
Abstract
Abstract
O'Brien, Catherine, John W. Castellani, and Stephen R. Muza. Acute hypobaric hypoxia effects on finger temperature during and after local cold exposure. High Alt Med Biol 16:244–250, 2015.—Mountain environments have combined stressors of lower ambient temperature and hypoxia. Cold alone can reduce finger temperature, resulting in discomfort, impaired dexterity, and increased risk of cold injury. Whether hypobaric hypoxia exacerbates these effects is unclear. To examine this, finger temperature responses to two cold water immersion tests were measured at sea level (SL, 99 kPa), 3000 m (70 kPa), and 4675 m (56 kPa) at the same air temperature (22°–23°C). Nine males sat quietly for 30 min, then completed the tests in balanced order. For the cold-induced vasodilation (CIVD) test, middle finger pad temperature was measured during immersion in 4°C water for 30 min. For the Rewarming test, finger temperature was measured for 30 min following a 5 min hand immersion in 16°C water. Average oxygen saturation was 98.6% during SL, 90.7% at 3000 m, and 75.8% at 4657 m. Mean finger temperature during the CIVD test (7.1°C) was similar among trials. There was no difference in CIVD parameters of nadir, apex, or mean finger temperatures; however both onset and apex times were earlier at 3000 m, compared to SL (0.6 min and 1.6 min, respectively). These differences did not persist at 4657 m. Rewarming after hand immersion was similar among trials, reaching 22.7°C after 30 min, compared to an initial finger temperature of 29.3°C. The results of this study provide no evidence that hypobaric hypoxia increases risk of cold injury. Previous findings of blunted finger temperatures at altitude are likely due to the lower ambient temperature that typically occurs at higher elevations.
Introduction
M
One method for examining finger temperature response is the cold-induced vasodilation response (CIVD), a cyclic oscillation in blood flow that occurs in the extremities during prolonged cold exposure (Lewis, 1930). CIVD is a reproducible response when measured under controlled conditions (O'Brien, 2005) and is believed to offer some protection against cold injury (Wilson and Goldman, 1970; Daanen and van der Struijs, 2005). Few studies have examined the effect of altitude on CIVD.
Daanen and Van Ruiten (2000) measured CIVD during single finger immersion in ice water for 30 min, a method that could easily be administered in the field, at elevations as high as 5100 m and at sea level. They found blunted CIVD at altitude; however, the ambient temperature during the altitude tests was 3.5°C lower than at sea level, resulting in lower initial skin temperature which can itself blunt CIVD (Daanen et al., 1997). In another study, Mathew et al. (1977) measured the CIVD response during hand immersion in 4°C water and found blunted responses in lowlanders air-lifted to 3500 m, compared to sea level. But again, the air temperature at altitude was lower. From these studies, it is unclear whether CIVD at altitude was blunted due to the hypobaric hypoxia or due to the lower ambient temperature.
In an attempt to control for the lower ambient temperature at altitude, Takeoka et al. (1993) measured CIVD in a tent controlled at ∼23°C at 2260 m and 4860 m altitude in Japanese sea level residents and high altitude natives. Both groups had lower finger temperatures at the higher altitude, with a difference of ∼3.0°C in the Japanese. However, when the Japanese were tested in a hypobaric chamber controlled at 25°C after returning to sea level, they showed the opposite results: finger temperature during cold water immersion was ∼0.7°C higher at 4000 m, compared to 2000 m (Takeoka et al., 1993). This difference was primarily due to the CIVD response at 2000 m in the chamber, where mean finger temperature was ∼4°C lower than at 2260 m altitude. No mechanism was presented for these unexpected findings, although there are several confounding factors. For example, while temperature during the CIVD test at altitude was controlled, outdoor ambient temperatures at 4860 m was lower (17°C) than at 2260 (23°C) or sea level (24°C). How long volunteers were in the temperature-controlled tent before testing began, and whether the tests were performed on separate days, sequentially, or randomized were not reported. Finally, no sea level control tests were performed, which could have provided insight into possible adaptations due to high altitude exposure.
The confounding results of these studies indicated a need for a controlled climatic chamber study on the effect of hypobaric hypoxia on CIVD. Meeuwsen et al. (2009) performed such a study comparing normobaric normoxia to hypobaric hypoxia, as well as normobaric hypoxia and hypobaric normoxia, using a simulated altitude of 3353 m. The only difference found in finger temperatures was a lower amplitude of CIVD with hypoxia (Meeuwsen et al., 2009). Since mean finger temperature was unaffected, the physiological significance of this finding may not be meaningful. Alternatively, it may be that this represented a level of hypoxia at which changes begin to appear, and that greater changes would occur at higher altitude.
