
Abstract
Abstract
Ebert-Santos, Christine. High-altitude pulmonary edema in mountain community residents. High Alt Med Biol. 18:278–284, 2017.—High-altitude pulmonary edema (HAPE) affects lowlanders ascending quickly to elevations above 2440 m. Mountain resident children with no travel can sometimes develop HAPE as was observed over 30 years ago (Fasules et al., 1985). This is not well known and children instead are diagnosed as having pneumonia or asthma. In our clinic at 2800 m, we see children presenting with severe hypoxemia, clinical, and radiographic findings consistent with HAPE despite no recent travel. We call this mountain resident HAPE. We reviewed records of 48 patients with pulmonary symptoms. Analysis included vital signs, pulse oximetry, laboratories, physical findings, and clinical course. We identified 33 residents with HAPE and no travel, five with reentry HAPE, two visitors with classic HAPE, six residents with pneumonia, and two with asthma. Also, 48 X-rays on hypoxemic children seen between 2006 and 2017 were reviewed. Five showed definite HAPE with follow-up X-rays within 48 hours confirming rapid clearing on oxygen, 27 showed findings consistent with HAPE or viral pneumonia and no repeat study. Children living at elevation presenting with hypoxemia are commonly misdiagnosed. Rapid improvement with oxygen and little to no improvement with bronchodilators are more consistent with HAPE, and thus, antibiotics and other treatments can be avoided.
Introduction
H
There has been remarkable population growth in high-altitude cities and towns in the United States during the last 50 years. In Colorado, in the three counties above 2800 m, the population increased from 21,000 in 1980 to 52,000 in 2010. With migration and tourism, many more people are ascending above 2500 m, making HAPE more common in high-altitude medical clinics. With proper diagnosis, HAPE is easily managed while the consequences of undiagnosed and mistreated HAPE can be fatal.
It is well accepted that HAPE occurs in visitors at high altitude who present to local clinics with hypoxemia. With more mountain locals being treated for hypoxemia, there is an increasing clinical suspicion that HAPE may affect residents of high-altitude communities as well, a condition termed mountain resident HAPE (MRHAPE). This could also apply to those living at high-altitude plateaus such as in Tibet. The precipitating factor in the development of classic HAPE is the marked and relatively abrupt change in barometric pressure, with subsequent decrease in partial pressure of oxygen that causes severe pulmonary hypertension leading to pulmonary edema and worsened hypoxemia. The altitude at which this may happen can be less than 2400 m if the patient has or recently has had an upper respiratory viral infection (Gabry et al., 2003). Residents who are acclimated to high altitude do not develop HAPE secondary to a change in barometric pressure, but rather secondary to an upper respiratory infection. Inflammation from the infection may increase alveolar capillary permeability, such that even with their otherwise moderate pulmonary hypertension at altitude, alveolar capillary leak occurs resulting in the development of pulmonary edema and hypoxemia. A study of hypoxemia in Peru on children living at 3750 m examined 423 children with respiratory symptoms and compared them to 153 healthy children. Children with low oxygen levels were more likely to have pneumonia. However, 10% of children who had upper respiratory infections also had low oxygen levels, indicating the possible presence of MRHAPE (Reuland et al., 1991).
Recently, several physicians in mountain clinics and at St. Anthony Centura Summit Medical Center and St. Vincent's Hospital, all above 2800 m in Colorado, have theorized that some of the children who present with upper respiratory symptoms and hypoxemia are being misdiagnosed as having pneumonia or asthma when their disease course better resembles HAPE. These patients are full-time residents at altitude, with a negative travel history, and respond well to oxygen treatment, supporting the diagnosis of MRHAPE.
Case Reports with X-Rays
By definition, MRHAPE presents in patients with underlying respiratory illnesses. The degree of hypoxemia is remarkable when compared to other patients with colds, influenza, pneumonia, asthma, and/or sore throat. The following cases demonstrate the extent and range of symptoms and signs one can encounter.
