
Abstract
Abstract
Lankford, Harvey V. Dull brains, mountaineers, and Mosso: Hypoxic words from on high. High Alt Med Biol 16:363–370, 2015.— Dull and hypoxic brains have been a frequent subject in the medical and mountaineering literature. Deterioration of cognitive and other neurological function occurs at high altitude, with or without high altitude cerebral edema. This historical essay explores a 2014 first-ever English translation of cerebral blood flow studies by nineteenth century physiologist Angelo Mosso. Some of the medical history and physiology of brain function is discussed, but much of the style focuses on quotations from the writings of mountaineers and mountaineering physicians to provide color commentary about dull brains at high altitude.
Introduction
T
This historical study will feature the quotations of mountaineers and mountaineer physicians about their dull and hypoxic brains with headaches, intellectual decline, memory loss, time warp, hallucinations, flattened emotions, and other changes from the effects of extreme altitude, with or without High Altitude Cerebral Edema (HACE). The essay will also explore a 2014 first-ever English translation of cerebral blood flow studies by the nineteenth century physiologist Angelo Mosso.
Although performed near sea level in Turin, Italy, rather than in his later mountain laboratory, several aspects of his brain research are applicable to high altitude. Some medical history and physiology of brain function will be discussed in a limited fashion, but the Words From On High style of the author (Lankford 2009, 2014a, 2014b, 2014c) will focus on quotations from the writings of mountaineers and mountaineering physicians to provide color commentary about dull brains at high altitude.
Angelo Mosso and Circulation of the Blood in the Brain
There are many arbitrary starting points for a discussion about brains at high altitude. For example, headaches in the mountains were known from ancient times, and there have been countless comments by altitude-sufferers about headaches. Hypoxic symptoms were recognized in balloon ascents of the late 1700s, and two deaths occurred when French physiologist Paul Bert's colleagues ascended rapidly by balloon to roughly the height of Mt. Everest (1878, p. 967).
Angelo Mosso (1846–1910) was a prolific physiology pioneer of that same era. While he has long been known to students of high altitude, there has been a resurgence of interest in him. For example, his 1894 studies at the 4560 m Capanna Regina Margherita laboratory in the Italian Alps (Mosso, 1897, 1898) were used as a centerpiece in our review of the history and physiology of the right ventricle at high altitude (Lankford and Swenson, 2014c). Mosso's hypobaric chamber exposures and his theories on “acapnia,” rather than Bert's correct hypoxia as a cause of the dominant physiological effects of high altitude, were reviewed by Di Giulio and West (2013). This current historical essay on dull brains at high altitude will instead include some of Mosso's work on the circulation of blood in the brain.
Sandrone et al. discussed recently-uncovered archives about a Mosso whole-body circulation balance machine (2014). Mosso's studies of vascular patterns led to improvements in his later direct brain studies, all of these performed in an attempt to qualitate cerebral blood flow (CBF), brain weight, and brain activity. They attribute to Mosso the establishment of a conceptual basis of some of today's noninvasive functional neuroimaging techniques that take advantage of changes in CBF characteristics.
In their commentary on the technological progression of brain imaging studies, Raichle and Shephard also praised Mosso, even though he could not foretell all of the complex factors and tools used in today's sophisticated brain activity mapping and imaging. (2014, p. xxvi). Lastly, in a review of CBF (Ainslie and Subudh, 2014), it was again noted that Mosso's observations of CBF preceded the quantitative ones by half a century, and like others, they recognized him as a forefather of high altitude cerebrovascular physiology.
Mosso's Sulla circolazione del sangue nel cervello dell'uomo (1879) was translated from Italian into German (Mosso, 1881), but not into English until 2014 by Christiane Nockels Fabbri in Angelo Mosso's Circulation of Blood in the Human Brain (Mosso, 2014) with editing and commentary by Raichle and Shepherd (2014). The English translation and the commentary, even though they are both in the same new book, will be cited separately throughout this article for clarity's sake. These sources and others help to chronicle the technological advance in measuring brain activity and allow this article's style to juxtapose history and science with mountaineering quotations to tell the story of dull and hypoxic brains in a richer way.