The purpose of the present study was to examine the effect of two altitudes on baseline finger temperature, finger temperature during cold exposure (the CIVD response) and finger temperature during rewarming from cold water immersion, compared to sea level responses. We hypothesized that finger temperature would be lower during the altitude exposures, compared to sea level. Both finger temperature response during the CIVD test (Daanen and van der Struijs, 2005), as well as finger rewarming rate after brief cold water immersion (Brändström et al., 2008) have been related to susceptibility to cold injury during military field training in cold regions. Cold injury to the feet is also a concern (Daanen and van der Struijs, 2005); therefore, foot temperature was also measured. Any changes in these responses due to hypoxia would be important during military operations with combined cold and altitude stressors, as well as for mountain sojourners. These experimental tests were performed using a temperature-controlled hypobaric chamber and unacclimatized, resting subjects who have not been subjected to the rigors of ascent to high altitude and the corresponding cold exposure.
Methods
Nine male volunteers participated in this study, which was approved by the U.S. Army Research Institute of Environmental Medicine Scientific and Human Use Review Committees. Each volunteer gave his written informed consent after being briefed on the purpose, experimental procedures, and known risks of the study. Investigators adhered to Army Regulation 70-25 and U.S. Army Medical Research and Materiel Command Regulation 70-25 on the use of volunteers in research. Volunteers were medically screened to exclude individuals who had a history of cold injury, difficulty equalizing pressure in their ears, or recently been exposed to altitude above 1200 m for longer than 4 days. Volunteers were restricted from tobacco use on the morning of an experimental trial. Participants had a mean±SD age of 23.8±5.3 years; height 171.8±5.9 cm; weight 79.3±13.3 kg; and body fat 17.9±6.0%.
The study consisted of three separate experimental trials, which differed only in barometric pressure. Barometric pressure was set at 99 kPa (225 m) for sea level (SL), 70 kPa (3000 m) for moderate altitude, and 56 kPa (4675 m) for high altitude. Trials were spaced a week apart, with the order of trials balanced among volunteers. Before beginning the trials, volunteers participated in an altitude chamber familiarization session to accustom them to the sensation of their ears equalizing to the pressure changes and to provide them with safety training. Trials were not blinded, as pressure changes indicated to volunteers whether they were at sea level or altitude. However, they were not told which trial was being conducted, nor did they observe pulse oximeter readings.
Familiarization
The air temperature during the experimental trials was intended to be neutral for the volunteers, such that there was neither a drive to conserve heat (resulting in finger vasoconstriction) or lose heat (resulting in finger vasodilation). The air temperature during the familiarization session was initially set at 22°C, but was adjusted upwards by 0.5°C increments if volunteers felt too cool. Since “thermoneutral” varies among individuals (Boudewyns, 1985), volunteers were allowed to adjust their clothing layers (Army Physical Training uniform) to achieve their own thermal comfort. The air temperature and clothing layers determined during the familiarization sessions were thereafter standardized for the experimental trials.
Volunteers were also familiarized with the water temperatures used for the CIVD and hand rewarming tests, as well as with the Thermal Sensation (TS) and Thermal Comfort (TC) scales (Berglund, 1998), and the modified Environmental Symptoms Questionnaire (ESQ) (Beidleman et al., 2007), that were administered by computer. The supplementary modified ESQ, or Altitude Illness Symptoms Questionnaire, is used to assess symptoms of altitude illness, with a score greater to or equal than 0.7 indicative of acute mountain sickness (AMS). (Supplementary material is available online at www.liebertpub.com/ham.) Although the short duration of altitude exposure in this study was unlikely to cause AMS, if symptoms did occur and were associated with autonomic nervous system changes, finger blood flow responses could be affected. In this event, the data from those volunteers would be excluded from analysis. Thermal sensation (TS) was measured on a scale that ranged from 0.0 (unbearably cold) to 8.0 (unbearably hot), where 4.0=comfortable; 3.0=cool; 5.0=warm. Thermal comfort (TC) was measured on a scale from 0 (comfortable) to 4 (intolerable), where 1 was slightly uncomfortable.
