
Abstract
Abstract
Steier, Joerg, Nic Cade, Ben Walker, John Moxham, and Caroline Jolley. Observational study of neural respiratory drive during sleep at high altitude. High Alt Med Biol. 18:242–248, 2017.
Aims:
Ventilation at altitude changes due to altered levels of pO2, pCO2 and the effect on blood pH. Nocturnal ventilation is particularly exposed to these changes. We hypothesized that an increasing neural respiratory drive (NRD) is associated with the severity of sleep-disordered breathing at altitude.
Methods:
Mountaineers were studied at sea level (London, United Kingdom), and at altitude at the Aconcagua (Andes, Argentina). NRD was measured as electromyogram of the diaphragm (EMGdi) overnight by a transesophageal multi-electrode catheter; results were reported for sea level, 3,380 m, 4,370 m, and 5,570 m.
Results:
Four healthy subjects (3 men, age 31(3)years, body mass index 23.6(0.9)kg/m2, neck circumference 37.0(2.7)cm, forced expiratory volume in 1 second 111.8(5.1)%predicted, and forced vital capacity 115.5(6.3)%predicted) were studied. No subject had significant sleep abnormalities at sea level. Time to ascent to 3,380 m was 1 day, to 4,370 m was 5 days, and the total nights at altitude were 21 days. The oxygen desaturation index (4% oxygen desaturation index [ODI] 0.8(0.4), 22.0 (7.2), 61.4 (26.9), 144.9/hour, respectively) and the EMGdi (5.2 (1.9), 12.8 (5.1), 14.1 (3.4), 18.5%, respectively) increased with the development of periodic breathing at altitude, whereas the average SpO2 declined (97.5 (1.3), 84.8 (0.5), 81.0 (4.1), 68.5%, respectively). The average EMGdi correlated well with the 4%ODI (r = 0.968, p = 0.032).
Conclusion:
NRD sleep increases at altitude in relation to the severity of periodic breathing.
Introduction
R
Neural respiratory drive (NRD), as measured by the electromyogram of the diaphragm (EMGdi), is closely correlated with breathlessness (Reilly et al., 2011; Jolley et al., 2015; Jolley and Moxham, 2016) and can be recorded breath by breath while patients are asleep (Steier et al., 2010; Xiao et al., 2014).
We hypothesized that sleep-disordered breathing at altitude is closely correlated with NRD, and that high levels of NRD would lead to increasing numbers of apneas and a greater severity of sleep-disordered breathing with ascent to high altitude.
Participants and Methods
This study was planned as part of a program to assess “NRD in cardiopulmonary conditions and normal subjects,” and it was approved by the local research ethics committee at King's College London, United Kingdom (Reference No: 05/Q0703/82; V3-21/02/2006). Informed written consent was obtained from all participants before inclusion in the study.
An expedition to the Aconcagua, Argentina (peak altitude 6,962 m), was planned to assess NRD in asleep healthy volunteers. For this purpose, four mountaineers were recruited and initially studied in the sleep laboratory at sea level (King's College Hospital, London, United Kingdom). Exclusion criteria were any medical condition that could put participation during a mountaineering expedition at altitude at risk; only young healthy subjects were recruited. We recorded demographics, spirometry, full polysomnography, tests of respiratory muscle strength, and baseline recordings of the EMG of the diaphragm and the parasternal intercostal muscles. The equipment was taken for a test to the International Foundation High Altitude Research Station Jungfraujoch, CH (November 2007; altitude 3,450 m). The expedition to the Aconcagua started in December 2007 and finished at the end of January 2008, ascending via Confluencia (3,380 m), Plaza de Mulas (4,370 m), Camp Canada (5,050 m), Camp Alaska (5,200 m), and Nido de Condores (5,570 m); however, overnight sleep studies were performed at 3,380 m, 4,370 m, and 5,570 m only. For reasons of safety, a stop of at least 2 days at each level of altitude was planned. All mountaineers passed a medical examination before commencing the climb and again at Plaza de Mulas (4,370 m), none showed any of the following signs or symptoms of altitude sickness or pulmonary edema:
Symptoms:
• Difficulty in breathing at rest • Cough • Weakness or decreased exercise performance • Chest tightness or congestion
Signs:
• Crackles or wheezing in at least one lung field • Central cyanosis • Tachypnea • Tachycardia
The recording equipment stopped working after the 1st night at Nido de Condores (5,570 m), and only one sleep study (subject JS) could be obtained.
