
Abstract
Abstract
Foster, Gary P., Paresh C. Giri, Douglas M. Rogers, Sophia R. Larson, and James D. Anholm. Ischemic preconditioning improves oxygen saturation and attenuates hypoxic pulmonary vasoconstriction at high altitude. High Alt Med Biol. 15:155–161, 2014.—Exposure to hypoxic environments is associated with decreased arterial oxygen saturation and increased pulmonary artery pressures. Ischemic preconditioning of an extremity (IPC) is a procedure that stimulates vasoactive and inflammatory pathways that protect remote organ systems from ongoing or future ischemic injury. To test the effects of IPC on oxygen saturation and pulmonary artery pressures at high altitude, 12 healthy adult volunteers were evaluated in a randomized cross-over trial. IPC was administered utilizing a standardized protocol. IPC or placebo was administered daily for 5 days prior to ascent to altitude. All participants were evaluated twice at 4342 m altitude (placebo and IPC conditions separated by 4 weeks, randomized). The pulmonary artery systolic pressure (PASP) at 4342 m was significantly lower in the IPC condition than the placebo condition (36±6.0 mmHg vs. 38.1±7.6 mmHg, respectively, p=0.035). Oxygen saturation at 4342 m was significantly higher with IPC compared to placebo (80.3±8.7% vs. 75.3±9.6%, respectively, p=0.003). Prophylactic IPC treatment is associated with improved oxygen saturation and attenuation of the normal hypoxic increase in pulmonary artery pressures following ascent to high altitude.
Introduction
E
Ischemic preconditioning (IPC) is a procedure that has the effect of markedly attenuating ischemia reperfusion injury. The IPC procedure is performed by repetitive occlusion of arterial blood flow to an organ or extremity (e.g., 5 minutes occlusion, followed by 5 minutes of restored blood flow, repeated several times). The protective effects of IPC on local and remote tissues are largely attributed to effects on vasoactive and inflammatory pathways (Gho et al., 1996; Birnbaum et al., 1997; Kharbanda et al., 2002; Auchampach et al., 2004; Ali et al., 2007; Botker et al., 2010). The protective effects of IPC occur in two phases, early (lasting 2–3 hours) and late (returning at 12–24 hours and lasting 48–72 hours) (Murry et al., 1986; Marber et al., 1993).
The systemic or “remote” effects of IPC can be profound. As an example, IPC to one arm can dramatically reduce the size of a myocardial infarction, mitigate the incidence of arrhythmias, and improve recovery of myocardial contractility and vascular function in both animal models and human trials (Murry et al., 1986; Birnbaum et al., 1997; Auchampach et al., 2004; Botker et al., 2010). These effects also extend to the pulmonary vasculature, where our group demonstrated that the hypoxic increase in pulmonary artery systolic pressure during acute simulated altitude conditions is significantly attenuated IPC in humans (Foster et al., 2011).
The intent of the present study was to test the effects of the late phase of IPC on pulmonary artery pressures and Sp
Materials and Methods
Subjects
Fourteen healthy, nonacclimatized adults (42±14 years, twelve male and two female) habituated to strenuous exercise were enrolled. These subjects provided written informed consent for study participation, which was approved by the VA Loma Linda Healthcare System Institutional Review Board (IRB). The subjects had no medical conditions limiting exercise or known heart or lung disease. None of the subjects had a history of abnormal HPV response to high altitude exposure (such as high altitude pulmonary edema). Two of the subjects developed illnesses (one sprained ankle, one bronchitis) precluding completion of the protocol and were excluded from the study. The study protocol was completed in 12 of the initial study subjects (eleven male, one female). The subjects had a mean height 179.9±8.7 cm, a mean weight of 74.3±12.0 kg, and a mean BMI of 23.3±2.6 kg/m2.