Mosso's Experiments on the Brain
In his book, Mosso first discussed the investigations of others but thought that they needed comparison to other influences. His terminology included brain “pulsations” and “oscillations” from cardiac and respiratory movements with their separate rhythms and neural controls, and independent “undulations” in the brain itself. In his own words, “cerebral pulse and volume changes of the brain which depend on a systemic cause, are to be distinguished from those that are purely local and specific to the brain, [so] the appropriate procedure must consist of the simultaneous recording of the pulse of the brain and that of another body part.” (Mosso, 2014, pp. 98–102). In recognizing this, he was able to anticipate the signal-to-noise problem still relevant in modern neuroimaging today (Sandrone, 2014).
He was able to do this with three unfortunate patients with longstanding skull defects from trauma or disease that had healed with pulsating fibrous scar over the dura mater (Mosso, 2014, pp. 33–45). He attached a small lever to the exposed tissue, improved upon a multipurpose Marey tambour apparatus, and traced brain volume (plethysmographic) movements onto a rotating cylinder kymograph (Mosso, 2014, pp. 43–48). The simultaneous multimodal recording of cerebral, respiratory, and peripheral vascular movements was made, the latter with a water-filled device for the arm adapted from his own previous studies of peripheral pulses. See Figures 1–3.

Mosso's plethysmographic apparatus for recording cerebral pulsations. Mosso. (1881). Fig. 1, Chapter 2, p 42. http://vlp.mpiwg-berlin.mpg.de/library/data/lit8288/index_html?pn=51&ws=1.5. All figures are from the Mosso German translation, and archive: Mosso A.(1881). Ueber den Kreislauf des Blutes im menschlichen Gehirn: Untersuchungen. Veit. Leipzig. http://vlp.mpiwg-berlin.mpg.de/library/data/lit8288/index_html?pn=4&ws=1.5. Università di Torino, Dipartimento di Neuroscienze, Sezione di Fisiologia: Biblioteca Angelo Mosso. http://vlp.mpiwg-berlin.mpg.de/library/data/lit25558? Last accessed March 18, 2015.
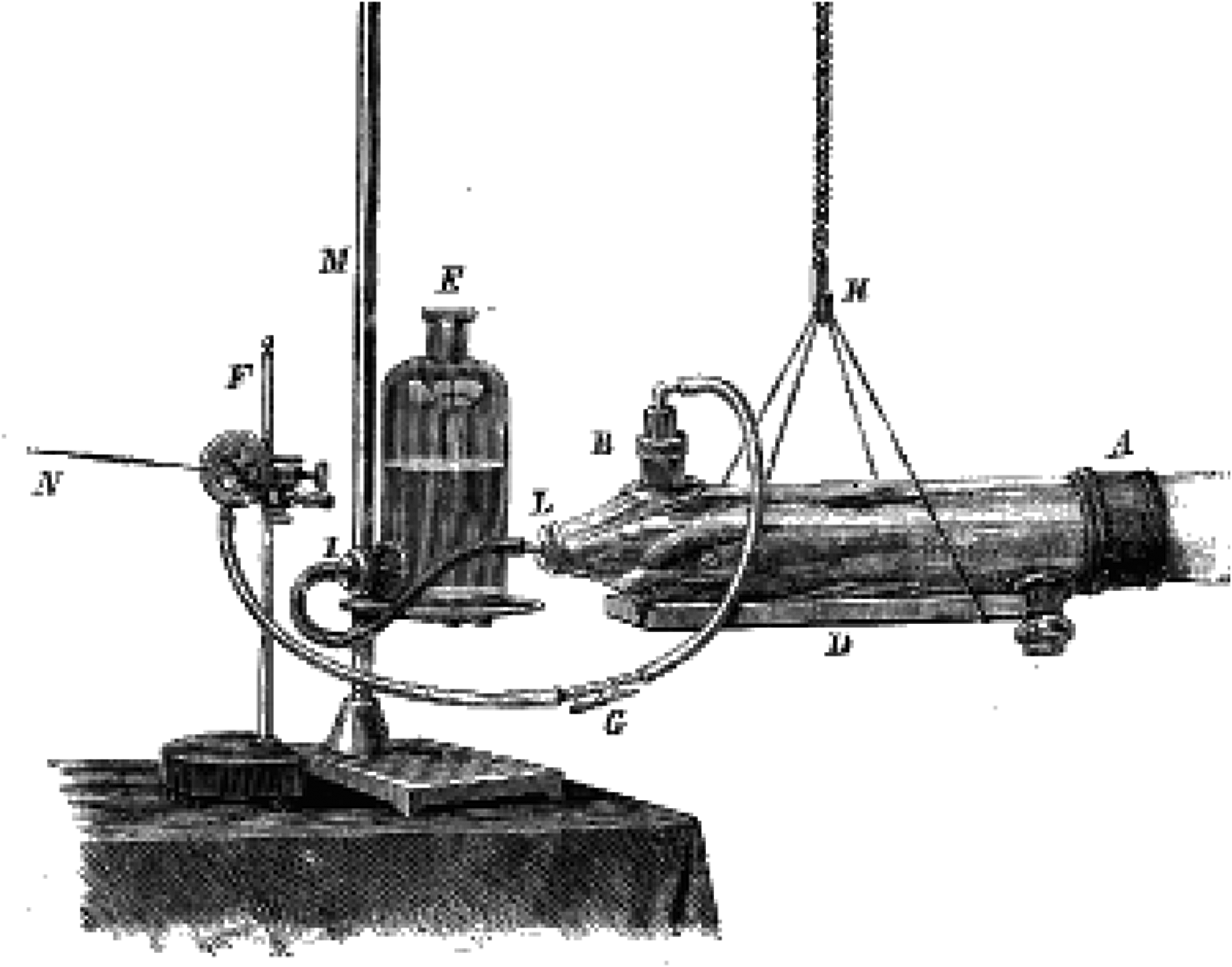
Mosso's hydrosphygmograph for measuring forearm circulatory phenomena. Mosso. (1881). Fig. 2, Chapter 2, p 44. http://vlp.mpiwg-berlin.mpg.de/library/data/lit8288/index_html?pn=53&ws=1.5.

Mosso's simultaneous recording on a rotating cylinder kymograph of the cerebral pulse (top line