Experimental trials
For the experimental trials, volunteers reported to the laboratory for breakfast at 0630 h, then rested quietly until entering the hypobaric chamber at 0800 h. They remained seated while combination heat flow and temperature sensors (Concept Engineering, Old Saybrook, CT) were attached at seven skin sites (chest, upper arm, forearm, back of hand, thigh, calf, top of foot), and thermistors (YSI 2252, Yellow Springs OH) were attached to the right and left middle finger pads. Mean skin temperature was calculated as [0.3 * (chest+arm)+0.2 * (thigh+calf)] (Ramanathan, 1964). Because experimental trials were conducted under neutral conditions and local cold exposure was limited to a small surface area (finger) or short duration (hand), the stimulus for a change in heat balance was negligible and core temperature was not measured. After attaching the sensors, the chamber atmosphere was adjusted for the appropriate altitude, which took about 15 min for the two altitude trials. On the SL trial, the small change in pressure sealed the doors so that the environmental conditions could be maintained.
For the first 20 min of exposure, volunteers sat quietly. They then completed the computerized tests of TS, TC, and ESQ. After completion of these tests, a noninvasive finger pulse oximeter (Model 8600, Nonin Medical, Inc, Plymouth, MN) was attached to the index finger to measure arterial oxygen saturation and heart rate, and data were averaged over 1 minute. Finally, thermography images (Model SC4000, FLIR Systems, Billerica, MA) were taken of the dorsal side of each hand, which rested on a flat surface.
Cold tests
After 30 min exposure, the first cold-water immersion test was performed. Each volunteer completed two tests: the CIVD test, which measured skin temperature during immersion of a single finger, and the Rewarming test, which measured skin temperature during recovery from a brief immersion of the whole hand. The order of tests was balanced among volunteers, with the second test, performed with the opposite hand, beginning at 70 min. At 110 min, both tests were completed and the ESQ/TS/TC tests were administered, oxygen saturation and heart rate were measured, and thermography images of both hands were made.
During the CIVD Test, middle finger pad temperature was measured during immersion in 4°C water for 30 min (O'Brien, 2005). The hand was supported by a plexiglass plate, with the middle finger bent to extend down into the water up to the proximal interphalangeal joint.
For the Rewarming test, a thin (0.03175 mm) polyethylene glove was worn to prevent evaporative cooling due to moisture on the hand from confounding the skin temperature during rewarming. The hand was immersed to the level of the styloid processes of the radius and ulna in 16°C water for 5 min, and the glove was taken off as the hand was removed from the water so that the thermography measurements, taken for the next 30 min as the hand rewarmed, were directly from the dry skin surface. Average temperature within a 1 cm circle at the middle finger nailbed, determined using FLIR ThermaCAM Researcher software, was used for data analysis.
Statistical analyses
The primary purpose of this study was to determine whether hypobaric hypoxia alters finger blood flow as indexed by finger skin temperature. During the CIVD test, the following parameters were compared: initial finger temperature, nadir and apex temperatures, onset of vasodilation, and mean finger temperature during cold-water immersion (O'Brien, 2005). During the Rewarming test, comparisons were made over time, from pre-immersion to 1, 5, 10, 20, and 30 min post-immersion. Mean skin temperature and foot temperature were analyzed using time points during each computer test (25 min and 115 min), as well as between the two cold water immersion tests (65 min). The ESQ, TS, and TC scores were also compared at the two time points of the computer tests. Statistical analyses were performed using repeated measures ANOVA, with each volunteer serving as his own control. Statistical significance was set at p<0.05. When significant F-ratios were found, paired comparisons were made using Tukey's Honestly Significant Difference post-hoc test. All data are shown as mean±standard deviation.
Results
The three simulated altitude conditions produced average oxygen saturation levels that were significantly different among all three trials (p<0.001), falling from SL (98.6±0.7%) to 3000 m (90.7±3.2%) and again to 4675 m (75.8±5.3%). Two participants reached a score of 0.7 on the ESQ after 25 min at 4675 m; one resolved shortly and was well below that threshold at the time of the second ESQ test, and the other resolved with supplemental oxygen at the end of the trial. Since their remaining data were within the range of the remaining volunteers, they were not excluded from analysis.