Patient A
A 10-year-old male presented with increasing shortness of breath 24 hours after a clinic visit for fever. At the initial visit, he had normal oxygen saturation and a positive test for influenza during the H1N1 season. He was prescribed oseltamivir (Tamiflu®) and ibuprofen. His medical history was significant for multiple respiratory illnesses with hypoxemia. He had bronchiolitis at age two, upper respiratory infection (URI) with an O2 saturation of 86% that improved with nebulized albuterol at age five, and pneumonia with an O2 saturation of 87% at age seven. This illness manifested with a respiratory rate of 40 and rales in the right lung base.
Vital signs were as follows: HR 130, T 38.6, RR 24, O2 saturation 71%.
The patient was alert, but pale lying on the table. The only significant findings on physical examination were rales in the right lung and tachycardia. His O2 saturation improved to 90% on ½ lpm O2 given after albuterol nebulization. A chest X-ray demonstrated dense streaky infiltrates throughout the right lung (Fig. 1). White blood count was 7200. Blood cultures were negative.
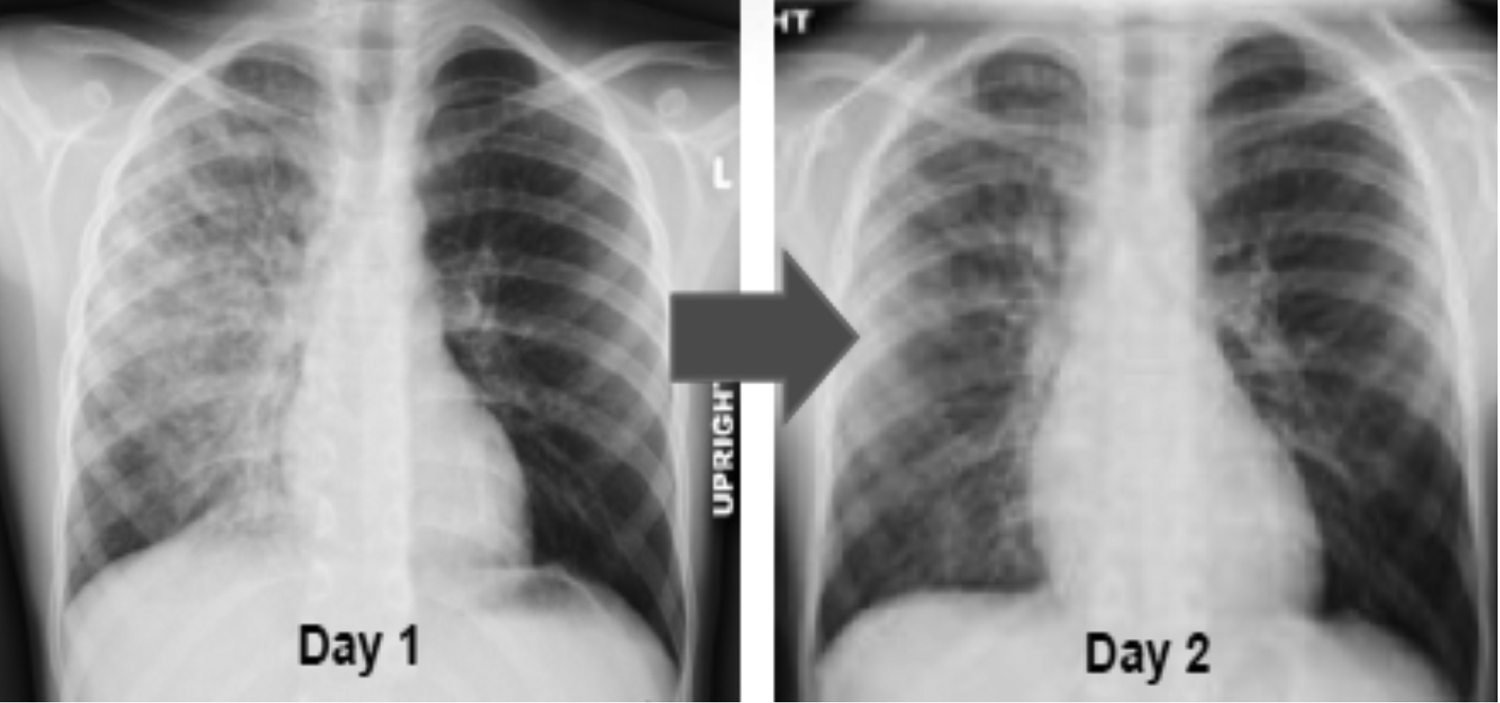
Ten-year-old male patient with suspected case of HAPE. X-ray below shows lung changes after treatment for 1 day. HAPE, high-altitude pulmonary edema.
