
Abstract
Abstract
Cushing, Tracy, Ryan Paterson, Jason Haukoos, and N. Stuart Harris. Intraocular pressure is not associated with acute mountain sickness. High Alt Med Biol 14:342–345, 2013.—
Introduction
A
At present, the diagnosis of AMS remains dependent on subjective patient reporting of symptoms and on nonspecific clinical findings (Hackett and Roach, 2001; Roach et al., 1993). Studies have investigated portable, objective diagnostic tools to diagnose patients with AMS in the field using scoring systems, ultrasound measured optic nerve sheath diameter, and intraocular pressure (IOP) with varied success. (Cymerman et al., 2000; Ersanli et al., 2006; Fagenholz et al., 2009; Kayser et al., 2010) The presence of a simple, robust physiologic measurement to assist in the rapid diagnosis of AMS would be a great advance. Investigations of IOP as a marker for AMS are based on data demonstrating an association between IOP and elevated ICP. Some authors have hypothesized and demonstrated that IOP may correlate with increased intracranial pressure (Lashutka et al., 2004; Sajjadi et al., 2006), while other studies have shown no association between the two (Kirk et al., 2011; Muchnok et al., 2012).
IOP is a function of aqueous humor production and subsequent drainage via the trabecular meshwork. The modified Goldmann equation relates the variables that determine steady state IOP, including conventional and uveoscleral aqueous outflow rates, aqueous outflow facility, and episcleral venous pressure (EVP) (Sit et al., 2008). IOP is thus influenced by anything that increases production or decreases drainage of the aqueous humor including age, physical exertion, and medications, among other factors, and its measurement is affected by changes in corneal thickness, measuring device, and time of day (Cymerman et al., 2000; Doughty and Zaman, 2000; Ersanli et al., 2006; Kniestedt et al., 2006; Karadag et al., 2008; Wong et al., 2009).
Prior studies investigating the correlation between IOP and symptomatic AMS have been underpowered, small, and taken as a group, ultimately inconclusive as to the effect of altitude on IOP and the correlation between IOP and AMS. (Bayer et al., 2004; Bosch et al., 2010; Ersanli et al., 2006; Karadag et al., 2008; Karakucuk and Mirza, 2000; Somner et al., 2007). This study is a large, prospective, convenience sample of IOP in high altitude trekkers, which attempts to determine whether a correlation exists between IOP and symptoms of AMS.
Methods
Subjects were recruited from a convenience sample of trekkers in the Khumbu (Everest) region of Nepal, at an elevation 14,410 ft (4392 m). Subjects were excluded if they had a prior history of ocular surgery, glaucoma, were less than 18 years of age, or were unable to consent due to language barriers or due to altered mental status.
Study protocol
The study protocol was reviewed and approved by the Partners Human Research Committee (Boston, MA) and the Nepal Health Research Council (Kathmandu, Nepal). Upon enrollment in the study, participants were asked to complete a questionnaire yielding a Lake Louise score for AMS (LLS). The criterion of LLS ≥3 plus headache was used to define AMS. Subjects had their heart rate and oxygen saturation measured with a pulse oximeter (Devon Medical, PA, USA).
Upon completion of the questionnaire, each participant received three IOP measurements in each eye using an applanation tonometer (Tono-Pen XL® Reichart Technologies, NY, USA) with the patient in a supine, eye-neutral position after topical anesthetic (tetracaine ophthalmic 0.5%) was applied. Investigators measuring IOP were blinded to the subjects' LLS.
IOP measurements were averaged across both eyes within subjects. A multivariable logistic regression analysis was performed to determine the association between IOP and AMS while adjusting for age, ascent or descent, and use of acetazolamide. Correlation between IOP and O2 saturation was assessed using a Spearman correlation coefficient. Data were analyzed using Statistical Analysis System® (SAS®) software (SAS®, NC, USA).
Results
161 subjects were enrolled with a median age of 36 (IQR: 29–45) years. 60% of the subjects were male, 75% were ascending, and 64% were taking acetazolamide, dosages ranging from 125 mg QD to 375 mg BID. Overall, 38% of the study population (N=61) were diagnosed with AMS as defined by LLS ≥3 (95% CI: 31%–47%) (Table 1).
The median IOP was 21 (IQR 18–24) mmHg. Logistic regression models demonstrated no association between IOP and AMS (OR 1.0, 95% CI: 0.9–1.1) when controlling for age, ascent versus descent, and whether subjects were taking acetazolamide (Fig. 1).
