
Abstract
Abstract
Ke, Tao, Jiye Wang, Erik R. Swenson, Xiangnan Zhang, Yunlong Hu, Yaoming Chen, Mingchao Liu, Wenbin Zhang, Feng Zhao, Xuefeng Shen, Qun Yang, Jingyuan Chen, and Wenjing Luo. Effect of acetazolamide and gingko biloba on the human pulmonary vascular response to an acute altitude ascent. High Alt Med Biol 14:162–167, 2013.—Acetazolamide and gingko biloba are the two most investigated drugs for the prevention of acute mountain sickness (AMS). Evidence suggests that they may also reduce pulmonary artery systolic pressure (PASP). To investigate whether these two drugs for AMS prevention also reduce PASP with rapid airlift ascent to high altitude, a randomized controlled trial was conducted on 28 healthy young men with acetazolamide (125 mg bid), gingko biloba (120 mg bid), or placebo for 3 days prior to airlift ascent (397 m) and for the first 3 days at high altitude (3658 m). PASP, AMS, arterial oxygen saturation (Sa
Introduction
Acetazolamide and ginkgo biloba extract are two drugs that have been mostly investigated for prevention of acute mountain sickness (AMS). An inhibitory effect of acetazolamide on HPV was first observed as early as 1977 (Emery et al., 1977), but it was not confirmed until more comprehensive studies in isolated perfused lungs and live animals (Deem et al., 2000; Hohne et al., 2004). It was observed that both acetazolamide and ginkgo biloba extract could prevent early HAPE in rats (Berg, 2004; Berg et al., 2004). Further evidence showed that ginkgo biloba administration increased production of NO and decreased endothelin-1 and intracellular free Ca2+ of vascular endothelial cells (Ren et al., 2002; Wu et al., 2008), both of which were important mediators of pulmonary vasoconstriction. Although the two drugs hold promise for the prevention of pulmonary artery systolic pressure (PASP), there is no trial evaluating the effect of acetazolamide or ginkgo biloba extract on PASP in humans in the context of a quick ascent altitude exposure, such as travelers ascending rapidly from lowland elevations.
An acute exposure from low land to high altitude by air is an ideal protocol for the assessment of vascular responses to hypoxia, since the initial acclimatization time that may vary with different ascent profiles in other studies is well controlled. It also has direct clinical relevance for the many people nowadays who fly to high altitude regions for recreation or work. In the present study, we took advantage of an airlift ascent to evaluate the effect of acetazolamide and gingko biloba on PASP in a group of young men who were flown by airplane from Xi'an (397 m) to Lhasa (3658 m) in a randomized, double-blind and placebo-controlled clinical trial.
Methods
Participants
The trial was performed according to a prospective, double-blind, placebo-controlled design. Twenty-eight healthy lowland young men (17–22 years old) with no altitude experiences (>2500 m) in the preceding 2 years were enrolled into the trial on July 17–20, 2011. The highest altitudes they had ever climbed to were 1560 m to 2300 m, and none of them had ever been to the Tibet plateau. They were flown by a commercial airplane from Xi'an to Lhasa nonstop in 3 hours. All participants were fully aware of the study procedures and provided informed written consent. The Chinese Ethics Committee of Registering Clinical Trials (approval number, ChiECRCT-2011046) approved the study, which was conducted in accordance with the Declaration of Helsinki.
Treatment
The participants were randomized into three groups according to random numbers generated by using a software package (SPSS version 16.0, SPSS Inc, Chicago, Il), with nine in the acetazolamide group (125 mg bid), ten in the gingko biloba group (120 mg bid), and nine in the placebo group. Acetazolamide (Diamox; Wyeth Pharmaceuticals; USA), gingko biloba (Ginaton; Dr. Willmar Schwabe Pharmaceuticals; Germany), and placebo (provided by the Institute of Pharmaceuticals of the Fourth Military Medical University) were packaged in visually identical capsules at the Institute of Pharmaceuticals of the Fourth Military Medical University. Drug administration started 3 days before the ascent (in Xi'an, 397 m) and was continued for the first day in Lhasa (3658 m): a 3-day pretreatment and 1-day treatment duration. The compliance of each participant was followed and supervised by three investigators.
Outcomes
The primary outcome was PASP to hypoxia on the first day in the three groups. PASP on the second day and the third day were also observed as follow-up data. Secondary outcomes included AMS, arterial oxygen saturation (Sa
Statistical methods
PASP, Sa
Results
Baseline characteristics of the 28 participants are summarized in Table 1. The acetazolamide, ginkgo biloba, and placebo groups were well matched with no statistically significant differences in age, weight, height, and BMI. All subjects completed the treatment and follow up as planned.
One-way ANOVA, data are shown as means±SD.
Sa
FEV1%, forced expiratory volume in one second/forced vital capacity; FVC, forced vital capacity, liters; HR, heart rate, beats/minute; LLS, Lake Louise score; MAP, mean arterial pressure, mm Hg; PEF, peak expiratory flow, liters/minute. SaO2%, arterial oxygen saturation. Data are shown as mean and 95% CI.
p<0.05, †p<0.01: Paired Samples t Test, comparing the measurement at 3658 m with the measurement at 397 m; ‡p<0.05, one-way ANOVA with Bonferroni multi-comparison test, comparing acetazolamide or ginkgo biloba with the placebo group. §Data are shown as median and range.
