
Abstract
Abstract
Robinson, Jeffrey C., Cheryl Abbott, Christina A. Meadows, Robert C. Roach, Benjamin Honigman, and Todd M. Bull. Long-term health outcomes in high-altitude pulmonary hypertension. High Alt Med Biol. 18:61–66, 2017.
Background:
High-altitude pulmonary hypertension (HAPH) is one of several known comorbidities that effect populations living at high altitude, but there have been no studies looking at long-term health consequences of HAPH. We aimed to determine whether HAPH during adolescence predisposes to significant pulmonary hypertension (PH) later in life, as well as identify how altitude exposure and HAPH correlate with functional class and medical comorbidities.
Methods:
We utilized a previously published cohort of 28 adolescents from Leadville, Colorado, that underwent right heart catheterization at 10,150 ft (3094 m) in 1962, with many demonstrating PH as defined by resting mean pulmonary arterial pressure ≥25 mmHg. We located participants of the original study and had living subjects complete demographic and health surveys to assess for the presence of PH and other medical comorbidities, along with current functional status.
Results:
Seventy-five percent of the individuals who participated in the original study were located. Those with HAPH in the past were more prone to have exertional limitation corresponding to WHO functional class >1. Fifty-five years following the original study, we found no significant differences in prevalence of medical comorbidities, including PH, among those with and without HAPH in their youth.
Conclusions:
Surveyed individuals did not report significant PH, but those with HAPH in their youth were more likely to report functional limitation. With a significant worldwide population living at moderate and high altitudes, further study of long-term health consequences is warranted.
Introduction
I
In the Rocky Mountains of Colorado, there are an estimated 900,000 people living above 6900 ft (2100 m). This population has been the focus of a number of studies over the last 5 decades, offering the feature of being evolutionarily young; it is unlikely that there has been appreciable genetic adaptation to the high-altitude environment. In 1962, a unique study was performed in the city of Leadville, Colorado, which sits at an altitude of 10,150 ft (3094 m). After epidemiologic studies demonstrating significant right axis deviation on electrocardiographs (ECG) among school-going individuals, 28 healthy and asymptomatic individuals who were 12 to 17 years of age underwent resting and exertional right heart catheterization. Sixteen of these children had two findings of pulmonary hypertension (PH) on examination (increased P2), chest radiograph (enlarged pulmonary vasculature or right atrium), or ECG (right axis deviation), while 14 had no objective evidence of PH. The results (summarized in Table 1) were striking in that 10 of the 28 subjects had a resting mPAP ≥25 mmHg, along with many showing significant increases with exercise (Vogel et al., 1962).
Long-term health outcomes of patients with HAPH are largely unknown. Autopsy studies performed in the Andes demonstrate significant pathologic right ventricular and pulmonary vascular remodeling in subjects with HAPH (Penaloza and Arias-Stella, 2007), while a small series of young children (less than 2 years old) residing at high altitude in the Rocky Mountains were thought to have what was termed “primary pulmonary hypertension” due to their exposure to altitude (Khoury and Hawes, 1963). Chronic habitation at high altitude has also been suggested to be associated with a decreased risk for ischemic heart disease, while data involving chronic obstructive pulmonary disease, stroke, and cancer are conflicted (Jaillard et al., 1995; Mohanna et al., 2006; Faeh et al., 2009; Sherpa et al., 2010; Ezzati et al., 2012; Laniado-Laborin et al., 2012; Youk et al., 2012). Thus, we sought to characterize through health surveys the long-term health outcomes, including clinically significant PH, in this unique cohort of individuals, a large portion of who had hemodynamically proven HAPH as teenagers.
Methods
Subjects
Permission to contact individuals and all aspects of the study design were approved by the Colorado Multiple Institutional Review Board (COMIRB protocol 13-3113). Participants were mailed informed consent, followed by a survey that comprised medical comorbidities, including pulmonary vascular disease, details of functional class, pertinent history such as oxygen use and smoking history, current medications, and history of living at altitude. In addition, publically available obituary records were utilized to determine deceased individuals and determine cause of death when available.