Demographics
At baseline, age (years), gender (male/female), height (m), and weight (kg) were recorded, and body mass index (BMI) was calculated (kg/m2). To assess the risk of sleep-disordered breathing, neck circumference (cm) was measured by using a standard tape measure.
Spirometry
Baseline spirometry was recorded after calibration of the equipment by using a 3 L syringe (Vitalograph®, Buckingham, England), seated with a noseclip on, and by using a tube mouthpiece. The recording spirometer was a Vitalograph Gold Standard (Vitalograph). The participants were asked to breathe in slowly to total lung capacity (TLC) and then to blow out as fast and hard as they could to measure the forced expiratory volume in 1 second (FEV1) and the forced vital capacity (FVC). The maneuvers were repeated at least five times, until consistent results were obtained according to American Thoracic Society/European Respiratory Society (ATS/ERS) criteria for the standardization of spirometry (Miller et al., 2005).
Respiratory muscle tests
Tests of inspiratory and expiratory muscle strength were performed following baseline spirometry. The participants were seated and for the mouth pressure measurements a flanged mouthpiece was used, with a noseclip on; for the sniff pressure measurement, a sniff plug was inserted into one nostril (Heritier et al., 1994). The maximum inspiratory mouth and the sniff nasal pressures were recorded from functional residual capacity, whereas the maximum expiratory mouth pressure was recorded from TLC. A handheld portable pressure meter (MicroRPM® Respiratory Muscle Testing; Carefusion®, Basingstoke, United Kingdom) was used to record the pressures.
Polysomnography
A full polysomnography was performed by using Alice5® equipment (Respironics®, Murrysville, PA) at sea level. Electrical activity of the brain (EEG) was measured with surface electrodes (Gold); according to the ten-twenty system, we recorded F4/M1, C4/M1, and O2/M1. Sleep and respiratory events were scored with standard terminology (Iber et al., 2007). Electro-oculography was measured by Gold surface electrodes to detect rapid eye movements. A position electrode measured on which side the patient was lying. Pulse oximetry sensed the oxygen saturation and heart rate. Airflow was detected via a nasal cannula (sensing pressure) and an oronasal thermistor. Abdominal and chest wall movements were detected via uncalibrated inductance plethysmography bands around the chest and abdomen. Apneas were defined as no airflow for >10 s; hypopneas were defined as periods of reduced airflow <50% from baseline for >10 s. Obstructive episodes were scored if there was ongoing inspiratory effort measured during apneas or hypopneas; the events were scored as central if ventilatory effort was absent. Respiratory effort-related arousals were scored if an arousal occurred after a period of >10 s with an increased inspiratory effort that did not meet the criteria of apnea or hypopnea.
Pulse oximetry
During ascent to altitude, pulse oximetry (Nonin Medical, Inc.®, Plymouth, MN) recorded an average of 30.5 (4.3) hours for the subjects. Each mountaineer had an overnight pulse oximetry combined with EMG recordings at 3,380 m and at 4,370 m, recording was only possible in one mountaineer at 5,570 m. The data were analyzed on return to London and average oxygenation (SpO2), nadir, and the 4% oxygen desaturation index (ODI) were calculated.
Electromyography
A multipair electrode catheter (Yinghui Medical Tech Ltd®, Guangzhou, China) was inserted via one nostril to record the transesophageal EMGdi, as previously described (Luo et al., 2008; Steier et al., 2010), connected to RA-8® amplifiers (Yinghui Medical Tech Ltd.®, Guangzhou, China) that further transmitted the signal to an analog-to-digital converter, Powerlab® 16/30 running Chart® Version 5 (ADInstruments®, Colorado Springs, CO).