The data of PASP of the four observational days are shown in Figure 1. PASP in the three arms at 397 m were not significantly different (range, 15–25 mm Hg), but they were all increased on the first day after ascending from 397 m to 3658 m (p<0.01). PASP in the acetazolamide group (mean at 3658 m, 26.2 mm Hg) was significantly lower than that in the ginkgo biloba group (mean at 3658 m, 33.7 mm Hg, p=0.001) and the placebo group (mean at 3658m, 34.7 mm Hg, p<0.001). The incremental change in PASP in the acetazolamide group was 4.7 mm Hg (95% CI., 2.6–6.9 mm Hg), which was much lower than that in the ginkgo biloba group (13.1 mm Hg, 95% CI., 9.6–16.5 mm Hg, p=0.002) and the placebo group (14.4 mm Hg, 95% CI., 8.8–20.0 mm Hg, p=0.001). In the mixed linear model, the mean PASP of the 4 observational days in the acetazolamide group (25.7 mm Hg) was lower than that in the placebo group (29.5 mm Hg, p=0.009, multiple comparison using Bonferroni correction). After including Sa

Pulmonary artery systemic pressure (PASP) of the three groups (acetazolamide, ginkgo biloba, and placebo) at 397 m and on the first 3 days at 3658 m. The individual data of PASP in the three groups were plotted. PASP was estimated from the maximum velocity of continuous Doppler tricuspid regurgitation with an estimated value of 5 mm Hg of right atrium pressure (RAP). Bar represents mean PASP.
Arterial oxygen saturation (Sa
During the trial, no subject experienced disorientation or incapacitating fatigue as assessed by clinical assessment of LLS, and no case of HAPE or high altitude cerebral edema (HACE) was diagnosed in any group. Adverse reactions in AZ group were limited to one subject with polyuria, and three subjects with numbness and tingling of the fingers and toes. There were no reported adverse reactions in either the gingko biloba or placebo groups, beyond the typical symptoms of AMS.
Discussion
The main finding of our trial was that a 3-day pretreatment with acetazolamide at a dosage of 125 mg bid and a further day of administration at high altitude can effectively reduce altitude-related pulmonary hypertension in young male adults. A similar prophylactic effect was not found for gingko biloba, despite published animal work suggesting a possible utility (Ren et al., 2002; Berg, 2004; Wu et al., 2008). Acetazolamide was also able to reduce severity of AMS in an airlift ascent altitude exposure profile, which gives further support for the use of a lower dose of acetazolamide for the prevention of AMS as shown by others (Basnyat et al., 2003; 2006; Tissot van Patot et al., 2008).
The effect of acetazolamide on the pulmonary vasculature has received much attention for its use not only in preventing AMS, but possibly in preventing HAPE. A recent human study using the dynamic end-tidal forcing technique showed that 750 mg/day of acetazolamide (250 mg tid started 1 day before an acute normobaric hypoxic exposure) was effective in inhibiting pulmonary vascular resistance (Teppema et al., 2007) with 12% O2, but the result was obtained in a simulated altitude. Basynat et al. (2008) found that acetazolamide fails to decrease PASP at high altitude in already partially acclimatized humans. It was reasoned that the dosage of 500 mg acetazolamide, which was effective in preventing AMS, was insufficient to alter hypoxic pulmonary pressure (PASP) after partial or full altitude acclimatization, similar to the findings by Faoro et al. (2007) after 2 weeks at high altitude in Bolivia. However, we show by using an airlift altitude exposure to minimize the confounding effect of partial or complete acclimatization, that 125 mg bid acetazolamide is effective in reducing PASP, as well as preventing AMS.
As far as we know, this is the first trial to test the efficacy of low-dose acetazolamide and gingko biloba on PASP at altitude. The strength of the present study was that acclimatization time was well controlled in an airlift ascent profile. As quick ascent rate is a risk factor for HAPE (Basnyat and Murdoch, 2003), the airlift model used in the present study may well reflect the real context under which many persons may use drug prophylaxis for quick ascent. The increase in PASP on the first day was reduced by acetazolamide, and the effect persisted on the following 2 days. Although the duration of the pharmacologic effect of a single administration of acetazolamide usually exceeds its serum half-life (6–8 h) (Moviat et al., 2006), the carryover effect of acetazolamide on the PASP at altitude was apparently diminishing and likely would have been sustained had the subjects continued to take acetazolamide.