Data collection
Following written informed consent, we had surviving individuals complete a general health survey to determine functional limitations, medical comorbidities, current medications, family history, pertinent exposures, and years at altitude, including current altitude. For deceased individuals, we assessed for cause of death from information in obituaries and the Social Security Death Index. Deceased individuals were included in the analysis of comorbidities when cause of death could be determined. Baseline demographics and hemodynamics were garnered from the original article from 1962.
Statistics
Data were stratified by the existence of resting PH (defined in our study as mPAP ≥25 mmHg), and by birth in Leadville vs. lower altitude. Binary data underwent analysis using Fisher's exact test with a two-tailed p-value analysis with p < 0.05 used as significance cutoff. Continuous variables were analyzed using student's t-test with p < 0.05 used as significance cutoff. All statistics and graphs were produced using Prism 6 (GraphPad).
Results
Survey response rate
After original participants were identified, we were able to establish contact and obtain completed surveys from 16 of the original 28 participants (Table 1). All located individuals agreed and consented to participation. Furthermore, utilizing archived obituaries and the Social Security Death Index, we were able to identify that five of the individuals were deceased, with two dying from traumatic accidents in young adulthood, one from malignancy, one from cardiovascular disease, and one unable to determine etiology. Hence, we obtained 75% capture of the original study participants.
Time spent at high altitude and altitude of current residence
We surveyed respondents on years spent residing in Leadville, Colorado, and (for those who had relocated) altitudes of other locations where they have resided. We found that mean time of residence >10,000 ft was 31.75 years (SD ±12.7 years), with individuals relocating to lower altitude at between 17 and 47 years of age, and current altitude of residence 4128 ft (SD ±3522 ft), with all but one individual relocating from Leadville, Colorado, to a lower altitude (Fig. 1).
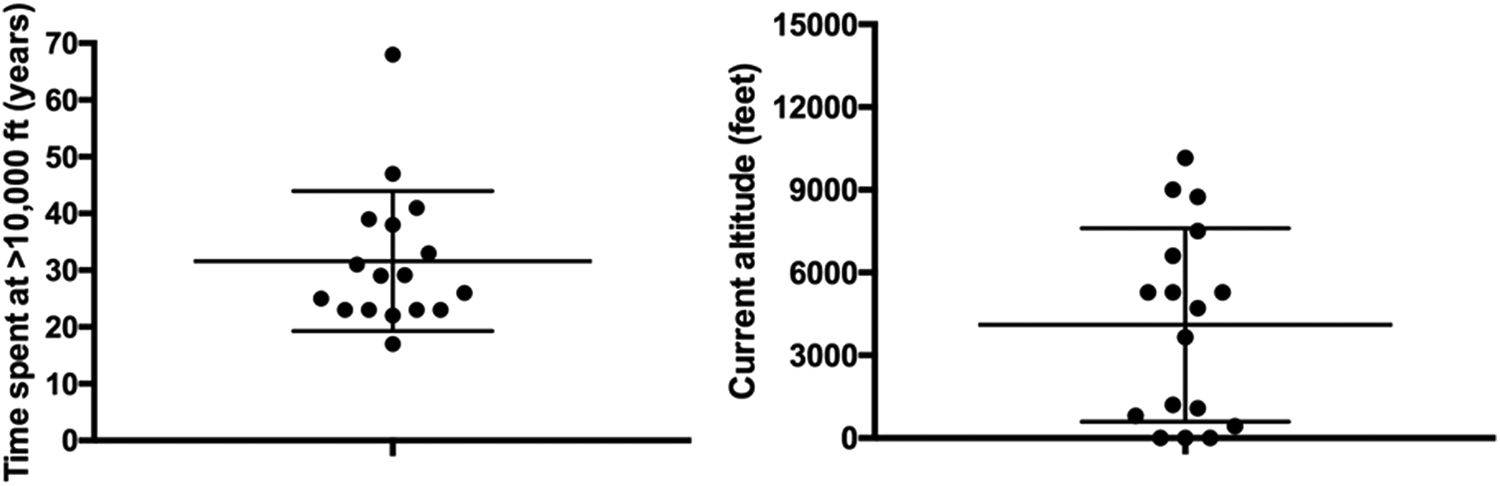
Time at altitude >10,000 ft and current altitude of residence of study respondents.