The EMG of the neck muscles, parasternal intercostals, and abdominal muscles was recorded by using surface electrodes (Kendall Arbo®; Tyco Healthcare®, Neustadt, Germany) from standard positions (White et al., 1995; Maarsingh et al., 2000; Konrad et al., 2001; Duivermann et al., 2004; Lasserson et al., 2006). The surface electrodes were positioned on the sternocleidomastoid (neck) muscle bilaterally 2 cm above the clavicle and 3 cm beneath the mastoid process (EMGneck). A reference electrode was placed on the skin 6 cm lateral to the midline below the clavicles. For recording the EMG of the parasternal intercostals (EMGpara), electrodes were placed on each side of the sternum 3 cm from the midline in the second intercostal space (Reilly et al., 2011). The EMG of the abdominal muscles (EMGabdomen) was recorded from electrodes that were 2–3 cm lateral to the umbilicus bilaterally over the region of the rectus abdominis.
The EMG was recorded during resting breathing and during the maneuvers that have been described to achieve maximum or close-to-maximum activation of the diaphragm; while breathing in to TLC (TLC maneuver); and while breathing in as hard as possible against a closed airway (PImax maneuver), maximal sniffs, and maximum voluntary ventilation for 15 s (“sprint MVV”). In addition, EMG was recorded during maximal expiration against an occluded valve (PEmax maneuver). Maneuvers were repeated until consistent results were achieved, at least five times, and the maximum of all maneuvers was then selected to represent 100% activity. The recordings of the spontaneous EMG were sampled at 1 kHz, and EMG data were filtered with a high-pass 30 Hz and an additional low-pass 1 kHz filter. The rectified signals of the EMG (root-mean-square of the raw data) were quantified and transformed into percentage of maximum activity (as derived from the maximum inspiratory and expiratory maneuvers described earlier).
The equipment was powered by two Victron Energy AMG GEL 12–35 batteries (120 Ah; Victron Energy, Nuneaton, United Kingdom) that were connected to a Phoenix Inverter 12/350/Blue Power Charger 45–65 Hz, 200 W 12 V/15A (Victron Energy), and it was charged by six standard flexible outdoor solar panels (560 × 1490 mm, 12 V/140 W).
All EMG channels (diaphragm, neck, parasternal, abdomen) were recorded at sea level. At altitude, the EMG of the diaphragm (transesophageal), the parasternal intercostals, and the abdominal muscles (surface EMG) were recorded and analyzed. The placement of the transesophageal multipair electrode catheter allows the recording of five channels around the electrically active region of the diaphragm. The positioning of the esophageal catheter is such that channel 1 and channel 5 provide the largest recorded signals, which are then selected for analysis (root-mean-square, time constant 100 ms of the peak signal), as previously described (Luo et al., 2008, Steier et al., 2010). The “absolute level of NRD” is defined as the recorded percentage of maximum activity allowing the comparison of levels of drive between different subjects and different conditions, as described by our group (Jolley et al., 2009; Luo et al., 2009; Steier et al., 2010; Reilly et al., 2011) and others (Sinderby et al., 1998). To obtain an average of the NRD, each nonperiodic breath during a 1 minute period at the end of each 10 minute period at night was analyzed and included, if variability of the signal was less than 25% from baseline. These 1 minute data blocks were summed, and the mean of the sum of these values was taken for the whole night to calculate the average level of NRD (baseline).
The occurrence of cyclical changes in a biosignal, for example, not only during periodic breathing but also commonly observed during obstructive sleep apnea, makes analysis difficult. It requires the description of an average baseline and of the deviation from that baseline. In respiratory sleep medicine, this is achieved by reporting the average nocturnal SpO2 and the number of desaturation events (ODI). In the analysis of the EMG signals, a similar approach was achieved by providing the average EMG between apneas to provide the baseline and the slopes of the EMG signal (decrescendo, crescendo) both before and after central apneic events, as previously described in other forms of sleep-disordered breathing (Luo et al., 2009; Steier et al., 2010), as well as the index of respiratory events.