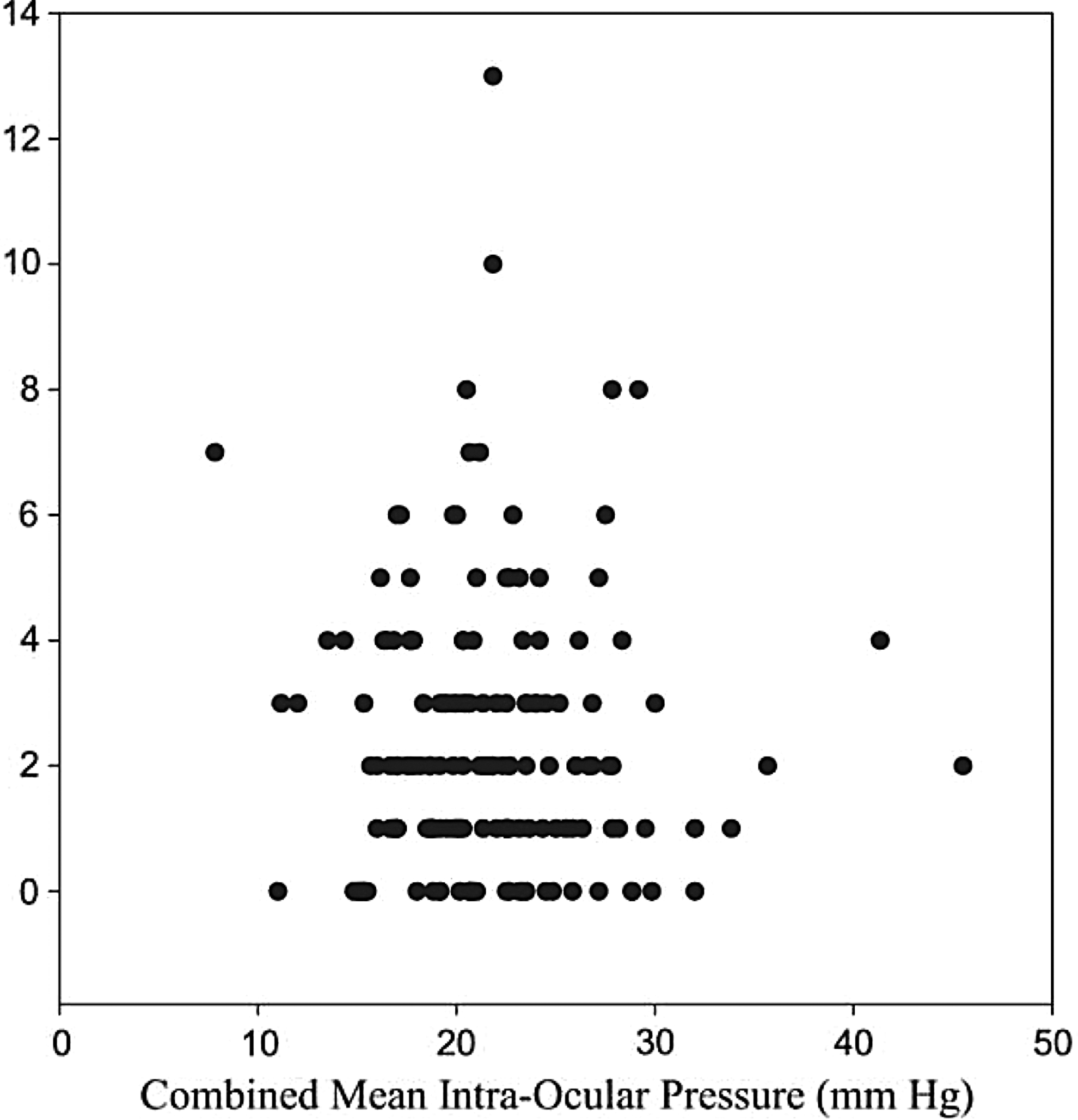
Combined mean intra-ocular pressure versus Lake Louise Score.
Age (OR 1.0, 95% CI: 0.9–1.0) and the use of acetazolamide (OR 1.4, 95% CI: 0.6–2.6) were also not associated with IOP, while ascent (OR 0.4, 95% CI: 0.2–0.9) was negatively associated with IOP when controlling for all other variables. Oxygen saturation as measured by peripheral pulse oximetry was not correlated with IOP (p=0.93).
