
Abstract
Abstract
Havryliuk, Tatiana, Bhuwan Acharya, Emily Caruso, and Tracy Cushing. Understanding of altitude illness and use of pharmacotherapy among trekkers and porters in the Annapurna region of Nepal. High Alt Med Biol 16:236–243, 2015.—We surveyed Nepali porters and guides as well as English- and non-English-speaking trekkers on their knowledge of altitude illness and its treatment during trekking expeditions to the Annapurna region of Nepal. From March 15 to April 15, 2014, Nepali porters and visiting trekkers were surveyed regarding their ability to recognize and treat altitude illness in Manang, Nepal (3540 m). Their personal use of medications and home remedies and presence of acute mountain sickness (AMS) symptoms were also assessed. 504 subjects were surveyed, including 108 Nepalis. Overall incidence of AMS symptoms was 16%, 5% among Nepalis, and 21% among trekkers. Subjects recognized that headache (88%) was one of the symptoms of AMS, however many reported not knowing the symptoms of high altitude pulmonary edema (40%) or high altitude cerebral edema (42%). 58% of subjects reported carrying and 16% reported taking acetazolamide, while only 2 (0.4%) respondents took dexamethasone. The majority of subjects reported that they would be able to recognize (67%) and treat (62%) altitude illness. Trekkers reported a higher incidence of AMS symptoms than Nepalis. Although most respondents recognized symptoms of AMS, both Nepalis and trekkers lacked knowledge regarding more serious presentations of altitude illness, thus both groups were overconfident in their ability to recognize and treat altitude illness.
Introduction
T
The rate of ascent and the maximum altitude attained are the main factors determining the development of altitude illness. Acute mountain sickness (AMS) is characterized by headache, fatigue, anorexia, sleep disturbances, and lightheadedness in unacclimatized persons after recent ascent to greater than 2500 m (Hackett and Roach, 2012). Ten to 25% of unacclimatized individuals develop AMS when traveling to moderate altitude of 2500 m in Colorado, U.S. (Honigman et al., 1993). About half of trekkers in Nepal ascending to altitudes of 4000 m over 5 or more days develop AMS (Hackett et al., 1976).
A recent study found that 48% of trekkers crossing Thorung La pass (5400 m) experienced AMS (defined by Lake Louise Severity Score ≥3), a decrease from the incidence found in prior studies at this site; authors attributed this finding to slower ascents and use of prophylactic medications (McDevitt et al., 2014). The incidence of AMS increases to 85% when unacclimatized subjects fly directly to 3860 m (Hackett and Rennie, 1979).
Given the recent construction of a road facilitating access to faster ascent, altitude illness has become more of a concern on the Annapurna Trekking Circuit in Nepal. The road allows travelers to ascend to altitudes >3000 m in one or two days, increasing the risk of altitude illness. Overall rates of more dangerous illnesses such as high altitude cerebral edema (HACE) and high altitude pulmonary edema (HAPE) are estimated to be at 0.5%–1% and 0.2%–15% depending on ascent rate and final altitude (Bartsch and Roach, 2011; Bartsch and Swenson, 2013; Bartsch et al., 2002).
Incidence of AMS among Nepali porters and guides has a wide range, but most studies report a decreased incidence as compared to foreign trekkers. In a study conducted at Machermo in the Khumbu region of Nepal, 21% of trekkers and 8% of porters reported AMS symptoms at 4470 m (Newcomb et al., 2011). Many porters reside at higher elevation than trekkers, and porters surveyed later in the trekking season might have been better acclimatized. Hillenbrand et al. (2006) found an incidence of 11.9% of AMS among porters trekking to Lobuche at 4930 m. Another study found 45% of Sherpas climbing to extreme altitudes averaging 5500 m reported experiencing at least one symptom of AMS (Droma et al., 2007).