Chronic health comorbidities
We surveyed respondents on the existence of common medical comorbidities, examining both as a whole, and then stratified the results by the presence of resting HAPH in youth (Fig. 2), and assessed for development of chronic health conditions. Only one individual in the Leadville cohort self-identified as having PH, although this person was not on any specific pulmonary arterial vasodilator therapies and had carried this diagnosis since participation in the 1962 study. Furthermore, there was no significant difference in other pulmonary comorbidities, including asthma, chronic obstructive pulmonary disease (COPD), or sleep-disordered breathing between subjects with and without adolescent HAPH. Regarding cardiovascular disease, subjects collectively reported a 47.6% rate of systemic hypertension, with men in this cohort reporting a 23.1% rate of heart disease and no women reporting heart disease. 57.1% of individuals with HAPH as adolescents reported having diabetes, as opposed to 11.1% of those without. In summary, we found that the presence of adolescent PH was not clearly associated with risk for developing clinically evident progressive pulmonary vascular disease.
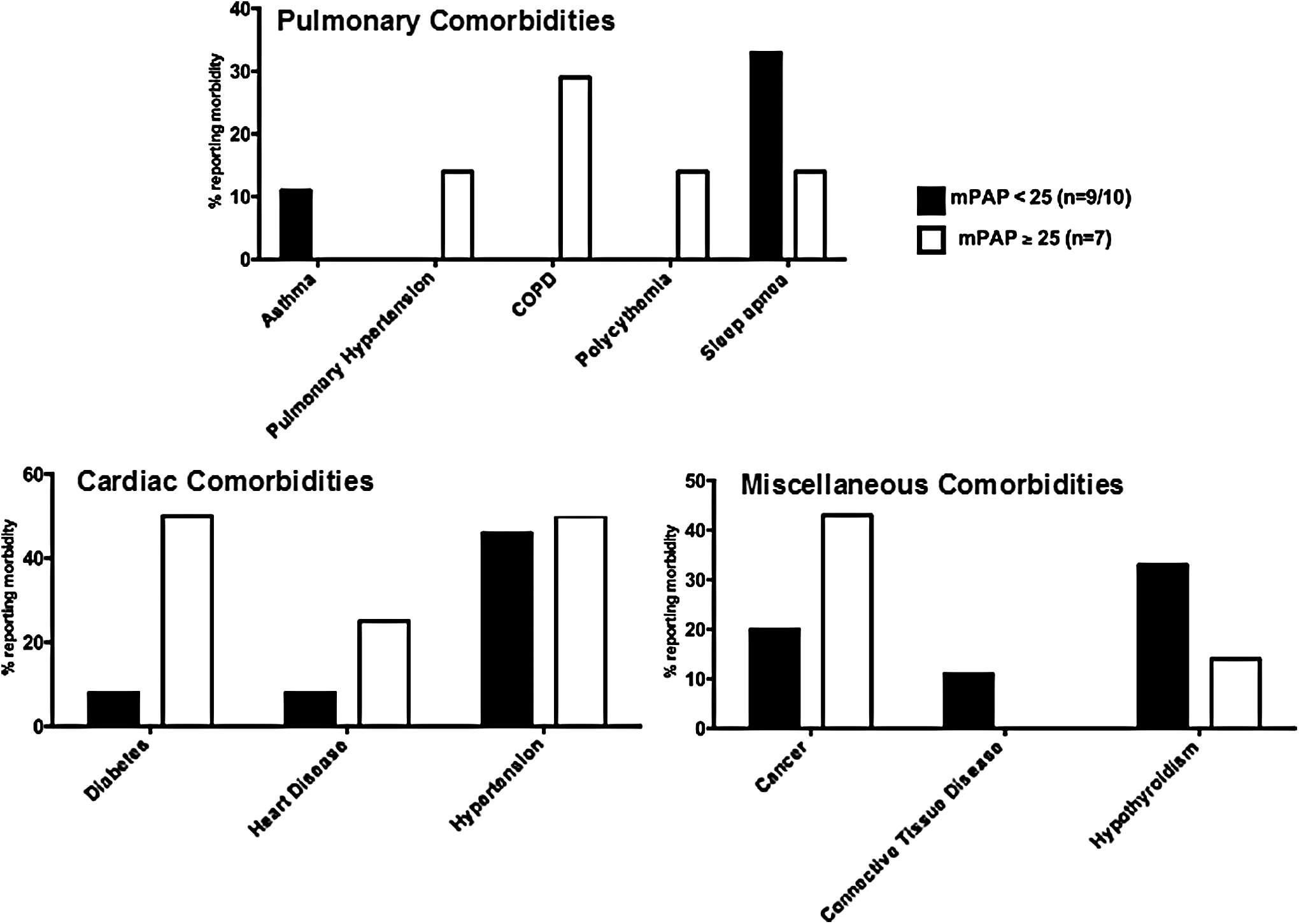
Self-reported medical comorbidities stratified by presence of adolescent HAPH. Individuals were stratified by adolescent mean pulmonary arterial pressure of < 25 or ≥ 25 mmHg and surveyed for pulmonary, cardiovascular, and other medical comorbidities. There were no significant differences in comorbidities as calculated using contingency table with Fisher's exact probability test.