Discussion
In this study, the largest assessment of IOP at high altitude yet published, there is no association between IOP and AMS (as defined by LLS), age, or acetazolamide use in trekkers to the Khumbu region of Nepal at an elevation 14,410 ft.
The incidence of AMS in our subjects (38%) is consistent with the incidence of AMS in multiple prior studies at this elevation. Despite this significant incidence of AMS, there is no association between IOP and AMS. This result is consistent with the current pathophysiologic explanations of AMS and IOP regulation, where significantly elevated ICP is required to elevate IOP. Given that ICP increases may not be associated with AMS, our results appear physiologically sound (Kaur et al., 2002; Natsis et al., 2009). Of note, none of the participants in this investigation were diagnosed with high altitude cerebral edema (HACE), which results in markedly elevated ICP (Hackett, 1999). It is thus doubtful that any of the participants had ICPs greater than 50 mmHg, which is the degree of ICP hypothesized to elevate IOP (Qureshi, 1995).
It has been demonstrated that ICP rises, transiently, with altitude exposure (Foster et al., 2011). Small, transient elevations in IOP have been reported upon exposure to hypobaric hypoxia, which then plateau and ultimately return to normal with acclimatization and prolonged exposure to altitude (Bosch et al., 2010; Somner et al., 2007) Similarly, the results of this study did show an elevated IOP under conditions of hypobaric hypoxia at 14,410 ft with a mean IOP of 21 mmHg (IQR 18–24 mmHg). When controlled for acetazolamide use, the data showed no effect of acetazolamide on IOP (Fig. 2). Given acetazolamide's role in the treatment of pathologically increased IOP (e.g., glaucoma) by decreasing aqueous fluid production, this finding remains unexpected (Kaur et al., 2002). This lack of association might be attributed to the relative youth and good ophthalmologic health of our study population (prior eye surgery or glaucoma were exclusion criteria).
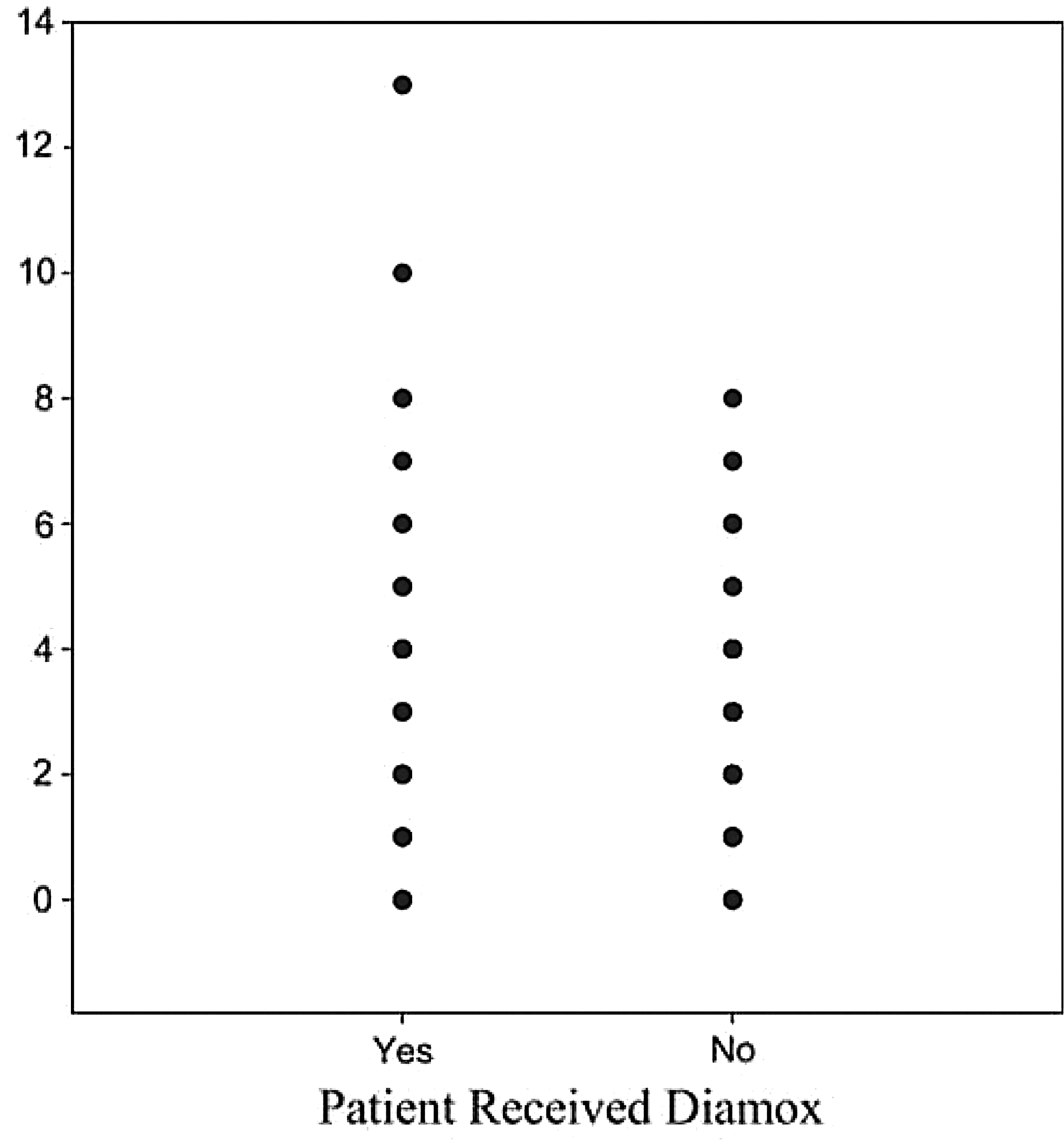
Diamox versus Lake Louise Score.
Unexpectedly, ascent was inversely associated with IOP, but not significantly so. As such, persons ascending had lower IOP measurements. This trend was present independent of acetazolamide use (a medication presumably more commonly used during ascent). Physical exertion is associated with decreased IOP and would presumably be more prevalent in those actively ascending, which may account for this trend towards lower IOP (Natsis et al., 2009; Qureshi, 1995).
