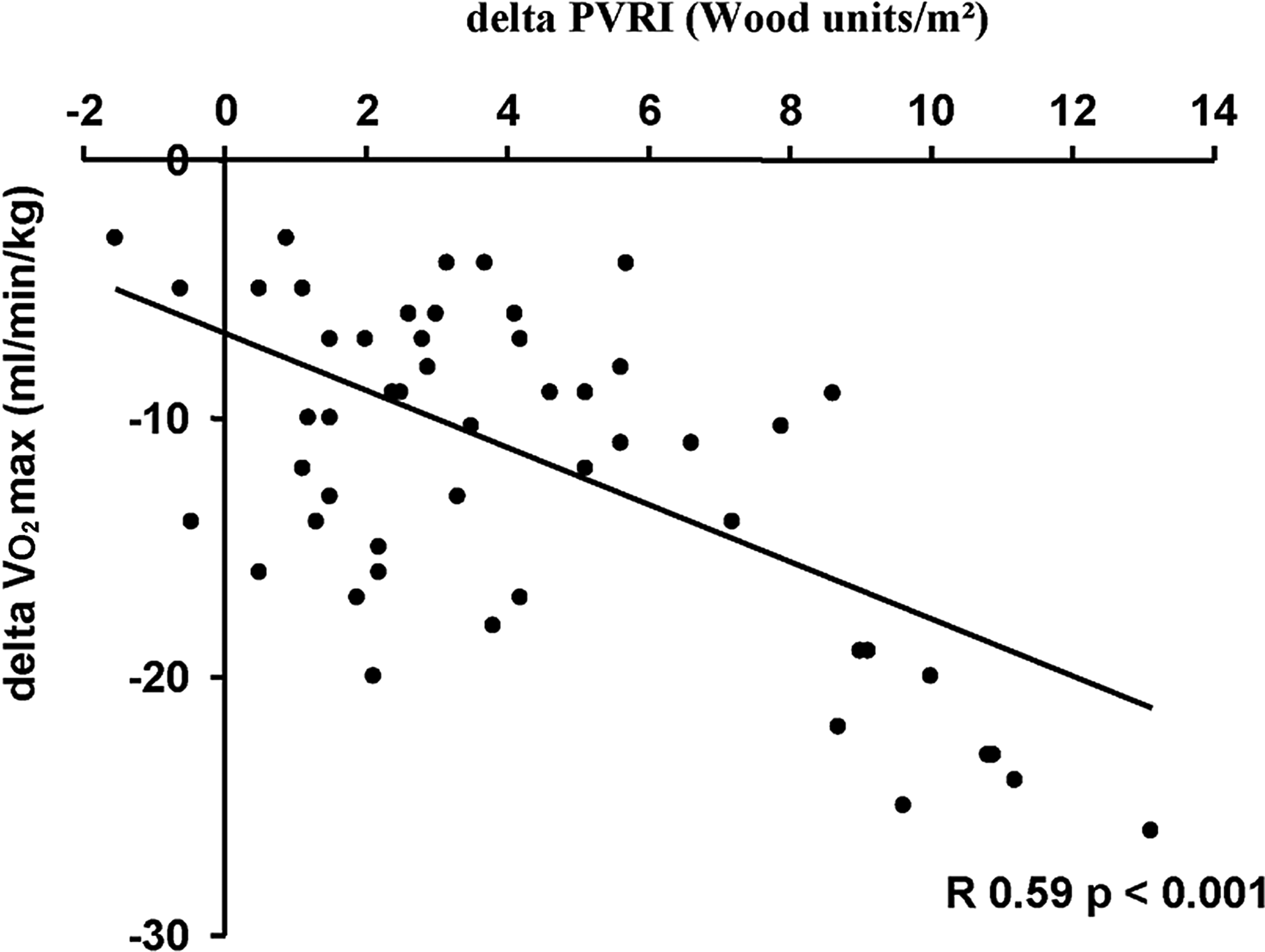
Change in V
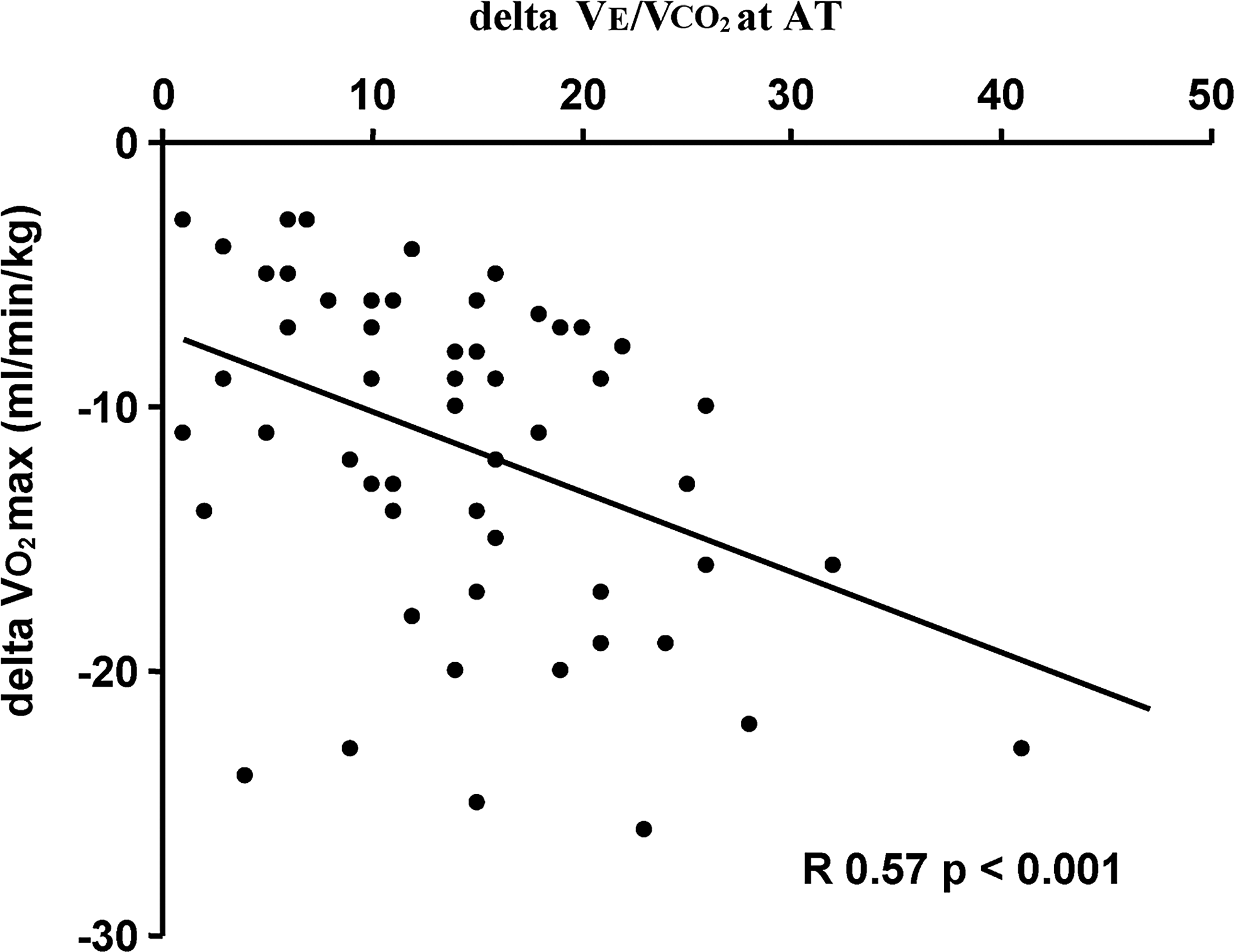
Change in V
Discussion
The present results show for the first time that in healthy subjects, V
In the present study, lung diffusing capacity was measured by the transfer of both NO and CO. The NO/CO transfer method was initially introduced with the rationale that the infinite affinity of NO for hemoglobin (θNO) would allow to calculate the membrane component of DLCO (Guenard et al., 1987). The Roughton and Forster equation states that 1/DLCO=1/Dm+1/θVc, where Dm and Vc are the membrane and capillary blood volume components of DLCO respectively (Roughton and Forster, 1957). With θVc equal to the infinite, a DLNO measurement would exclusively be determined by the membrane component of the alveolo-capillary gas transfer. Recent work has demonstrated that θNO has a finite value, introducing uncertainty about previously reported Dm and Vc calculations (Borland et al., 2012). Furthermore, the assumption of the linearity of 1/θ-P
The DLNO/DLCO ratio slightly decreased at high altitude, suggesting a predominant effect of increased Vc (Glenet et al, 2007, Hughes and Pride, 2012). This could be explained by capillary distension in addition to recruitment related to increased pulmonary prefusion pressure caused by hypoxic pulmonary vasoconstriction and, possibly, increased effective capillary pressure related to a venous component of hypoxic vasoconstriction (Maggiorini et al, 2001). However, the small size of the effect and the many assumptions on which the estimation is based make this result incompletely convincing. Furthermore, the DLNO/DLCO ratio did not change when DLCO was recalculated with P
During exercise at various intensities, DLCO and DLNO have been shown to increase in proportion to workload, with no change in the DLNO/DLCO ratio, which was stable at 4.52±0.24 (Zavorsky et al., 2004). In the present study, DLNO/DLCO was at the same mean value of 4.5 at sea level. Altitude exposure was associated with an increase in both DLNO and DLCO, confirming previous report in acclimatized subjects (Agostoni et al, 2011) or altitude exposure without strenuous exercise (Groepenhoff et al., 2012). However, the DLNO/DLCO, ratio slightly decreased. This is probably explained by capillary distension in addition to recruitment related to increased pulmonary perfusion pressure caused by hypoxic pulmonary vasoconstriction and, possibly, increased effective capillary pressure related to a venous component of hypoxic vasoconstriction (Maggiorini et al, 2001). However, DLNO/DLCO ratio did not change when DLCO was recalculated with sea level θ values.