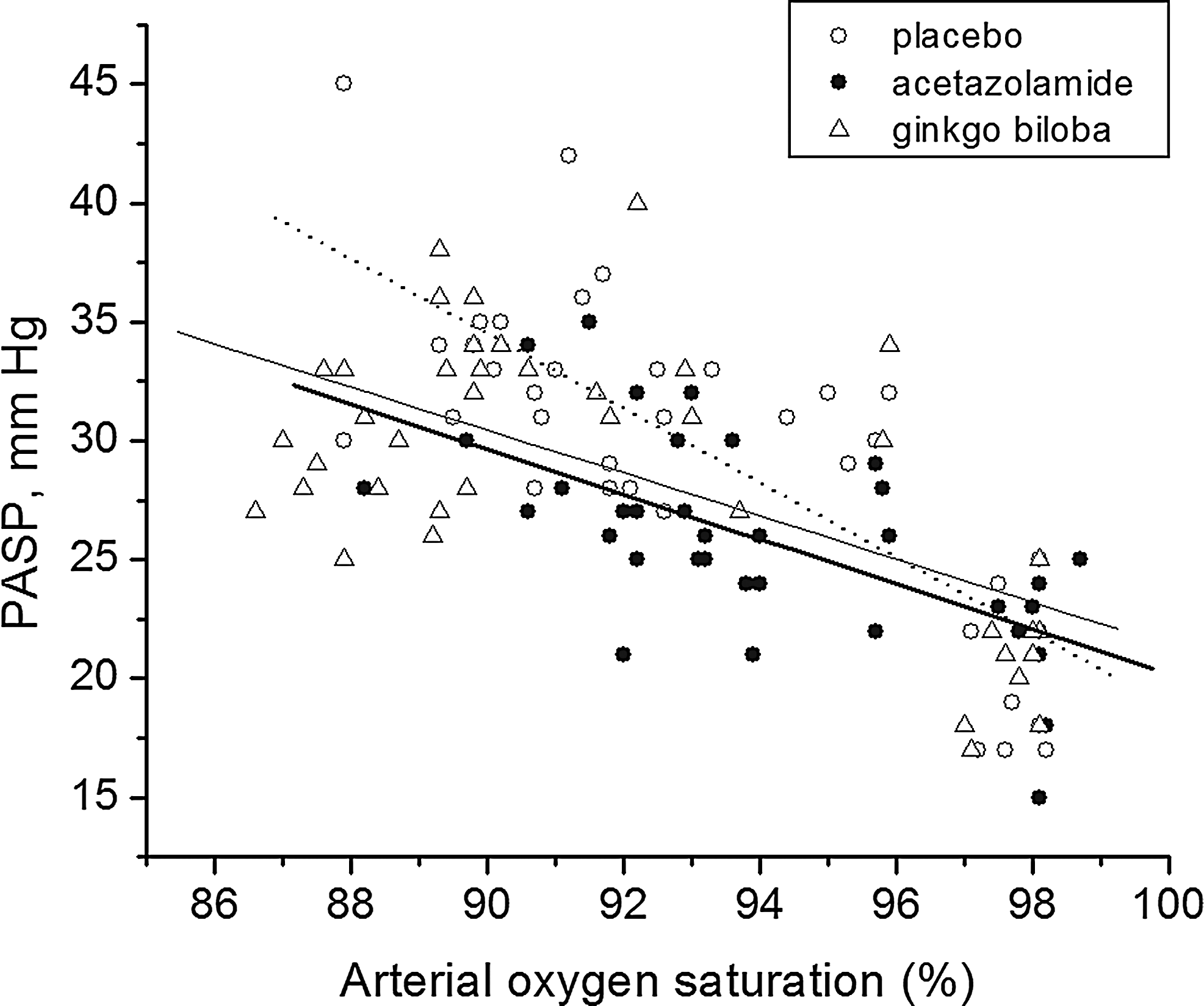
Although the relation of change with altitude of PASP to Sa
Because increased PAP is considered a key causal factor in HAPE, the present study has significance for the future evaluation of the effect of this lower dose of acetazolamide on HAPE prevention in HAPE-susceptible subjects. As treatment of chronic mountain sickness by acetazolamide is recommended (Richalet et al., 2005), it will be worth testing the effect of acetazolamide on chronic hypoxic pulmonary hypertension, as well as on the amelioration of polycythemia in chronic mountain sickness cases. Although the current study holds promise for a lower dose of acetazolamide in preventing HAPE, future studies of larger samples including both males and females are warranted. The minor but significant effect of acetazolamide on PASP that may be more prominent in higher risk ascent or in exercise and hypoxia needs further investigations.
In summary, our data suggest that a low dosage of acetazolamide (125 mg bid for several days before altitude ascent), but not gingko biloba, can mitigate early increase of PASP in a situation of rapid ascent to high altitude.
Footnotes
Acknowledgments
The authors thank Bin Wang, Dali Xi, Shenming Zhang, and Pengchong Cao for the help during the physical measurement in Lhasa, and Ruian Wang for providing medical support during the trial. Special thanks to the research participants who generously contributed with their time and energy during the trial.
Author Disclosure Statement
No authors have conflicts of interest.
This work was supported by the National Key Technology R&D Program (Grant 2009BAI85B04); National Nature Science Foundation of China (Grant 81172621); and Program for Changjiang Scholars and Innovative Research Team in University (PCSIRT, IRT1112).