Outcome parameters
To define the correlation between NRD and sleep-disordered breathing, the level of NRD, as measured by the EMGdi (%max), was recorded at each level of altitude and differential respiratory muscle recruitment, as expressed by the EMG activity of different muscle groups, was further correlated to abnormal breathing patterns. Other outcomes were the apnea threshold of NRD and the EMGdi that was associated with central sleep apneas, as well as the oxygen desaturation index (4% ODI), the mean and nadir nocturnal SpO2, and the surface EMG of the parasternal intercostal and abdominal muscles. Sleep studies with recordings of the EMG and nocturnal pulse oximetries were performed the first night when ascending to a new altitude. Time to ascent to 3,380 m was 1 day, to 4,370 m was 5 days, and to 5,570 m was 13 days; the total of nights spent at altitude was 21 days.
Statistical analysis
SPSS® Version 20.0 (SPSS,® Inc, Chicago, IL) was used for the analysis. Results are reported as mean (standard deviation [SD]) for all normally distributed test results, and results represent the average data of the first night at a new altitude. The small sample size of the group with multiple comparisons at different altitudes precluded the use of many statistical tests and, instead, we decided to report the 95% Confidence Interval (95% CI) to provide information about overlap of the group's means. Significance was accepted with a p-value <0.05.
Results
Four healthy mountaineers were studied at sea level and during ascent to altitude. The group was young, predominantly male, normal in weight, and without any obvious respiratory abnormalities (Table 1).
Demographics of participants (n = 4). Except for the gender ratio, data are presented as mean (SD; 95% CI).
BMI, body mass index; CI, confidence interval; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; SD, standard deviation.
The global inspiratory, diaphragm, and expiratory muscle strength was normal. Respiratory muscle EMG recordings revealed diaphragm and parasternal activity while awake similar to that observed in normal subjects (Steier et al., 2010), as well as low neck muscle and expiratory muscle activity (Table 2).
Respiratory muscle strength and activity while awake at sea level. Data are presented as mean (SD; 95%CI).
EMG, electromyography; PEmax, maximum expiratory mouthpressure; PImax, maximum inspiratory mouthpressure; Psniff, nasal, maximum inspiratory sniff nasal pressure.
The polysomnography at sea level revealed a short sleep time with preserved sleep architecture and a relatively normal sleep efficiency. There were no respiratory abnormalities, no significant apneas or hypopneas, and no hypoventilation (Table 3).
Results of the polysomnography at sea level (London, United Kingdom; 0 m). Data are presented as mean (standard deviation; 95%CI).
TST, total sleep time; REM, rapid eye movement sleep; SE, sleep efficiency; SpO2, oxygen saturation; RDI, respiratory disturbance index.
Sleep-disordered breathing developed with increasing altitude in all subjects and the severity increased with a higher altitude, leaving all subjects with severe central sleep apnea and periodic breathing (Table 4). Recordings at 5,570 m were obtained only in one subject who had a 4% ODI of 144.9/h, a mean SpO2 of 68.5%, and a nadir SpO2 of 50.4%.
Respiratory parameters and EMG activity during sleep. Data are presented as mean (SD; 95%CI). (EMGdi = NRD, primary outcome), expressed as percent of maximum activity at sea level, for inspiratory and expiratory muscles at sea level and different altitudes (Night 1); only one sleep study was obtained at 5,570 m.
EMG, electromyography; EMGdi, electromyogram of the diaphragm; ODI, oxygen desaturation index; SpO2, oxygen saturation.
The EMG recordings at different altitudes showed increased variability that was associated with the development of sleep-disordered breathing. Cyclical crescendo-decrescendo patterns of inspiratory EMG activity were observed during most of the night (Fig. 1).