Study design
Initial testing was performed at the VA Loma Linda Healthcare System facility in Loma Linda, CA (altitude 370 meters, ambient Pb ∼727 mmHg, PI
Ischemic preconditioning
Ischemic preconditioning (IPC) was completed by placing a blood pressure thigh cuff (Tycos, hand held aneroid sphygmomanometer 5098-03 and Welch-Allyn durable two piece cuff 5098-02 cb, Skaneateles Falls, NY) around one thigh, inflating it to a pressure of ∼200 mmHg for 5 min, then deflating for 5 min of restored blood flow. This sequence was repeated for a total of four cycles over an elapsed time of 40 min [4×(5 min of arterial occlusion +5 min nonocclusion)=40 min]. IPC was administered daily for 5 days with the fifth IPC en-route to Barcroft laboratory, prior to ascent. The placebo condition was timed identical to the IPC condition with the blood pressure cuff inflated to only 40 mmHg.
Echocardiography
Echocardiography was performed with a portable ultrasound machine (Siemens, P50 ultrasound system, Siemens Medical Solutions USA Inc., Ultrasound Division, Mountain View, CA) using standard techniques. Echocardiographic data was recorded digitally and anonymized for analysis. The sonographers (and all study staff ) were blinded to the subject study condition (placebo or IPC) at the time of echocardiography and data analysis for all phases of the study. Two sonographers, blinded to subject condition, independently analyzed the echocardiographic data off-line. Spectral Doppler tracings were independently graded for quality and excluded if deemed not interpretable by either sonographer. Pulmonary artery systolic pressure (PASP) was calculated using the modified Bernoulli equation: (4V2)+5 mmHg, where V equals the peak end-expiratory tricuspid regurgitation velocity (TRV) by continuous wave spectral Doppler and 5 mmHg is the assumed right atrial pressure (Yock and Popp, 1984; Rudski et al., 2010). A minimum of three TRVs were averaged for each subject and each condition. As a means of providing external validation of the PASP findings, the mean pulmonary artery pressure (mPAP) was calculated using the empirically derived formula and methods described by Kitabatake et al. (1983), where the mPAP=10^ [−2.8 (AT/ET) +2.4]. AT equals systolic acceleration time across the main pulmonary artery measured by pulsed wave spectral Doppler and calculated from initiation to peak (sec) and ET is the right ventricular systolic ejection time measured utilizing the same Doppler wave, from initiation to end (sec). Cardiac output was calculated by assessment of the left ventricular outflow tract (LVOT), using the formula: cardiac output=πr2×VTI×heart rate, where VTI is the velocity-time integral of blood flow across the LVOT (Christie et al., 1987; Weyman, 1994).
Pulse oximetry
Pulse oximetry was measured and recorded continuously at Barcroft Lab (3800 meters) and the summit (4342 meters) throughout the course of echocardiography using a pulse oximeter (Masimo Corporation, RDS-1 Signal Extraction Pulse Oximeter, Irvine, CA) that was placed on the index finger or earlobe. Sp
Lake Louise Acute Mountain Sickness Score
The Lake Louise Scoring System (LLS) for Acute Mountain Sickness was used to assess symptoms of mountain sickness (Sutton and Houston, 1992). All subjects completed the questionnaire at the summit of White Mountain following exercise for both IPC and placebo conditions.
Exercise task
The study subjects performed a 12.8 km run from an altitude of 3560 m to 4342 m on two occasions (once for each testing condition), separated by at least 4 weeks. Heart rate was measured throughout the course using a chest mounted radio transmitted heart rate monitor (Polar Vantage NV, Polar Electro Inc., Lake Success, NY). Aid stations were provided at four locations along the course to provide water, nutrition, or other support to the study subjects.
Statistical analysis
Based on a randomized crossover study design, it was estimated that 8–10 subjects would be required for an 80% power to detect a 5 mmHg change in PASP with an α value of 0.05. Normally distributed continuous variables were evaluated using two-way repeated measures analysis of variance (ANOVA). The ANOVA included terms for high altitude and IPC and compared low altitude, high altitude, IPC, and no IPC conditions. Post-hoc testing for continuous variables was performed using a paired 2-tailed Student's t-test. Continuous variables are reported as mean values±one standard deviation (SD). A p value of<0.05 was considered significant.