Recognizing early symptoms and signs of AMS, HACE, and HAPE is fundamental to instituting timely treatment and preventing devastating outcomes, thus prior knowledge of altitude illness is an important asset for at risk trekkers and porters in high altitude regions. Vardy et al. (2005) found that trekkers who chose safe ascent options as answers to questions regarding AMS tended to ascend more slowly and were less likely to develop AMS than the group with a more aggressive approach, suggesting that education on risk factors for AMS might play a role in prevention. Based on their two-question survey, Newcomb et al. (2011) concluded that “both trekkers and porters demonstrated appropriate knowledge of actions to be taken in response to altitude illness.” However, 30% of the respondents chose to delay descent in a HACE/HAPE scenario, which could be lethal in a real situation.
McDevitt et al. found that only 42% of surveyed trekkers in Nepal had an “elementary knowledge” about the risk and prevention of AMS based on responses to two questions (McDevitt et al., 2014). Trekkers' recognition of altitude-related illnesses and knowledge of basic treatments could be life-saving in remote high altitude regions. However, little is known about what prior altitude education trekkers have, the sources of their information, and their confidence in recognizing and treating altitude illness. Even more limited are data on the knowledge of altitude illness among Nepali porters and guides as well as non-English-speaking trekkers.
Trekkers' and porters' use of medications and herbal remedies at high altitude and their understanding of potential dangers have been poorly studied. McDevitt et al. (2014) found that 44% of English-speaking trekkers were using acetazolamide during their climb over 5400 m Thorung La pass, while 1% used dexamethasone. Recent debate over the use of steroids among mountaineers to enhance performance and to prevent altitude illness, particularly at extreme altitudes, underscores the need to assess users' knowledge about their potential dangers, such as life-threatening adrenal suppression (Bancos et al., 2015; Dinsen et al., 2013; O'Neil, 2013; Robert et al., 1979). Data are also lacking on use of pharmacotherapy among non-English speaking trekkers and Nepalis, as well as consumption of food supplements and herbal remedies for altitude illness prevention.
We surveyed English and non-English speaking trekkers and Nepali porters and guides in Manang, Nepal (3540 m) on their knowledge of altitude illness presentation, prevention, and treatment, as well as their pharmacotherapy practices.
Materials and Methods
This study was approved by the Colorado Multiple Institutional Review Board (COMIRB) and Nepali Health Research Council.
Between March 15, 2014 and April 15, 2014, trekkers, porters, and guides trekking on the Annapurna Circuit in Nepal were asked to participate voluntarily in a survey regarding their knowledge of altitude illness and their use of pharmacotherapy for its treatment and prevention. Trekkers completed surveys prior to the daily altitude illness lecture given at the Himalayan Rescue Association (HRA) aid post in Manang (3540 m). Porters and guides were recruited in nearby teahouses as they rarely attend the lecture. Surveys were administered in English, Nepali, Hebrew, French, Spanish, and Russian languages to capture as many subjects as possible. Choice of the languages was based on the epidemiology of visitors in the McDevitt et al. (2014) Manang study and the facility of obtaining translations. Inclusion criteria included all trekkers, porters, and guides, ages 18 or older that were able to read and write in one of the above languages.
The survey consisted of four parts. Part one asked for demographic information, pre-departure medical consultation, and prior and current experience of AMS symptoms. Part two assessed subjects' ability to recognize symptoms of AMS, HACE, and HAPE and tested their knowledge about commonly held beliefs about altitude illness. Part three focused on the knowledge and use of medications, food supplements, and herbal remedies to prevent and treat altitude illness. Part four surveyed subjects' confidence in being able to recognize and treat altitude illness and the source of their altitude education. The survey in English can be viewed in Appendix A.
Data were entered manually into an Excel database (Microsoft Excel, Microsoft Corporation, Inc., Redmond, WA) and transferred into SAS format. Statistical analyses were performed using SAS Enterprise Guide 4.3 (SAS Institute, Inc., Cary, NC). Partially answered surveys were included in the analysis.