Mosso traced blood flow wave contours to differentiate specific brain activity. His work began the long evolution to current imaging of regional brain blood flow changes in human cognitive and behavioral states. For example, he examined the varying effects from sleep versus awakening, dreaming, fasting versus fed states, warmed versus cooled states, mental activities such as arithmetic calculations, emotions, and drugs or chemicals such as ammonia, amyl nitrate, and chloral hydrate (Mosso, 2014, pp. 49–62, 107) Several features of his recordings agree with modern studies, including a delay of a few seconds, with onset and offset transients (Raichle and Shepherd, 2014, p. xix).
With his numerous studies, he was also aware of vessel wall elasticity, and some of the effects of oxygen and carbon dioxide (Mosso, 2014, pp.102, 125). This preceded by many decades our current knowledge that, applicable especially to high altitude and mountaineers, influences on CBF include arterial oxygen and carbon dioxide tensions, oxygen content, cerebrospinal fluid pH, hematocrit, hypoxic cerebral vasodilatation, hypocapnic cerebral vasoconstriction, hypoxic ventilatory response, and hypercapnic ventilatory response (Ainslie, 2014).
On the mountain, CBF is but one of the many factors associated with hypobaria, hypoxemia, adequate convective oxygen delivery, and contributing to symptoms of Acute Mountain Sickness (AMS) and HACE. Mountaineers have commented on how it feels in some situations similar to what Mosso observed in his lab near sea level, in his hypobaric chamber, and on Monte Rosa. Many of their stories follow and will be emphasized here.
Dull Brains
Mosso found increases in cerebral pulse volume and amplitude during intellectual activities (Mosso, 2014, pp. 66–70). At high altitude, anything intellectual or cognitive is more difficult, the severity of acute hypoxic exposure increasing with the amount of ascent. Impairment from chronic exposure also occurs in natives at high altitude, but is open to interpretation from a medico-sociological standpoint (Yan, 2014).
Mountaineers, on the other hand, have been unmistakable about their own mental deterioration, at least to the degree allowed by the witty Mallory quotation in the introduction. A more modern style of expressing it is by James Tabor in Forever on the Mountain on Denali: “Up high, the dumber you get, the smarter you think you're becoming.” (2007, p. 132).
Dull brains are a frequent topic in the mountaineer literature, and some famous names will appear here. A good place to start is with a prominent figure in the history of high altitude medicine. In 1938, on the first American expedition to K2, Charles Houston found that “I thought of all sorts of notes to write in the little book I carried, but somehow had not the mental energy to put them down.” (Houston and Bates, 1939, p. 279). In 1953 on his next and nearly fatal time there, he observed in K2 The Savage Mountain, “Was our judgment so warped by altitude that we really believed that we could go higher?” (Houston and Bates, 1954, p. 162).