Air temperature (set at 22°C for the first two volunteers, 22.5°C for the next two volunteers, and 23°C for the remaining five) was similar (p>0.05, SD 0.3°C) among trials for each volunteer. All volunteers wore long pants; three volunteers chose to wear only short-sleeved shirts, while the remaining six wore both a long-sleeved shirt and lightweight nylon jacket. The same clothing was worn on all three trials. There was no difference in TS among trials; however, TS increased (p=0.043) over time, from “comfortable” (4.0±0.9) at 25 min to “slightly warm” (4.3±0.8) at 110 min. There was no difference (p>0.05) among trials or over time for TC, which was rated as “comfortable” (0.2±0.6).
Mean skin temperature (Fig. 1) was higher (p=0.005 for time x trial interaction) at 4675 m, compared to SL or 3000 m, and did not change during exposure to 4675 m, but fell over time (p<0.05) during both SL and 3000 m. While it appears that mean skin temperature began to increase during the second half of the exposure to 4675 m, the increase is only ∼0.2°C and was not statistically significant.
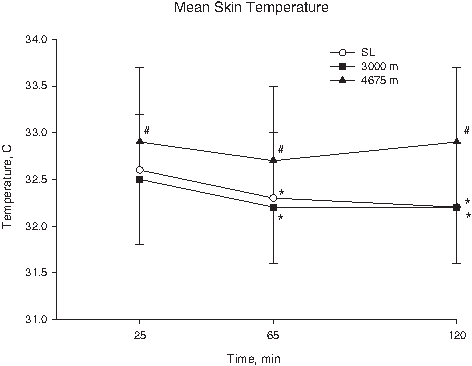
Mean skin temperature is presented for all three trials. * indicates significant difference from temperature at 25 min. # indicates significant difference between 4675 m and both SL and 3000 m.
Foot skin temperature (Fig. 2) fell (p=0.005 for time x trial interaction) during all three trials; however, it was lower after 65 min during SL than either of the altitude trials, and at 120 min foot temperature among all three trials was significantly different.
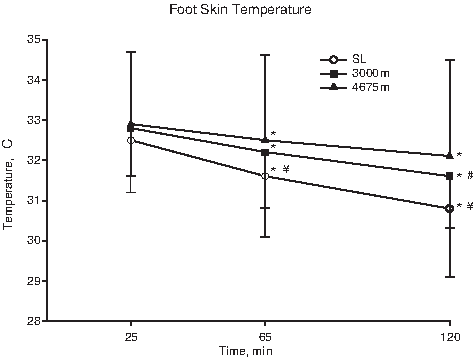
Foot skin temperature is presented for all three trials. * indicates significant difference from temperature at 25 min. ¥ indicates significant difference from 3000 m and 4675 m. # indicates significant difference from 4675 m.
CIVD parameters are shown in Table 1. There was no significant difference among trials for finger temperature before immersion, or for nadir, apex, or mean finger temperature. Both onset (p=0.007) and apex (p=0.026) times were earlier at 3000 m, compared to sea level; however, this earlier shift did not persist at 4675 m. Figure 3 shows a representation of the CIVD response for each trial. This graph was made by combining the data of all volunteers for each trial. This dampens the values for individual parameters because they are averaged, but the relative differences among trials can be seen, including the earlier shift in timing of CIVD during the 3000 m exposure.
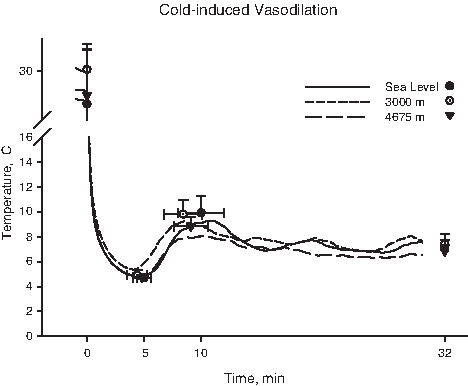
Cold-induced vasodilation is presented as a composite of data from all volunteers, and shows the leftward shift in the time components (nadir and apex) at 3000 m. Because the composite data are averaged across all subjects, the times and temperatures of nadir and apex are dampened; therefore, mean and standard deviation are also shown for initial, nadir, apex, and mean finger temperatures at sea level (open circles), 3000 m (closed squares), and 4675 m (closed triangles).
Significant difference (p<0.05) compared to Sea Level.
Rewarming from cold-water hand immersion (Fig. 4) did not differ among trials. Initial finger temperature was 29.3±2.6°C. Ten minutes after hand immersion in 16°C water, finger temperature was 20.3±2.3°C, but rose to only 22.7±4.7°C after 30 min of rewarming.