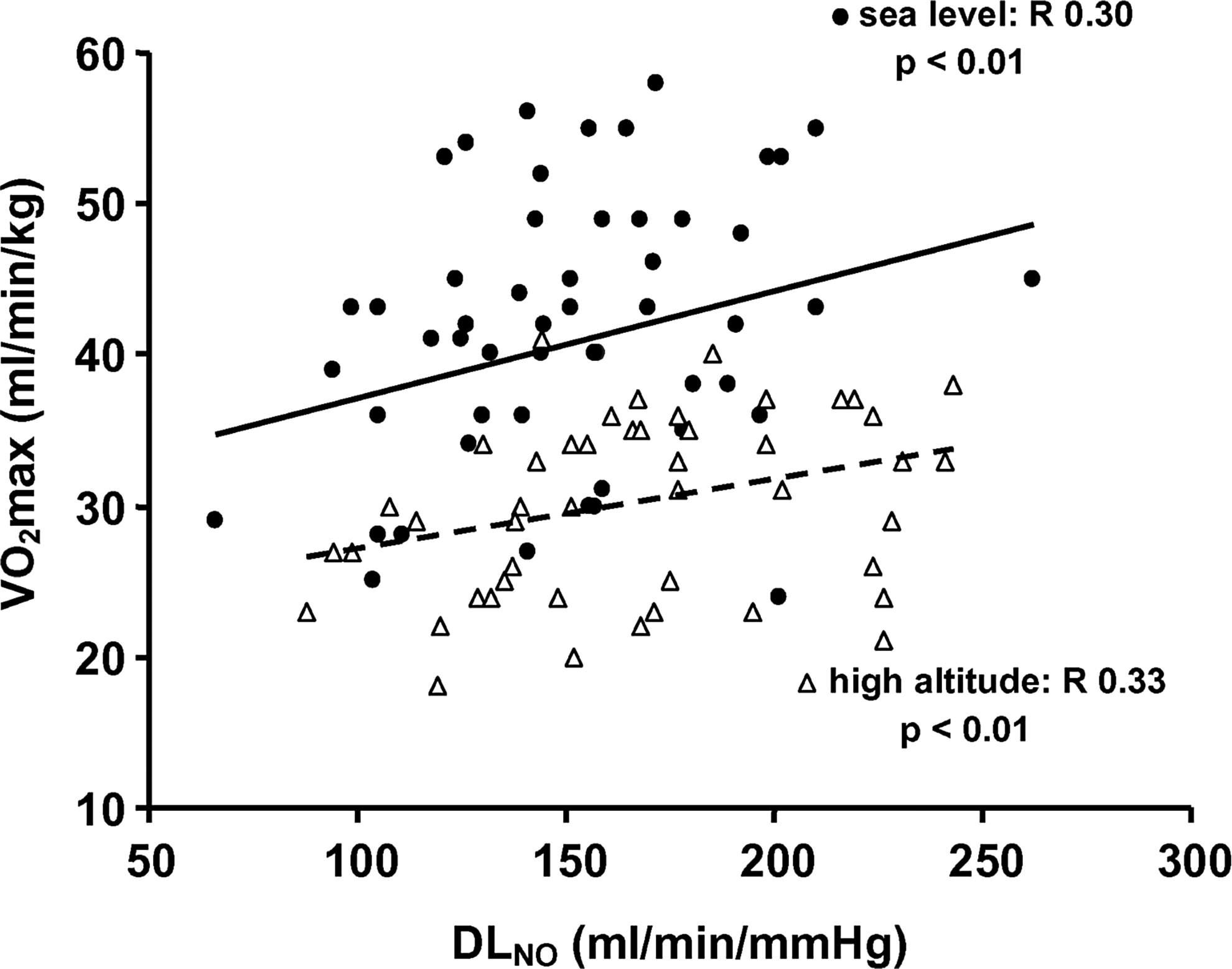
In the present study, a univariate analysis revealed that V
The observation of a lower PVR associated with a higher exercise capacity at altitude is in keeping with previous reports (Ghofrani et al., 2004; Faoro et al., 2009; Fischler et al., 2009; Naeije et al., 2010; Naeije, 2011). In the present study, a lower mPpa and a higher SVI were both independently associated with a higher V
Invasive, as well as more recent noninvasive studies, show that the response of the pulmonary circulation to exercise at progressively increased workload is characterized by variable slopes of mPpa-Q relationships, from 1 to 2.5 mmHg/L/min, with maximum mPpa between 40 and 50 mmHg at the highest flows (Reeves et al., 1999; La Gerche et al. 2010; Argiento et al., 2012, Lalande et al., 2012). There may be a maximum possible Ppa with which a healthy right ventricle can cope to maintain flow output adapted to peripheral demand, and this will be reached at higher maximal Q in subjects with lower PVR (La Gerche et al., 2010; Argiento et al., 2012). Positive pulmonary transit of agitated saline in healthy subjects at high levels of exercise and cardiac output probably reflects both arteriolar and capillary distension (La Gerche et al., 2010, Lalande et al., 2012). Another factor to consider is exercise-induced increase in left atrial pressure, which occurs at high levels of exercise (Stickland et al., 2006), and is transmitted upstream to mPpa in a close to one to one ratio (Reeves et al., 1999). This increase in left atrial pressure is delayed to higher levels of exercise in very fit subjects (Stickland et al., 2006) in relation to a decreased left ventricular diastolic compliance (Levine et al., 1991). The present demonstration that DLNO is associated with V
The combination of higher DLNO related to lower PVR being associated with higher aerobic exercise capacity was equally identified in normoxia and in hypoxia. Hypoxic pulmonary vasoconstriction in humans is usually mild and variable (Grover et al., 1983), but with a capillary-venous component (Maggiorini et al., 2001). This may explain why pulmonary vasodilating interventions decrease PVR and improve V