A member of the 1953 Everest team, Wilfrid Noyce, declared that, “The top layers of my brain were probably dormant up there.” (1954, p. 237). To make matters much worse, Noyce would candidly admit, “At the time I thought I was as alert as at sea level.” (1954, p. 182). Such neurological cost of climbing to extreme altitude would later be studied by anesthesiologist Hornbein et al., (1989). On the West Ridge traverse of Everest in 1963, he himself had fatalistically depicted the outrageously dangerous, exposed, and hypoxic situation this way: “Death had no meaning, nor, for that matter, did life.” (1965, p. 175).
His partner, Willi Unsoeld, had wondered on that occasion about the brains of his teammate stating, “It was difficult to distinguish fanaticism from genius. Obviously, it was a kind of hypoxia.” (Coburn, 2013, p. 182). Unsoeld was actually no better off himself, admitting later in 1976 that, “losing a good part of his mental acuity on Mt. Everest in 1963, he didn't think that the richness of his life was reduced, ” (Roskelley, 1987, p.47). In Everest the Cruel Way during a winter climb, Joe Tasker had no illusions about his dull brain: “My mind was as active as a garden snail.” (1981, p. 71). The next year, he and Pete Boardman would disappear on the Northeast Ridge of Everest, their names honored afterwards on the Boardman-Tasker Prize for Mountain Literature.
This was a dilemma in high altitude mountaineering—risk versus reward. In West and Lahiri's High Altitude and Man with some of their work from the 1981 American Medical Research Expedition to Mt. Everest (AMREE), the chapter on Hypoxia and Brain Flow by Edelman et al. includes this admonition: “Higher cortical function … is almost definitely modified. Whether this is a hindrance (impairment of critical judgment) or an aid (creation of euphoria necessary to complete the arduous task), the climbers themselves must decide.” (1984, p. 101). The previous quote by Houston about the questionable wisdom of going higher suggests that criticism of mountaineers by others is justifiable. Said another way high on Aconcagua, the mental condition of this essay's author and his climbing partner, “suggested evidence of cerebral dysfunction. Going higher toward the summit was deemed proof by those not in the business.” (Lankford 2000).
Headaches
Mosso's three patients with holes in their heads certainly had reasons to have headache symptoms initially, and his first patient had them chronically, but this was not his research concern. As for mountaineers and others, ascent to high altitude often results in headache. High altitude headaches, AMS, and HACE with edematous brains may increase intracranial pressure (ICP) once the limits of compliance are reached, part of the cranial “tight fit” theory of Hackett (1999). This is still an unsettled topic.
Direct measurement of ICP is problematic in the field from a practical and ethical basis, multiple noninvasive methods give inconsistent results, and above all, the balance between cerebral arterial delivery and venous drainage must be considered (Wilson et al., 2014, Wilson, 2015). One might speculate, if the tight fit theory was more substantiated, that Mosso's three subjects with their “relief ports,” or at least the one with the brain atrophy and extra space, might have done well at high altitude if they had been taken to Mosso's Monte Rosa lab when it opened 15 years later.
Less colorfully, the pathophysiology of high altitude headache and cerebral edema includes these factors: arterial desaturation, vasodilatation and vasoconstriction, imbalances between cerebral inflow and outflow capacities, vasogenic and cytotoxic brain edema, changes in blood brain barrier permeability
There is no shortage of headache anecdotes from mountaineers. Mallory makes this comparison: “the dull height-headache … [is] not unlike the effect of poisoning by carbon monoxide.” (1923, p. 159). Rather than turning cherry red, a much later climber on the world's sixth tallest peak, Cho Oyu, made this graphic analogy, “My head was a boiled vegetable inside a bone pressure cooker.” (Berry 2012, p. 73). Tasker in Savage Arena warns us of the ominous continuum from simple AMS headache to HACE with some British understatement, “Apart from the difficulty of performing any action with such a low oxygen intake, there is also an unquantifiable risk of contracting pulmonary or cerebral oedema, the sickness of high altitude which fills the lungs or brain with fluids. This, at best, is incapacitating and at worst is fatal.” (1982, p. 179).
Emotions
Mosso also found that “states of emotional excitement affect the cerebral blood circulation far more conspicuously than does intellectual activity.” (Mosso, 2014, pp. 60–71).