Comparisons were made between Nepali and non-Nepali respondents regarding presence of symptoms consistent with AMS, use of pharmacotherapy, overall understanding of altitude illness, and confidence in recognizing and treating it. All data are reported using descriptive statistics; differences between continuous variables are expressed as medians with 95% confidence intervals (CIs) and categorical variables expressed as percentages with 95% CIs. No adjustments were made for multiple comparisons.
Results
A total of 504 surveys were filled out by trekkers, porters, and guides during the one-month study period. During the same time period, 699 trekkers attended the altitude lecture at the HRA aid-post, thus we surveyed 58% of HRA lecture attendees. Approximately 100 surveys were administered at local teahouses to capture Nepali subjects.
Out of 504 completed surveys, 244 were in English, 91 in Nepali, 76 in Hebrew, 51 in French, 22 in Spanish, and 20 in Russian. Respondents came from 37 different countries, with Nepal and Israel being the most common (Appendix B). The majority of subjects were male (64%), and most (93%) were surveyed on their ascent of the Annapurna Circuit toward Thorung La Pass (5400 m). The median home altitude for Nepali respondents was 1500 m, while it was 100 m for non-Nepalis. Nepali respondents more frequently reported seeking medical consultation prior to trekking than non-Nepali respondents (Table 1).
AMS symptoms
381 subjects (76%, 95% CI: 72%–79%) reported they had never experienced AMS (Table 2). When asked if AMS symptoms were present at the time of the survey, only 54 (11%, 95% CI: 8%–14%) responded affirmatively and 64 (13%) were uncertain. Respondents indicating they were experiencing AMS symptoms or were unsure were then asked