Rewarming from cold-water immersion is presented for all three trials. There were no differences among trials (p>0.05). Overall mean and standard deviation of finger temperature is shown by the closed circles before immersion and after 5, 10, and 30 min rewarming.
Discussion
In a temperature-controlled hypobaric chamber, finger temperature responses to local cold exposure were evaluated at sea level and two simulated altitudes (3000 m and 4675 m). We sought to determine whether hypobaric hypoxia alters finger temperature response to local cold exposure when ambient temperature is controlled. Other factors known to influence finger blood flow and the CIVD response were also controlled, including time of day, posture, food intake, recent activity, and tobacco smoking (Daanen, 2003; O'Brien, 2005). This study demonstrated no effect of hypobaric hypoxia per se on the finger temperature response during CIVD or on rewarming from cold-water immersion. While there was a shift toward an earlier time course of CIVD at 3000 m, compared to SL, the magnitude was within the day-to-day reproducibility of the time parameters (O'Brien, 2005) and the shift did not persist at 4675 m.
Previous studies finding blunted CIVD with hypoxia may have been confounded by factors such as lower ambient temperature during altitude exposures ( Mathew et al., 1977; Daanen and Van Ruiten, 2000) or other adaptations that may occur with longer duration altitude exposure (Takeoka et al., 1993). Meeuwsen et al. (2009) controlled for these variables, and while they found a lower amplitude of CIVD at 3353 m compared to sea level, no other parameters, such as nadir, apex, or mean finger temperature, were affected (Meeuwsen et al., 2009). Thus, the results of the studies examining the effect of hypobaric hypoxia are inconsistent, and the physiological significance of changes that have been reported may not be meaningful.
Breathing hypoxic air stimulates chemoreceptors that increase sympathetic activity, resulting in vasoconstriction to maintain arterial pressure and coronary and cerebral blood flow (Heistad and Abboud, 1980; Hansen and Sander, 2003). However, local tissue hypoxia elicits an increase in blood flow in order to maintain the oxygen delivery required for metabolism (Cabrales et al., 2006). Furthermore, different types of blood vessels may respond differently to hypoxia (Folkow, 1955; Bertuglia et al., 1991). The net change at the tissue level reflects a balance between local mechanisms for vasodilation and central mechanisms for vasoconstriction. This may explain the differences in skin temperature observed in one region, compared to another.
In the present study, while finger temperature was not affected by hypobaric hypoxia, this was not the case in non-acral skin. Mean skin temperature remained higher throughout the trial at 4675 m than either SL or 3000 m. This is in agreement with previous investigations (Cipriano and Goldman, 1975; Sagawa et al., 1986), and suggests a threshold level of hypobaric hypoxia, in this case above 3000 m.
Ambient temperature also influences this response. Under cold conditions (15.5°C), Cipriano and Goldman found higher mean skin temperature at 5000 m, compared to sea level, and at 2500 m skin temperature was in between (Cipriano and Goldman, 1975). At warmer ambient temperatures the effect was reduced, such that at 21°C mean skin temperature was only significantly higher than sea level at 5000 m, and at 26.5°C there was no difference among trials (Cipriano and Goldman, 1975).
In contrast to mean skin temperature, skin temperature on the top of the foot, which is also non-acral skin, remained higher at both altitudes, compared to sea level, and decreased over time. In this case, the effect appeared to be graded by altitude exposure, with foot temperature at 4675 m higher than at 3000 m. Foot skin temperature was slightly lower than mean skin temperature. In non-acral skin, while the primary determinant of skin blood flow is core temperature, thresholds for vasodilation or vasoconstriction, as well as the slope of the rate of change, can be shifted by other factors, including local skin temperature and hypoxia (Minson, 2003).
In general, higher mean skin temperature is associated with higher finger temperatures, both at baseline and during CIVD, and the time course of CIVD may also be shifted to an earlier onset (Daanen et al., 1997). However, finger temperatures during CIVD were similar among trials, and although there was a shift to earlier onset and apex times of CIVD at 3000 m, this did not persist at 4675 m. This may be because the higher mean skin temperature in the present study was a local effect induced by hypoxia, rather than a result of higher body heat content.