Mosso may have noticed cerebral excitation with emotions at sea level, but at extreme altitude, emotions are usually dulled. He did not live long enough to witness the British attempts on Everest, but in The Fight for Everest 1924, leader EF Norton remarked that, “one is never elated at 23,000 feet; at these heights one's emotions are all in half tones.” (1925, p. 80). Surgeon T. Howard Somervell had found it hard to feel anger or anything else in 1922: “When at a height approaching 27,000 feet, I remember distinctly that I cared very little whether we reached the top of Everest or not.” (1922, pp. 305–306). A medical analogy from much later on K2 might explain it. Rick Ridgway portrayed emotions as “obscured in the anesthesia of twenty-seven thousand feet.” (1980, p. 266).
Sleep, Dreams, and Awakening
Mosso tried to distinguish blood flow shifts between the periphery and the internal workings of the brain in various situations, but he had difficulty evaluating sleep, chlorate hydrate-induced sleep, dreams, and awakening. With a paucity of data, he nonetheless concluded that the brain had “spontaneous fluctuations” in blood flow from “psychic-cerebral activities” (Mosso, 2014, pp. 74–91). There is also a paucity of accounts by climbers up high, other than their dreamy wishes to be back down low. For example, Eric Shipton, complaining about both his whole body and his head in the clouds, protests that “A climber on the upper part of Everest is like a sick man climbing in a dream.” (Tilman, 1948, p. 487).
Rather than overdoing this topic, the next section will focus on a different form of dreaming, so to speak. Hallucinations are distinguished from dreaming, which does not involve wakefulness. The word hallucination itself is derived from the Latin word alucinari meaning wandering mind.
Dull Brains, Hallucinations, and Mountaineers
Mountaineers are well-known for their dreaming about going to the mountains, but once at extreme altitude, even their daytime thoughts can become hypoxic dream-like states or frank hallucinations. Mosso would not be able to say much, but stories of hallucinations abound in the mountaineering literature. In a report of 70 cases in 24 subjects gleaned from literature and the internet, hallucinations were more likely to occur above 6000 m, last for minutes to hours, and have the following topics: presence of another person (36% of episodes and often correlated with an acoustic component), visual (32%), somesthetic (31%), or acoustic (25%) (Hüfner et al., 2014). According to their findings which, excluding an unspecified number with somatic symptoms, there were fewer than 10% with negative symptoms, disorganized thinking, or confusion. This is surprising. A viewpoint from another large but unpublished compendium (Lankford-Words From On High) is that such impairment is underrepresented because only survivors could write about it.
Despite this last opinion, benign or friendly mountaineer's hallucinations are, indeed, frequent. Perhaps the most famous hallucination was by Frank Smythe who got a lot of mileage out of it with his imaginary companion and mint cake story (Smythe, 1937, p. 633). In Everest the Hard Way, Scottish climber Dougal Haston confirmed the other-person imagery statistically associated by Hüfner with acoustic hallucinations:
While hallucinations make interesting reading, and at times might seem benign, the problem for a mentally-dysfunctional mountaineer is outright safety. In Dead Lucky. Life After Death on Mount Everest, Australian Lincoln Hall, who was indeed left for dead while descending from Everest in 2006, confesses that “I was no longer capable of distinguishing between the reality of the mountain and the fabrications of my mind.” (2007, p 153). He was lucky. Another version of this psychotic disconnect of the wandering brain and the wandering body up in the Death Zone is by mountaineer Tasker, warning of “my mind roaming independently of the automaton movement of my limbs.” (1982, p. 196).
1920–1930: Post-Mosso Research, and the Mountains
Mosso's inventions or modifications of equipment to study brain pulsations began the long technological journey to today's modern imaging techniques. Of course, there had been investigations by others. Examples include Charles Roy and Charles Sherrington who suggested a link between brain circulation and metabolism (1890). In the same year, famous psychologist William James acknowledged the work of Mosso while discussing the concept of brain blood flow variations during mental activities in his tome, Principles of Psychology (1890). However, research stagnated after Mosso's work, in part from lack of technological advance and in part from the conclusions of an influential Royal College of Surgeons professor, Leonard Hill.