to list the symptoms that were present (Fig. 1). Among these 118 individuals, 95 (81%) reported their symptoms and 79 were found to have symptoms consistent with AMS. The overall rate of current symptoms consistent with AMS among respondents was 16% (95% CI: 13%–19%), with a rate of 5% (95% CI: 2%–10%) among Nepalis and 21% (95% CI: 17%–25%) among trekkers.
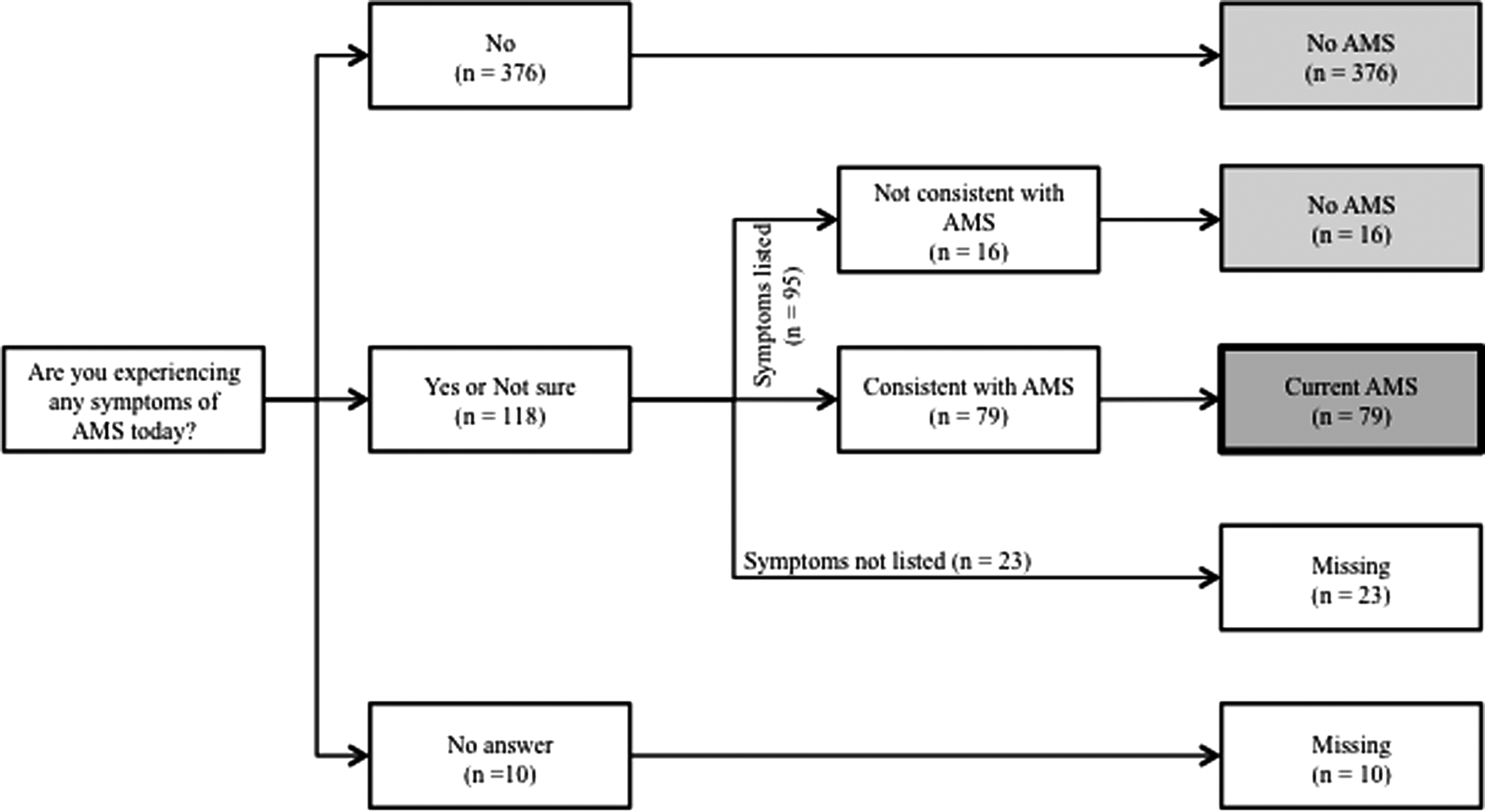
Flow diagram of respondents reporting of current symptoms associated with acute mountain sickness (AMS).
These symptoms include: headache, dizziness, fatigue, lack of appetite, poor sleep, nausea, and vomiting.
†These symptoms include: breathlessness, unsteadiness/coordination problems, chest pain, diarrhea, digits tingling, elevated heart rate, fever, finger swelling, cold symptoms, otalgia, face tingling, and cough.
Knowledge of AMS, HAPE, and HACE presentation
The majority of subjects correctly identified the symptoms of AMS, with 443 (88%, 95% CI: 85%–91%) listing headache as one of them. Overall, the Nepali group was less likely to choose correct symptoms. A large number of respondents reported that they did not know the symptoms for HACE or HAPE (Table 3).
Pharmacotherapy and other remedies
The most common medication carried was acetazolamide (58%, 95% CI: 53%–62%), while only 81 (16%, 95% CI: 13%–20%) reported currently taking this medication. Two respondents reported taking dexamethasone (0.4%, 95% CI: 0%–1%). Garlic, ibuprofen, and coca homeopathy were also common. Figure 2 represents the distribution of medications, supplements, and herbal remedies that respondents were carrying and taking at the time of the survey. There was no significant difference between Nepalis and trekkers in their use of acetazolamide, dexamethasone, ibuprofen, and garlic (Table 4).