Current functional class stratified by adolescent HAPH or altitude
We assessed for functional limitations in the Leadville cohort through a questionnaire that characterized activities of daily living by functional group: Group 1, no limitations in ordinary physical activity (ability to walk/climb stairs without fatigue or shortness of breath); Group 2, mild symptoms (comfortable at rest, but have slight fatigue, chest pain, shortness of breath, or lightheadedness with ordinary activity of walking, climbing stairs, and recreational activities); Group 3, significant limitation in activity due to symptoms (comfortable at rest, but have increased fatigue, chest pain, shortness of breath, or lightheadedness with ordinary daily activities requiring rest periods for showering, dressing, walking, climbing stairs, etc.); and Group 4, severe limitations in activity (symptoms of fatigue and shortness of breath with activity and at rest). It was found that all individuals with adolescent resting mPAP <25 mmHg reported no functional limitations, whereas three of the seven individuals with mPAP ≥25 mmHg reported significant functional limitation (Fig. 3A). When patients were stratified by total years spent at an altitude greater than either 5000 ft (1524 m) or 10000 ft (3048 m), as well as current altitude (Fig. 3B), there was no trend at worsening functional class.

Current functional class stratified by presence of adolescent HAPH or current altitude.
Association of neonatal high-altitude exposure and current functional class and comorbidities
High altitude has been associated with low birth weights, which has been documented in Leadville, Colorado, as well as the Andean populations, while the Tibetan population is relatively protected (Moore, 1990). Neonatal or childhood high-altitude exposure has been associated with diastolic dysfunction (Stembridge et al., 2016), and animal experimentation has suggested that neonatal hypoxia may predispose to pulmonary vascular dysfunction (Sartori et al., 1999; Julian et al., 2015), suggesting that neonatal or early childhood high-altitude exposure may alter susceptibility to various diseases through epigenetic or alternative means. Thus, we stratified our population by birth at Leadville, Colorado, or elsewhere and examined medical comorbidities and current functional class. Only 4 of the 16 survey respondents were not born in Leadville, Colorado, with the average age of moving to this altitude of 8.1 years (SD ±4.9 years). There were no differences in disease susceptibility or current functional class.
Discussion
Worldwide, there are >140 million individuals residing above 8200 ft (2500 m), estimates of HAPH prevalence range from 5% to 23%—with variation likely attributable to corresponding region of the world and underlying genetic background (Moore et al., 1998; West et al., 2012), emphasizing that HAPH is an important public health concern. Herein, we have utilized a highly unique cohort of patients from Leadville, Colorado, given their prior hemodynamic demonstration of a high prevalence of resting and exercise-induced PH to look at long-term health and functional outcomes. The demographics of survey respondents revealed that the great majority had moved to a lower altitude, although there was, on average, a significant amount of years spent at elevations >5000 ft.