Results
Effect of IPC on oxygen saturation
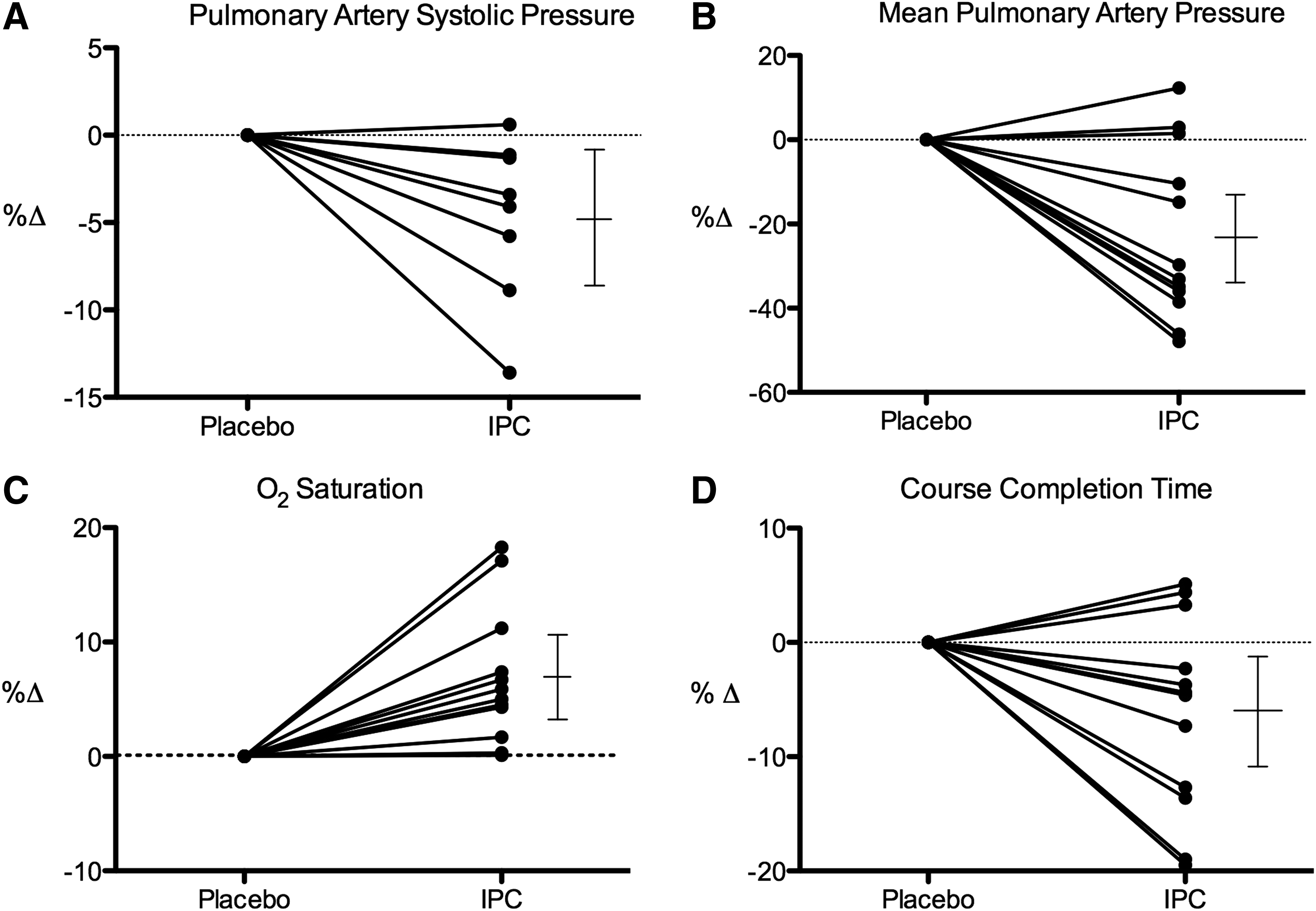
At the summit, oxygen saturation was significantly higher in the IPC condition compared to the placebo.