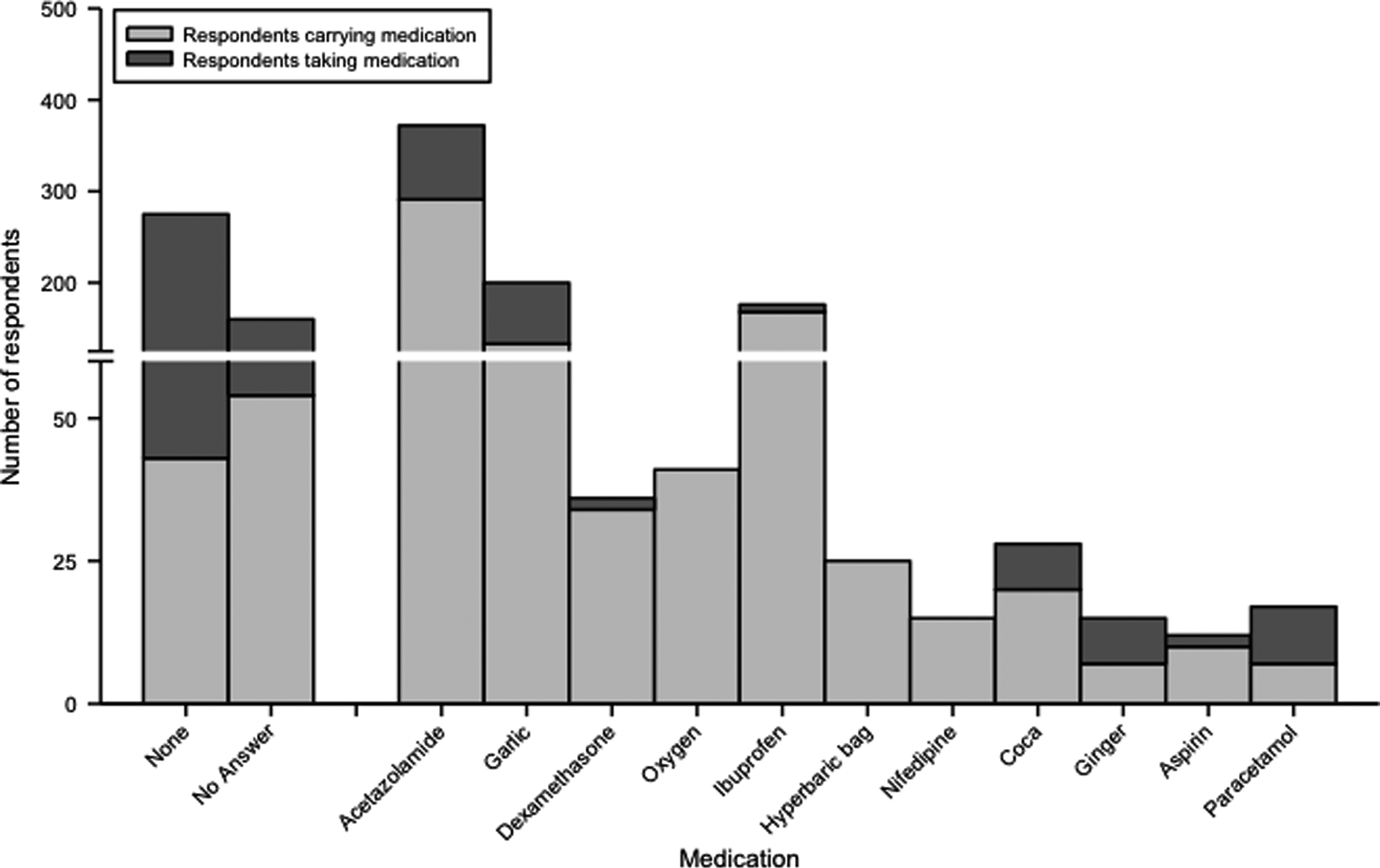
Medications and other remedies carried and used by trekkers and porters.
Treatment knowledge
Most trekkers (79%; 95% CI: 74%–83%) and Nepalis (66%; 95% CI: 56%–75%) answered correctly that descent was the most definitive treatment for altitude illness (Fig. 3). Many respondents (430, 85%; 95% CI: 82%–88%) did not know or answered incorrectly when asked if the following statement was true: “Taking dexamethasone for more than one week and then stopping it abruptly can have life-threatening effects.” Among the 34 respondents who reported that they were carrying dexamethasone, 12 (35%; 95% CI: 20%–54%) provided the correct answer that taking dexamethasone could be dangerous.