We sought to determine the presence of PH within this population, finding only one individual who identified as having the disease, although the diagnosis dated back to the original study and the individual is not on a specific therapy for PH. In the original 1962 study, the rise in pulmonary vascular resistance with exercise appears to be predominantly due to hypoxic vasoconstriction, as evidenced by the administration of 44% oxygen to 22 students, which effectively reduced exercise mPAP by one third, regardless of the presence of resting PH. Furthermore, in a case report published after the 1962 study, one participant with a resting mPAP of 44 mmHg and exercise mPAP of 109 mmHg underwent repeat cardiac catheterization at sea level, in which her resting mPAP normalized to 17 mmHg, suggesting that perhaps—at young age—the HAPH seen in this population may be reversible (Grover et al., 1966). However, HAPH has been observed to have components characteristic of pulmonary arterial hypertension, including vascular remodeling (Arias-Stella and Saldana, 1962), in addition to a large body of work that demonstrates an integral role for hypoxic signaling in pathogenic vascular remodeling (Stenmark, 2006). It is somewhat reassuring that in this cohort, despite the prevalence of HAPH during their adolescence, there is no clear progression and development of clinically significant PH, which may be attributable to the fact that the majority moved to a lower altitude. However, three of seven subjects with mPAP ≥25 mmHg as adolescents had an increased propensity for functional limitation in later life, with none of the individuals with adolescent HAPH reporting limitations, raising the question of lasting physical effects of HAPH, perhaps in the form of vascular remodeling such as that seen in high-altitude inhabitants of the Andes. Importantly, the existence of adolescent HAPH was not associated with significant differences in medical comorbidities.
Prior studies have shown an association between high altitude and reduced rates of cardiovascular events (Ezzati et al., 2012), which have been posited to be related to increased catabolic state and reduced rates of obesity (Anderson and Honigman, 2011), or even a protective effect of hypoxia through increased hypoxia inducible factor stabilization in the myocardium (Eckle et al., 2008). Collectively, our subjects reported a 47.6% rate of systemic hypertension, as opposed to 65% of individuals over 60 years of age in the United States (Nwankwo et al., 2013). Furthermore, our study cohort reported a 17.6% rate of heart disease, compared to a reported U.S. prevalence of 25.5% in people aged 65–74 years (Johnson et al., 2014). While impossible to draw definitive conclusions from our small cohort, this would suggest a possible protective effect of long-term high-altitude exposure relative to the general U.S. population on cardiovascular risk.
There are multiple limitations within this study. There is the potential for considerable bias in survey sampling given the small sample size and risk of nonresponse bias and voluntary response bias. Furthermore, we acknowledge that comparing seven subjects with previous asymptomatic HAPH to nine subjects without HAPH (Table 1) is limited owing to lack of unbiased sampling in a study of this nature. Also, cause of death was determined utilizing publically available obituaries, which may be imprecise in true etiology of death. Our interpretation is also limited by the fact that except for one individual, all surveyed participants have relocated to a lower altitude. In this study, making firm associations between childhood HAPH and past and current altitude exposures with medical comorbidities is fraught with confounders, including environmental differences. Furthermore, making firm conclusions about long-term implications of HAPH of adolescents is limited in this population because the majority moved to lower elevations after several decades of altitude exposure.
In summary, our data suggest no clear long-term health risks associated with HAPH in the adolescent born at or living at high elevations for an extended period of time. Furthermore, as opposed to WHO Group 1 pulmonary arterial hypertension, HAPH has a distinct and nonprogressive pathobiology. A natural extension to the study herein would be to perform echocardiograms to assess for residual evidence of elevated right heart pressures or dysfunction—this was beyond the scope of this project. Also, there remain many unanswered questions regarding neonatal and childhood exposure leading to altered chronic disease susceptibility through genetic or epigenetic imprinting, which may play important roles in the development of high altitude pulmonary edema (Mishra et al., 2015), PH (Julian et al., 2015), or perhaps other chronic medical conditions (Brown and Rupert, 2014). In addition, how long must an individual be exposed to these conditions before long-term effects either positively or negatively are realized? Given the number of individuals—both in the United States and worldwide—who live at high altitude, there remain numerous unanswered questions of great public health interest. Larger scale epidemiologic studies will be necessary to more completely investigate the link between living at high altitude and comorbidities such as cardiac disease, metabolic disease, and pulmonary disease such as COPD.
Footnotes
Acknowledgments
J.C.R. had full access to all the study data and assumes responsibility for the integrity of the data and the accuracy of the analysis; he also drafted the initial article. J.C.R., T.M.B., C.A., and C.A.M. contributed to data collection and management. J.C.R., T.M.B., R.C.R., B.H., C.A., and C.A.M. contributed to analysis of the data and revision of the article.
Author Disclosure Statement
No competing financial interests exist.