Age was not associated with changes in IOP in this study. Normally IOP increases with age until the 6th or 7th decade, at which point it generally decreases. (Foster et al., 2011; Wong et al., 2009). Given our remote study location (multiple-days uphill walk at high altitude), it is not surprising that our study population tended towards a younger adult population (median age 36 years), with a narrow age range (IQR: 29–45 years). Pediatric subjects were excluded from participation. Given these unique features, our lack of association between age and IOP should not be considered generalizable.
Limitations
We report on a convenience sample at high altitude performed under austere conditions. There were no baseline or sea level measurements of IOP in the study participants, which does not allow for the evaluation of individual changes in IOP with exposure to altitude. In addition, subjects did not follow a standardized ascent protocol which might lead to variability in both AMS and IOP changes.
The diagnosis of AMS is based on the subjective reporting of physical symptoms, which is quantified by the LLS questionnaire (LLS-Q). Though subjective, LLS-Q is the preferred diagnostic tool for AMS and has been validated many times for use in research and in the field.
Central corneal thicknesses (CCT) were not measured in our study. It is known that CCT increases with exposure to the conditions at altitude secondary to corneal edema. Such increases can affect IOP measurements, usually leading to an underestimation of the IOP (Bosch et al., 2010; Czarnik et al., 2009; Tonnu et al., 2005). Thin CCT has been shown to artificially decrease IOP measurements in patients with glaucoma, and a meta-analysis of CCT and IOP showed that a 10% difference in CCT would result in a 3.4±0.9 mm Hg difference in IOP (p</=0.001, r=0.419) (Doughty and Zaman, 2000; Kniestedt et al., 2006). However, the same meta-analysis found that for “deemed healthy eyes,” the effect was smaller than in persons with diseased corneas (Doughty and Zaman, 2000).
IOP is also known to be affected by the time of day, with the highest values being found at night (Sit et al., 2008). This should not affect our study as all measurements were taken during the day.
Use of the Tono-Pen XL when compared to the gold standard (Goldmann tonometry) has been shown to differ by 0.6–1.0 mm Hg (Tonnu et al., 2005). Other methods of IOP measurement such as rebound, noncontact, and transpalpebral tonometry have shown similar intermethod agreement when compared to the gold standard (Cook et al., 2012) Overall, no field method has proven superior to another when compared to Goldmann.
Conclusions
This is a large, negative study demonstrating that IOP is not associated with, and appears to have little utility in, the diagnosis of AMS. Other approaches to easily and accurately diagnose AMS are needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.