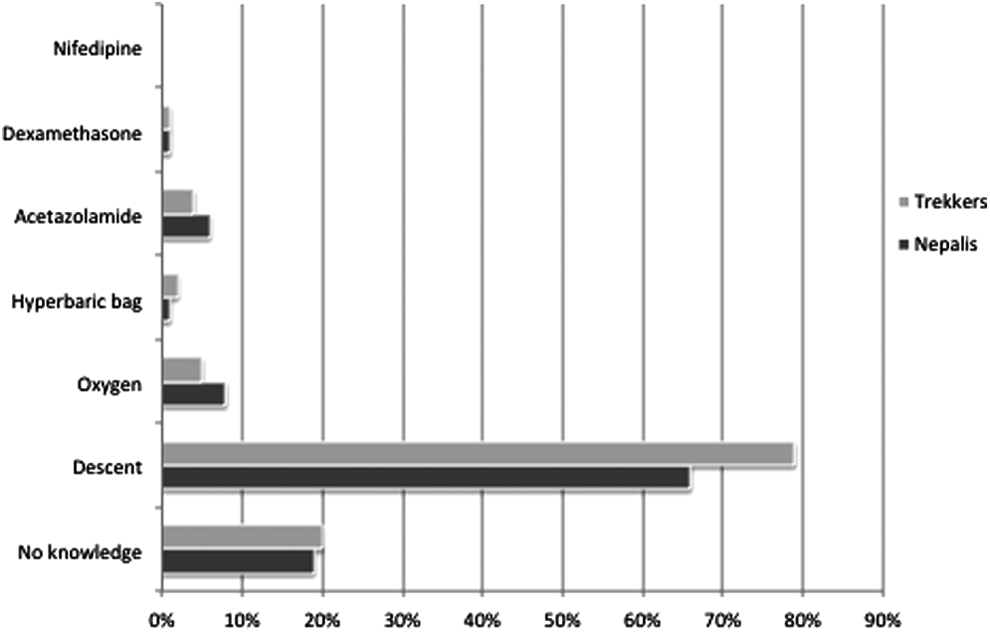
Knowledge of altitude illness treatment.
Sources of altitude education
Subjects listed the Internet, friends and colleagues, and guide books as the top three sources for learning about altitude illness (Fig. 4). Both Nepali and non-Nepali respondents reported using these sources; however a slightly higher proportion of trekkers reported the Internet as their primary source of knowledge (47% vs. 39%, difference −8%; 95% CI: −19%– 2%). More trekkers than Nepalis learned from medical providers (27% vs. 16%; 95% CI: −20%–3%).
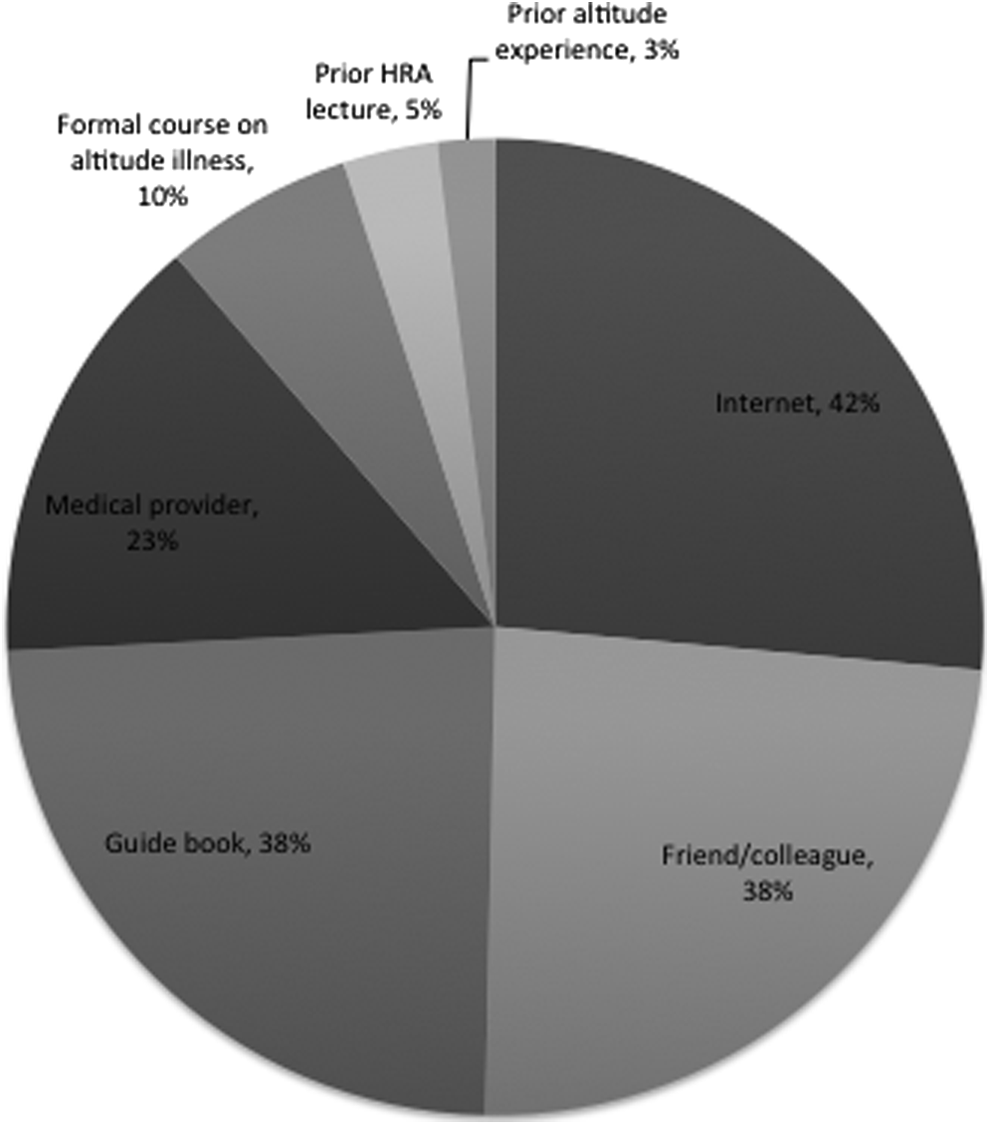
Sources that subjects used to learn about altitude illness prior to the trek. Less than of 1% subjects reported the following sources: prior AMS, medical studies, biology course, books, university, first aid talk, guide training, wilderness first responder and emergency medical technician training, flyers, TV programs, and guide.
Confidence in ability to recognize and treat altitude illness
The majority of subjects reported they would be able to recognize symptoms of altitude illness (67%; 95% CI: 63%–72%) and be able to treat it (62%; 95% CI: 58%–66%). There was no significant difference between Nepali and trekker groups.
Among the respondents who were unsure whether they had any current AMS symptoms, most reported they would be able to recognize (47/64, 73%; 95% CI: 61%–84%) and treat (38/64, 59%; 95% CI: 46%–71%) themselves and others for AMS. Out of this “unsure” group, more trekkers indicated that they would be able to recognize and/or treat AMS symptoms than Nepalis did (Table 5).
Role of trekking companies in education
Of the 228 trekkers that reported using a guide during their trek, 148 (65%) were educated on altitude illness prior to start of the trip. Of the 80 trekkers that did not receive any altitude education by their guides, 69 (86%) believed that they should have been informed about altitude illness by their guide.
Discussion
While limited data exist on the extent of knowledge that trekkers, guides, and porters have on altitude illness in the Nepali Himalaya, the prevalence of AMS may be as high as 48% in trekkers crossing the popular Thorung La Pass at 5400 m (McDevitt et al., 2014). Our study expands on this prior research which found that less than half of trekkers had “rudimentary” knowledge of AMS, and attempts to quantify trekkers' and porters' confidence in their ability to recognize and treat altitude illness as well as to assess the sources of their altitude education.