Hill correctly recognized that intracranial cerebrospinal fluid pressure varied with cerebral venous pressure. However, he specifically and incorrectly disagreed with Mosso, stating that movements of the brain were solely of cardiac and respiratory origin and that the brain was not metabolically active compared to muscle (Hill, 1896, pp. 15, 73–76, 152–155). Long after Mosso's death in 1910, Hill atoned himself on a different project in 1920. He had advised Scottish chemistry lecturer, accomplished Himalayan mountaineer, and high altitude scientist Alexander Kellas to try not only heavy oxygen canisters on Kamet but also rubber bags containing oxylithe (sodium peroxide) that produce oxygen when water is added (West, 2003; Mitchell and Rodway, 2011, p. 171).
Hill was helpful on another but unrelated high altitude experiment. The term “glacier lassitude” itself had been coined by George Mallory (Lankford, 2014b), but the cause was unclear. Everest expedition medical officer Hingston (1925, pp. 254–255) had continued a moist-air theory, but back in London, Hill studied humans on a bicycle ergometer at a simulated height of about 20,000 feet (6100 m) with varying levels of humidity, finding that it was not contributory (Hill, 1925). The environmental thermal and hypoxemic origins of glacier lassitude on Everest were thus uncovered. Unfortunately, the three expeditions of 1921, 1922, and 1924 set new altitude records on Everest, but did not reach the summit, and Kellas, numerous porters, Mallory, and Irvine were lost.
In 1928, a medical serendipity occurred. Somewhat similar to the exposed brains of Mosso's subjects, changes in blood flow were observed in a subject with an abnormal visual cortex. John Fulton's subject had a vascular malformation with a bruit more noticeable after the stimulus of increased use of eyes after being in the dark (Fulton, 1928). In 1929, the human electroencephalogram (EEG), only in use for 5 years, showed a phase of slow-wave sleep (SWS). It was not until 1953 that rapid eye movement (REM) sleep was recognized, something Mosso may have seen a hint of in his recordings (Raichle and Shepherd, 2014, pp. xxv–xxvi). He had been curious about sleep patterns back in 1879, not from electrical measurements, but from respiratory, cardiovascular, and cerebrovascular pulse contours (Mosso, 2014, pp. 74–97).
As for mountaineers, sleep can be problematic. Here is Smythe again, this time at 23,300 ft (7100 m) on Kangchenjunga: “I for one slept badly, but a restless night was compensated to some degree by the dulling effects of altitude on the brain.” (Smythe, 1935, p. 177).
1930–1940: Oxygen
The British would launch four more official attempts on Everest in this decade. The first was in 1933 with the hallucinating Smythe, and physician C. Raymond Greene with his knowledge of physiology. He found old, partially-filled cylinders from 1922, and, “took a swig of oxygen. The first effect was a sudden increase in the light. I saw more sharply and colours became brighter.” (Greene, 1974, p. 159). The dullness and brightness he referred to was Greene's nod to physiologist Haldane, who “sat in his steel chamber with the pressure gradually rising towards the normal: and how, at a certain level, the electric light glowed suddenly more brightly. At first, he thought the current had been increased, but later he came to realise that the change was in himself.” (Greene, 1931, p. 338). Whether it was Haldane in the chamber, Greene on the mountain, or aviators in the sky, oxygen was salubrious.
By now, an easier way to see the summit was by the Houston Mount Everest Flight Expedition (Fellowes, 1934) funded by aviation buff Lady Lucy Houston, unrelated to the later familiar figure in high altitude medicine. Simple supplemental oxygen had already been used in aviation for some time. It was well known that in thin air, hypoxic psychomotor skills and poor decision-making would leave both pilots and climbers forever on the mountain. For even higher up, protection against physical dangers other than simple hypoxia would require balloonists, pilots, and eventually astronauts to use pressurized masks and then full suits. Above the Armstrong Limit at about 63,000 ft (19,200 m), named for space medicine pioneer Harry Armstrong, atmospheric pressure is so low that water in the blood, and the brain, boils at body temperature (Armstrong, 1939; Douglas, 1973, pp. xxi, 108–148).
1940–1950
World War II superceded climbing and research during this decade, but quantitative measurements of whole brain blood flow and metabolism in humans were performed by Kety and Schmidt (1948) who estimated that the brain, which relies almost exclusively on moment-to-moment delivery of glucose and oxygen, consumed a huge 20% of the body's energy, yet constituted only 2% of the weight. This was something Mosso had suggested qualitatively many years before (Raichle and Shepherd, 2014, p. xxi). That regional and local cerebral blood flow changes exist to support the metabolic demand of active neurons is today termed “functional hyperemia” or “neurovascular coupling” and includes an increasingly deeper recognition of neurotransmitter-mediated regulation (Attwell et al., 2010, Shih et al., 2012).