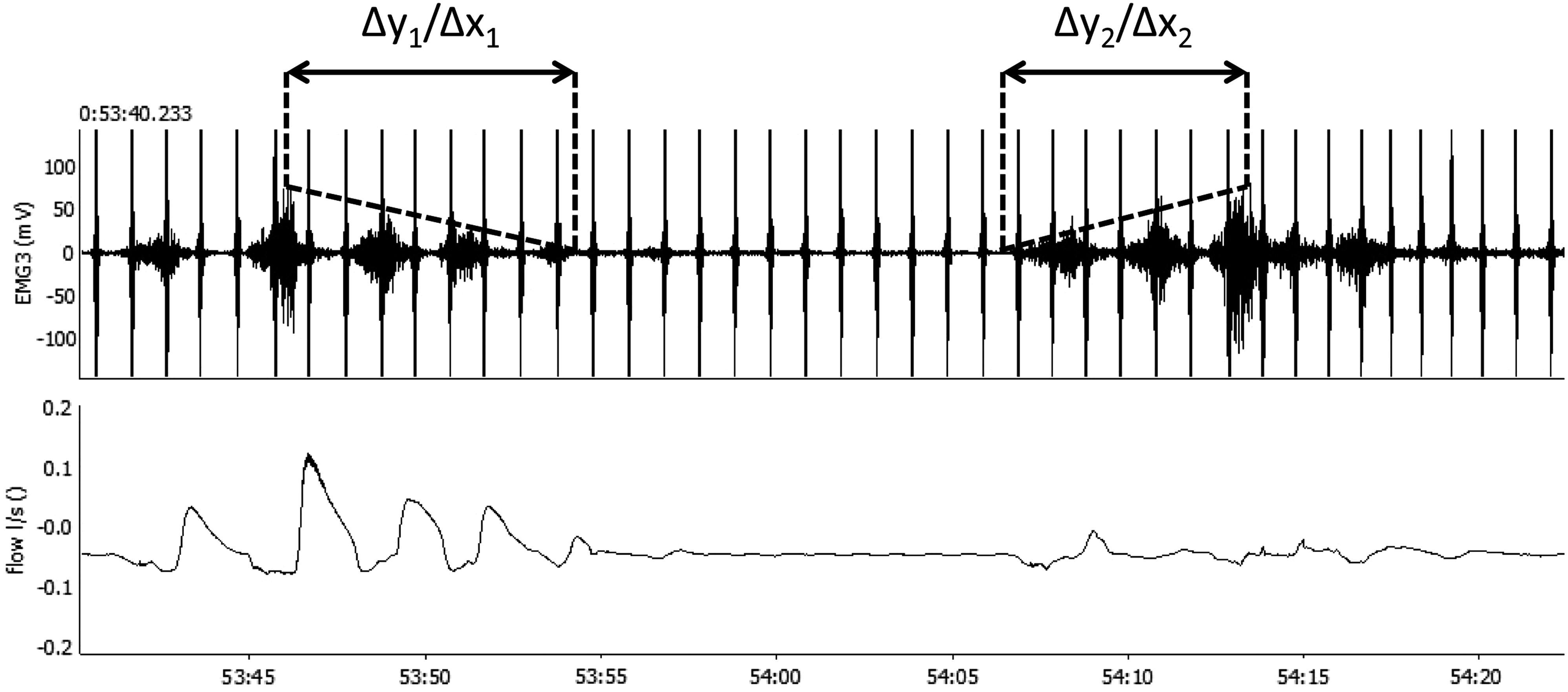
Periodic breathing while asleep in a healthy subject (BW) at 4,370 m altitude. The inspiratory activity of the diaphragm EMG (EMGdi, mV) is clearly visible between the ECG artefacts in Channel 1; airflow indicates a central apnea in Channel 2 (L/s). The decline in inspiratory EMGdi activity before the development of the apnea can be described by the gradient of the 1st slope (Δy1/Δx1); the incline in inspiratory EMGdi activity after the apnea is characterized by the gradient of the 2nd slope (Δy2/Δx2). ECG, electrocardiogram; EMG, electromyography; EMGdi, electromyogram of the diaphragm.
After sleep onset, EMG activity decreased significantly at sea level. At 3,380 m, increased EMG activity of the diaphragm, the parasternal intercostals, and the abdominal muscles was observed throughout the night. This activity did not increase significantly with further ascent to an altitude of 4,370 m (Table 4).
There was a positive correlation between the 4%ODI at 4,370 m and the EMGdi at 3,380 m (r = 0.97, p = 0.03) as well as a negative correlation between the EMGparasternal at sea level (r = −0.96, p = 0.04) and at 4,370 m (r = −0.97, p = 0.03). There was also an inverse relationship between the EMGdi at 3,380 m and the EMGparasternal at 4,370 m (r = −0.99, p < 0.01).
The cyclical occurrence of highly variable inspiratory activity when breathing asleep at altitude made it difficult to analyze stable periods of EMG activity and calculate averages (Fig. 2).