Nepali subjects reported lower incidence of AMS symptoms at 3540 m as compared to the trekkers in the study (5% vs. 21%), which is consistent with prior reports (Newcomb et al., 2011). Likely explanations for this finding include Nepali subjects' higher home altitude than trekkers' by 1200 m, acclimatization during prior treks during the season, and possible genomic adaptations to high altitude. It is known that porters also come from the lowland region of Terai (67 to 300 m elevation) and are likely to be at a higher risk of AMS than the porters from higher areas of Nepal.
Most subjects recognized the symptoms of AMS, with 88% listing headache as one. However, 42% and 40% reported not recognizing more dangerous conditions like HACE and HAPE. Consistent with prior studies, only 70% knew that descent was a definitive treatment for altitude illness (Newcomb et al., 2011). Nepalis showed a trend toward having less knowledge of altitude illness as compared to trekkers. Furthermore, our data suggest that respondents are overconfident in their ability to recognize and treat altitude illness given that the individuals who were unsure of having AMS symptoms still thought they could recognize (73%) and treat (59%) altitude illness.
Our pharmacology data were consistent with other studies showing that 16% of subjects were taking acetazolamide. We found that some trekkers, particularly those from France, were taking coca homeopathy, which has not been rigorously studied for AMS prevention and is not recommended by any major organizations. Likewise, many Nepalis and trekkers ingested garlic, which has not been shown to be helpful for prevention or treatment of AMS, and has been associated with higher rates of AMS among pilgrims in Nepal (Luks et al., 2010; Morris et al., 2013; MacInnis et al., 2013). Although a few people carried steroids such as dexamethasone (34 subjects), only a third of those were aware that steroids might have dangerous side effects if used for longer than 1 week. A small number of subjects reported learning about altitude illness from medical providers; thus the Internet and guidebooks, which currently serve as the main sources of information used by both Nepalis and trekkers, should be targeted to improve the quality of altitude illness education. In addition, guide services that do not currently educate their participants about altitude illness should be encouraged to do so.
There are potential limitations to our study. The survey method has inherent recall bias. It is possible that our subjects misreported the incidence of prior AMS, as well as details about preparation for their trek.
Although we used native speakers to translate the survey, questions might still be misunderstood due to language intricacies. Further cultural barriers also remain, such as when surveys were distributed in local teahouses, subjects tended to congregate together and discuss their answers despite being asked not to do so. Furthermore, for ease of data analysis and description we assumed that all Nepalis surveyed were guides or porters, but a small number from this group could have also been trekking for pleasure. This study unfortunately excluded illiterate porters, who may represent a group with less education in general and who know less about altitude illness than the sampled group.
On the other hand, trekkers with a lot of altitude experience or those traveling with commercial groups that provided altitude training might have opted to not attend the HRA lecture, thus skewing our results toward less informed subjects.
Data on the dosage of medications were solicited but not provided by most subjects, thus limiting further analysis.
Conclusion
Our study found that Nepali porters and guides a have lower incidence of AMS symptoms than trekkers. Both groups have satisfactory knowledge about AMS, but considerable lack of knowledge about the more dangerous conditions HACE and HAPE, with Nepalis showing a trend toward less knowledge. Our subjects reported significant use of herbal remedies like garlic and coca homeopathy to prevent altitude illness. Overall, trekkers and porters were overconfident in their ability to recognize and treat altitude illness and more rigorous education is required to keep travelers safe in the Nepali Himalaya.
Footnotes
Acknowledgments
Many thanks to the Himalayan Rescue Association (HRA), Dr. Buddha Basnyat, HRA volunteer physicians (Michael Wu and Frith Dollimore), and survey translators (Gobi Bashyal, Prakash Adhikari, Anne Stey, Addi Feinstein, Keren Rabinowitz, and Lidiya Gavrilyuk).
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.