Effect of IPC on pulmonary pressures
Eight of the twelve subjects had spectral Doppler tricuspid regurgitation data that met quality standards for paired matching of testing conditions determined independently by two sonographers. Analysis of variance (ANOVA) demonstrated a significant increase in PASP at the summit vs. low altitude (p=0.001) for all conditions and a significant lowering of PASP after IPC vs. placebo at the summit. The altitude-related increase in PASP was attenuated by 21.6% following IPC compared to placebo (p<0.05). To further evaluate these pressure changes, we administered 100% oxygen for 15 min at the summit and then repeated echocardiography. Following 100% oxygen administration for 15 min at the summit, the PASP normalized to low altitude values for both the placebo and IPC conditions.
The response of the mPAP for each condition was similar to the PASP findings described above. Paired post oxygen data were limited to 8 of 12 study subjects due to equipment failures. In these 8 individuals, supplemental oxygen decreased the mPAP for both the placebo and IPC conditions (Fig. 1).

Effect of IPC on exercise performance
The average time to complete the 12.8 km run was significantly faster when pretreated with IPC compared with placebo pretreatment. See Table 1 and Figure 2 for study results and percentage change graphs.
Graphs
bpm, beats per minute; CO, cardiac output; IPC, ischemic preconditioning of the lower extremity; L, liters; LA, low altitude; min, minutes; mPAP, mean pulmonary artery pressure; PASP, estimated pulmonary artery systolic pressure; PVR, pulmonary vascular resistance.
Summit data represent resting values obtained at the time of echocardiography, 20–30 min following completion of the course run.
1, LA Placebo vs. LA IPC; 2, Summit Placebo vs. Summit IPC.
8 subjects with matched data for the 4 study conditions.
Discussion
This study demonstrated significant attenuation of hypoxic pulmonary vasoconstriction and improved oxygen saturation at altitude following IPC treatment. To our knowledge, this is the first study to test and demonstrate the late IPC effects on HPV in humans at high altitude.
Historical perspective
Ischemic preconditioning has a number of profound physiologic effects highlighted by three important studies. Murry et al. (1986) demonstrated that when IPC was applied to canine myocardial tissue, there was a 2–3 hour protective effect against subsequent ischemic insult. This initial protective effect has been termed the “early” or “classic” phase. Marber et al. (1993) demonstrated a second less intense protective period after IPC that returned at hour 12–24 and lasted 48–72 hours. Finally, Przyklenk et al. (1993) discovered that IPC applied to a single canine coronary artery distribution induced protective effects to surrounding coronary distributions. Hausenloy, Ali, and Dave individually extended the findings of Przyklenk, and demonstrated the protective effects of IPC on distant organs including the heart, kidneys, and brain, when IPC is applied to an extremity (Dave et al., 2006; Ali et al., 2007; Hausenloy et al., 2007). In addition, Birnbaum et al. (1997) also reported a significant protective effect of remote IPC (lower limb ischemia-preconditioning) on the size of myocardial infarcts following acute coronary occlusion in rabbits. Interestingly, these researchers also included the paradigm of skeletal muscle electrical stimulation and found that IPC at a distant site can afford protection to the myocardium independent of lower limb muscle stimulation (Birnbaum et al., 1997). The protective effects observed in distant vascular beds has been termed “remote IPC” ( Przyklenk et al., 1993; Birnbaum et al., 1997; Kharbanda et al., 2002).
Effect of IPC on pulmonary pressures
Although the mechanisms responsible for HPV continue to be debated, evidence suggests that endothelin (Berger et al., 2009), increased sympathetic nervous system activity (Duplain et al., 1999), the loss of bioactive metabolites, and increased free radical production (Bailey et al., 2010) all play important modulating roles. Our hypothesis that IPC would attenuate HPV was postulated from the fact that IPC activates vasodilatory and anti-inflammatory pathways that may counteract the mechanisms responsible for HPV. The systemic effects of IPC are largely attributed to the release of vasoactive molecules, such as nitric oxide, bradykinin, oxygen free radicals, and adenosine (Vanden Hoek et al., 1998; Jaberansari et al., 2001; Yellon and Downey, 2003; Auchampach et al., 2004; Eckle et al., 2008), which are also known to affect the pulmonary vasculature (Mentzer et al., 1975; Russell et al., 1990; Balanos et al., 2002; Connolly and Aaronson, 2010; Ketabchi et al., 2012). Additionally, hypoxia-inducible factor 1-α is central in both the physiologic response to altitude and cardioprotection from IPC (Eckle et al., 2008).