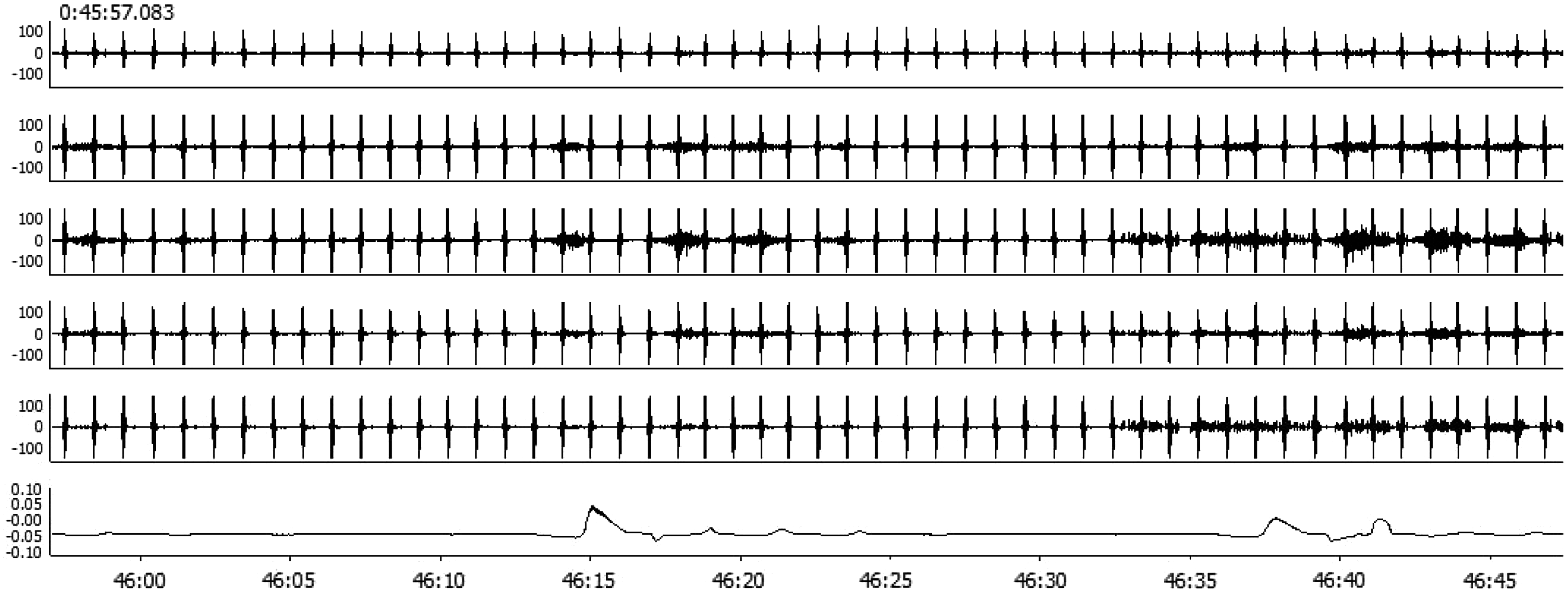
Transesophageal electromyography of the diaphragm (Channel 1–5; EMGdi) and airflow during sleep at 4,370 m of altitude. The EMGdi channel displays ECG artefacts (QRS complex) as well as inspiratory EMG activity. Airflow is indicated by pressure changes (Channel 6). There is a clear crescendo-decrescendo pattern in the inspiratory EMGdi activity followed by the absence of any inspiratory activity during central apnea.
Discussion
NRD, as measured by the diaphragm EMG, increases with high altitude as a response to hypobaric environmental conditions. The increased levels of drive are directly associated with the development of sleep-disordered breathing. The apnea threshold during periodic breathing is reached when EMGdi activity falls to levels below 5% maximum, the level required for resting breathing at sea level, and breathing resumes again when ∼10% of maximum EMGdi activity is reached after central apnea. To support diaphragm activity, extra-diaphragmatic muscles are recruited when asleep at altitude to achieve sufficient ventilation.