The effects of short-term altitude exposure on lung diffusing capacity has been reported variably (reviewed in de Bischop et al., 2011) but with a strong tendency to improvement when time is taken for optimal acclimatization (Agostoni et al., 2011). In the present study, altitude exposure was associated with moderate but significant increases in both DLNO and DLCO. Long-term to life-long exposure to high altitudes is associated with a marked increase in lung diffusing capacity, as well as with a decreased ventilatory response to exercise (Dempsey et al., 1971). It has been assumed that increased lung diffusion would be a favorable adaptation by allowing for maintained gas exchange at a lower level of ventilation (Dempsey et al., 1971). In the present study, VE/V
In conclusion, aerobic capacity at sea level, as well as at high altitude, tends to be higher in subjects with more pulmonary vascular reserve defined by a combination of lower pulmonary vascular resistance and higher lung diffusing capacity, along with a lower level of ventilation at any metabolic rate.
Footnotes
Acknowledgments
AP and RN drafted the report; AP performed part of the echocardiographic measurements, VF the CPET, and HG, CDB and JBM the lung diffusion measurements; CM advised and performed the statistical analysis; RN directed the expeditions, designed the studies, participated to the measurements, and is the guarantor of the paper, taking responsibility of the integrity of the work as a whole, from inception to published article. All the authors contributed to successive drafts of the report by comments and suggestions, and approved the final submitted version.
The authors thank S Huez, K Retailleau, R Bastin, M Moreels, M Mulè. and P Argiento for contribution to the echocardiographic examinations, M Lamotte, G Deboeck, M van der Plas, M Groepenhoff, S Beloka and M Overbeek for contribution to the CPET's, and C Scoditti, M Overbeek and G Leurquin-Stercq for contribution to lung diffusion measurements.
The expedition to Nepal was funded by the Ev-K2-CNR Project in collaboration with the Nepal Academy of Science and Technology as foreseen by the Memorandum of Understanding between Nepal and Italy, and thanks to contributions from the Italian National Research Council. The expeditions to Nepal and Peru were supported by grants from Pfizer. The expedition to Peru was made possible by the Instituto de Investigaciones de la Altura Universidad Peruana Cayetano Heredia, allowing for the use of the Cerro de Pasco Facilities. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author Disclosure Statement
No competing financial interests exist.