Hand rewarming was slower than expected on all trials, with half the volunteers not reaching 20°C even after 30 min rewarming. In a previous experiment in our laboratory (unpublished data) at a room temperature of 28°C, rewarming from cold water hand immersion was rapid and began in the fingertips, suggesting opening of arteriovenous anastomoses (AVA). This is likely related to body heat content ( Folkow, 1955; Flouris and Cheung, 2009), and may be why some investigators conduct this test at slightly warmer ambient temperatures (Bartelink et al., 1993; Lindsell, 2005; Poole et al., 2006; Ruijs et al., 2009) or immerse a smaller region, such as just the fingers (Cleophas et al., 1982).
However, it can be difficult to standardize body heat content among individuals. One method is to test each individual in their own thermoneutral zone, which can be identified using blood velocity measurements that corresponded to rapid opening and closing of AVAs (Bergersen et al., 1999). As ambient temperature falls from thermoneutral, the temperature at which vasoconstriction occurs varies among individuals (Vanggaard et al., 2011), which could explain the variability in the response among subjects that is typically observed. For example, at an air temperature of 24°C, there is a bimodal distribution of finger skin temperatures, with some individuals around 33°C and others around 24°C (Boudewyns, 1985). Administering the test under thermoneutral conditions may reduce variability among individuals, improve reproducibility, and allow discrimination among individuals with cold injury, such as vibration-induced white finger or Raynaud's Phenomenon. From a practical standpoint, a rewarming test would seem relevant for cold-weather activities; however, when measured at normal room temperature, these tests appear to have little diagnostic value (Bartelink et al., 1993; Laskar and Harada, 2005; Poole et al., 2006).
Likewise, because this study was intended to examine the effects of hypobaric hypoxia on finger temperatures, a neutral ambient temperature was desired, such that both heat loss and heat production mechanisms were minimized. Given the individual variability in thermoneutral conditions, rather than standardize air temperature and clothing for all volunteers, individual adjustments for thermal comfort were allowed during the Familiarization session. Thereafter, conditions remained the same for the experimental trials, and each volunteer served as his own control. This method may be similar to conditions in the field, where individuals dress for their own comfort; however, when comparing thermoregulatory responses among groups, standardized conditions may be preferred. The challenge is to standardize both the environmental conditions and initial thermal state of the volunteers simultaneously.
The altitude exposure in the present study was acute and of short duration. Some studies suggest altitude acclimatization alters CIVD. Daanen and Van Ruiten (2000) observed blunted CIVD after 3 days at altitude, but the response had nearly recovered to sea level values in subjects who remained at altitude for 45 days. Mathew et al. (1977) found the lowest CIVD response in lowlanders who were airlifted to altitude, highest in high-altitude natives, and an in between response for lowlanders who resided at high altitude for a year. Note that these studies found blunted CIVD even with acute exposure to altitude, which we attributed to the confounding factors inherent in field studies, such as lower air temperature. However, laboratory studies have demonstrated adaptations to hypoxia that could be involved in acral blood flow regulation. Altitude acclimation of a few weeks has been shown to restore arterial oxygen content, although sympathetic activity ( Durand et al., 1969; Rostrup, 1998; Calbert, 2003) and mean skin temperature (Blatteis and Lutherer, 1976) remain elevated. The complex interaction between central and local effects makes it difficult to speculate on how these changes may affect CIVD.
In summary, no evidence was found that hypobaric hypoxia increases risk of cold injury, as assessed by baseline finger temperatures, as well as the response during and following extremity cold water immersion. Previous findings of blunted CIVD during altitude exposure (Mathew et al., 1977; Takeoka et al., 1993; Daanen and Van Ruiten, 2000) are likely due to the lower ambient temperatures that also typically occur with increasing elevation, rather than the hypoxia per se. Although one study controlled for these values and found a reduced amplitude of CIVD with hypobaric hypoxia, overall mean finger temperature was no different from sea level values (Meeuwsen et al., 2009). For individuals traveling to high altitude, a more important factor may be the elevated mean skin and foot temperatures observed with hypoxia, which could result in greater heat loss and thereby increase risk of hypothermia.
Footnotes
Acknowledgments
Human subjects participated in this study after giving their free and informed voluntary consent. The investigators adhered to Department of Defense Instruction 3216.02 and 32 CFR 219 on the use of volunteers in research.
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the Army or the Department of Defense.
Any citations of commercial organizations and trade names in this report do not constitute an official Department of the Army endorsement of approval of the products or services of these organizations.
Author Disclosure Statement
The authors declare they have no conflicting financial interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.