Clinical significance
In response to hypobaric conditions, a high NRD at altitude increases ventilation to maintain oxygenation; this leads to intermittent hypocapnia with a respiratory alkalosis, resulting in a Cheyne-Stokes respiration, particularly when asleep. The central apnea threshold while asleep is reached when NRD declines to a level lower than that required for resting breathing at sea level.
It has been established that human beings develop sleep-disordered breathing at altitude, but the accurate measurement of physiological parameters has been challenging. This is the first study at high altitude that has recorded the transesophageal crural diaphragm EMG from the electrical active region that allows the accurate measurement of central motor neuron output (NRD) in humans (Luo et al., 2009; Jolley and Moxham, 2016). Knowledge about how subjects recruit respiratory muscle activity during sleep helps to understand the factors that determine acclimatization to high altitude. The levels of EMGdi activity at altitude, expressed as percent of maximum, are similar to those in patients with moderate COPD, asthma, obesity hypoventilation syndrome, and obstructive sleep apnea (Luo et al., 2008; Jolley et al., 2009; Steier et al., 2009, 2010, 2011). Thus, respiratory reserve is reduced with increasing altitude and, despite increased muscle recruitment, both hypoxemia when awake and sleep-disordered breathing deteriorate with ascent to altitude. Interestingly, a level of NRD similar to that at sea level predicts the imminent onset of central apnea, the so-called apnea threshold (Xie et al., 2001; Steier et al., 2010). During this 5 week-long expedition, the limited acclimatization at each level of altitude did not significantly affect the apnea threshold.
A high NRD at altitude leads to a higher minute ventilation, which results in more significant hypocapnia; this triggers apneas and oxygen desaturations, as indicated by the positive correlation between the EMG of the diaphragm and the oxygen desaturation index. However, in subjects who adopted a different breathing pattern at altitude by recruiting more chest wall muscle activity, the sleep-disordered breathing seemed to be less severe, as indicated by a negative correlation between the parasternal EMG and the ODI. In addition, central efferent output can be divided between different muscle groups at the same time. In the studied cohort at altitude, we recorded from the diaphragm and the parasternal EMG to identify inspiratory muscle activity. The negative correlation between parasternal and diaphragm EMG indicates that the subject's respiratory pattern varied and, as parasternal activity was recruited, diaphragm EMG was diminished. Considering that the volume effect of parasternal intercostal muscle activity will be significantly lower than the contribution from increased diaphragm activity, it is likely that subjects with increased chest wall muscle activity will have experienced less significant hypocapnic epsiodes, resulting in less severe sleep-disordered breathing.
These observations reflect the chemosensitivity to low levels of pCO2 after a period of relative hyperventilation that is employed to control for hypoxemia in hypobaric environmental conditions. During a central apneic event, the pCO2 level rises slowly back to normal levels that normalize the pH, and the pO2 then starts to fall again with a circulatory delay.
Limitations
This was an exploratory study in a small group of mountaineers, limited by the number of participants and the difficult logistics, allowing for hypothesis generation. However, data presentation using the 95% CI and the reliable occurrence and analysis of periodic breathing at altitude with repeated measurements at different levels of altitude allow a “proof of concept” to validate the observations. The study was further limited by a lack of access to polysomnography equipment at altitude but, as the baseline study at sea level confirmed the absence of any sleep-disordered breathing, the reporting of the oxygen desaturation index in parallel to the recording of electromyography provided valuable information to assess ventilation. The data recorded were from the first night at each level of altitude; therefore, they were only available for a single night in each subject at each level. Future studies should be designed to understand the effect of acclimatization by recording subsequent nights in the same subjects.
Conclusion
An increased NRD drive was associated with more severe sleep-disordered breathing. Future research should investigate in detail whether there is a protective level of NRD and a gender effect predicting the ventilatory response at altitude.
Footnotes
Acknowledgments
This work was supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy's and St Thomas' NHS Foundation Trust and King's College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health.
The authors gratefully acknowledge the support of the International Foundation High Altitude Research Station Jungfraujoch, CH during the planning of this expedition and for accommodating the team for equipment tests, the provision of the solar panel from the Everest-Xtreme Expedition, and the generous support by Aerolinas Argentinas in transporting the equipment.
Author Disclosure Statement
No competing financial interests exist.