Compelling evidence demonstrates that IPC has beneficial effects in ischemic reperfusion injury of the heart (Gho et al., 1996; Ali et al., 2007; Botker et al., 2010), kidneys (Ali et al., 2007), and brain (Dave et al., 2006). Our findings suggest that IPC also has important vasoactive roles in the pulmonary circulation and might be considered in future randomized controlled trials to determine if this simple treatment could have clinical implications for disease states associated with exaggerated HPV such as high altitude pulmonary edema and pulmonary hypertension. If so, IPC could be easily applied in remote high altitude emergency situations where other treatments modalities (decent from high altitude, supplemental oxygen, dexamethasone, phosphodiesterase inhibitors, etc) are not readily available.
Effect of IPC on oxygen saturation
In our study subjects, Sp
The protective effects of IPC occur in two phases. The first effect peaks at about 90 minutes after treatment, and the second appears 24 hours after treatment. Our study was designed to test the effects of the second phase of IPC, which has been attributed to the upregulation of nitric oxide (NO). While the second phase is known to be less potent than the early phase, it is more robust and ubiquitous (Bolli et al., 1997; Hausenloy and Yellon, 2010). Local NO has been shown to induce changes in mitochondrial respiration, becoming more potent as O2 concentration decreases (Shiva et al., 2007). It follows that NO-mediated effects on mitochondrial respiration may decrease O2 utilization at the cellular level, thereby maintaining arterial O2 saturation. Although speculative, IPC could induce changes in mitochondrial respiration via NO thereby contributing to improved oxygen saturation.
Effect of IPC on exercise performance
Hypoxia-induced impairment of exercise performance is largely influenced by cardiac output, arterial oxygenation, vasodilation, and oxygen uptake capabilities, including
Limitations
Due to the nature of the intervention, our study subjects were not completely blinded to IPC and placebo conditions. While knowledge of study conditions may have affected exercise performance, it is unlikely that this knowledge could have affected pulmonary pressures or O2 saturation. Our study was also limited to a small number of healthy subjects who were conditioned to intense exercise regimens. Therefore, our findings are not extendable to the general population or to individuals who suffer from pathological conditions of the cardiopulmonary system in which these parameters play a critical role. Specifically, whether IPC affects pulmonary artery pressures, pulse oximetry, or exercise capacity in nonathletic or even unhealthy individuals, with or without confounding co-morbidities, remains unresolved and provides a compelling avenue for future research.
Conclusions
This study demonstrates significant attenuation of the normal hypoxic increase of pulmonary artery pressures and improvement of oxygen saturation at altitude more than 3 hours following IPC treatment. Future studies are warranted to identify the molecular mechanisms responsible for these findings and to determine the extent of the effect on less healthy individuals.
Footnotes
Acknowledgments
Numerous individuals donated their financial, technical, and time resources to this project. We wish to particularly acknowledge the invaluable efforts of Laura Weaver-Carnahan (study nurse), Brent Carnahan (logistical support), Bertha Jadovitz (registered diagnostic cardiac sonographer), Brendan Matus, Moussa Saleh, Claire-Alyce Andrews, Jeremy Van't Hof, and each of the study subjects who donated their time and effort to make this project possible. Thanks to Siemens for loaning the portable P50 ultrasound machines without which the study data could not have been collected. Additionally, we wish to thank the staff at the Barcroft Laboratory, White Mountain Research Station for the use of their excellent facilities.
Author Disclosure Statement
No competing financial interests exist.