The war era must include mention of the 34-day hypobaric chamber experiment directed by Charles Houston named Operation Everest. (Houston, 1946; Houston and Riley, 1947a). With simulating slow and graded “ascent” that high, Houston suggested Everest could be climbed, although he did see that the men were blue and had undeniably dull brains (1947b). Mosso had also been that physically and mentally lackluster in his own chamber in 1898.
1950–1980: The Golden Age
In 1950, Annapurna was climbed by the French, beginning the golden age of Himalayan climbing with the first ascents of all 8000 m peaks by 1964. The Swiss had the Everest permission in 1952, and also felt the altitude. Climbing leader Rene Dittert joked, “I do not know if the brain can acclimatize itself, but I had the feeling that it would be a mistake to organize a chess tournament on the Khumbu.” (1954, p. 80). Swiss medical leader Edouard Wyss-Dunant minted the term Todeszone, or death zone, as about the height of the South Col (1953).
Tenzing and Raymond Lambert pushed farther, nearly reaching the South Summit of Everest. With dulled senses, Lambert admitted, “There was a confused impression of being on some other planet.” (Dittert et al., 1954, p 152). The following year, 1953, the same year that Houston and all but one of his team survived their famous tumble down K2, Tenzing and Hillary had reached the top of Everest.
A golden era also opened for technological leaps in the study of the central nervous system. Raichle and Shepherd (2014, p. xviii) give a timeline of these developments: regional brain blood flow in animals and humans correlated with behavior in 1955–1963; regional oxygen consumption measured in humans in 1970; computerized tomography (CT) in 1973; positron emission tomography (PET) in 1975; and magnetic resonance imaging (MRI) in 1979.
Near the end of that incredible stretch, in 1978, Reinhold Messner and Peter Habeler would prove true the 1920 predictions of Kellas, both the climbing rate and the summiting of Everest “by fair means,” a climbing term used by Alfred Mummery in the 1880s but later evolved by others to mean without supplemental oxygen. Messner would describe himself as “nothing but a single narrow gasping lung,” and in keeping with the theme of this article, “My mind is disconnected.” (1999, p.180). Dull brains, indeed.
1980s and Beyond: A Final Tribute to Angelo Mosso
Mountaineers would get a headache just thinking about these concluding modern remarks. That was certainly true in the anti-science sentiment of many in the climbing community of Mallory's day. He himself would say about Everest that medical tests “are of no value in determining where precisely on that other hill of unrivalled altitude persevering man will be brought to a standstill.” (Mallory, 1922).
The timeline of the advance of technology continues in Raichle and Shepherd's commentary (2014) with functional imaging with PET and blood flow in 1982, test analysis by image subtraction, stereotaxic image normalization, and image averaging in 1984–1990, and The Program in Cognitive Neuroscience in 1987. In the 1990s, blood-oxygen-level-dependent (BOLD) contrast functional MRI (fMRI) and event-related fMRI would transform studies of brain function.
Mosso became aware of ongoing or intrinsic brain metabolism. Current-day intrinsic functional studies reveal that this activity consumes most of the brain's energy budget compared to task-evoked utilization (Raichle and Shepherd, 2014, p xxv). Studies of the neurophysiology and biochemistry of brain imaging signals continue the march of technology. With ever more powerful expertise, it is possible to have blood flow resolution down to two-photon microscopy levels (Shih et al., 2012). Mosso is given supreme credit by Raichle and Shepherd (2014, p. xxiii) for his work over a century ago: “At these levels, Mosso's early vision merges with modern cellular and molecular brain studies.”
Conclusion
In his own way and time, Angelo Mosso was on the right track about brains and cerebral blood flow. Modern medicine and technology has a much better but still evolving understanding of the body at high altitude. The misery of hypoxic and dull brains described in the writings of the high altitude pioneers helps to tell the story in an equally unique but more evocative manner, both in terms of the mountaineering literature and illustration of some of the high altitude illnesses and physiology.
Footnotes
Acknowledgments
At times up high, the author and Remi Sojka had one brain between the two of them. At sea level, Erik Swenson had all of his.
Author Disclosure Statement
The author has no conflict, funding, or affiliation to report.