The patient was admitted to the hospital and treated for presumed severe pneumonia with ceftriaxone, clindamycin, and vancomycin in combination with continued O2 therapy. He improved rapidly, and the pulmonary infiltrates as well as hypoxia resolved within 48 hours.
Patient B
A 15-year-old female presented with cough for 3 weeks, a fever of 101 degrees F., diarrhea, fatigue, and new onset of vomiting. She had recently been in Las Vegas and returned home 1 week before her appointment. Other family members also had upper respiratory symptoms. Five days before coming to our clinic she was seen by another physician in the community and documented to have an O2 saturation of 90%. The diagnosis at that time was hyperventilation.
Initial vital signs were as follows: RR 28, HR 113, BP 102/72, O2 saturation 81%.
Physical examination was unremarkable except for rales and rhonchi in both lungs. White blood count was 10,200. The chest X-ray was read as consistent with HAPE by the radiologist (Fig. 2).

Fifteen-year-old female presented with suspected case of reentry HAPE. X-ray below shows lung findings at the time of evaluation.
She was treated with O2 at 2 lpm. She returned in 3 days for follow-up. Her O2 saturation was up to 85% and her respirations down to 24. Her cough had improved and she was no longer vomiting. There were still some rales bilaterally. She returned again in 2 weeks with an O2 saturation of 87%–90%. On examination she had a wheeze and was treated with albuterol and prednisone. She returned 3 days later with a stable O2 saturation of 90% and clear lung fields bilaterally.
Materials and Methods
Two different reviews were conducted: a medical record review for signs and symptoms limited to a recent year and a review of chest X-rays taken over an 11-year period on patients with hypoxemia. Electronic medical records for the Ebert Family Clinic from the year 2015 were searched for the terms hypoxemia, HAPE, pneumonia, or asthma. This was a typical year for respiratory illnesses and data from other years were less accessible due to changes in electronic record systems in the clinic and hospital. From these patients, age, vital signs, oxygen saturation, respiratory symptoms, length of illness, course of illness, previous hypoxemic episodes, history of travel, and radiologic studies were considered. See Appendix 1 for treatment protocol.
Normal oxygen saturations at our clinic range between 90% and 94%. Patients suspected of having HAPE, because of significant hypoxemia (O2 saturation <89%), were further divided into classic HAPE, reentry HAPE, and MRHAPE. Patients determined to have classic HAPE were residents of low altitude communities visiting the mountains and presenting with significant hypoxemia. Reentry HAPE was diagnosed in patients with significant hypoxemia within 48 hours of returning to their high-altitude residence after spending time at a lower elevation. Classification of MRHAPE was based on the finding of marked hypoxemia in a high-altitude resident with no recent history of travel.
Forty-seven chest X-rays on 38 patients from 2006 to 2017 in children with hypoxemia treated by the author were reviewed by a radiologist with experience diagnosing altitude-related illnesses.
Results
Clinical case review 2015
The Ebert Family Clinic, located at 2800 m, draws patients from 1500 m above and below our clinic altitude. The clinic had 4230 patient visits in 2015 representing 1637 unique patients, 10% being tourists from lower elevations.
Seventy-one patients met the selection criteria. Infants with bronchiolitis were excluded because hypoxemia is common in this condition at any elevation. Children with a history of asthma but not symptomatic or hypoxemic were also excluded. This left a total of 48 patients, ages 20 months to 15 years, with the median age of 5 years. Thirty-three patients (69%) were determined to have MRHAPE, five patients (10%) with reentry HAPE, two patients (4%) with classic HAPE, six patients (13%) were determined to have had pneumonia, and two patients (4%) were determined to have an acute asthma exacerbation. Most of the patients with HAPE were of preschool and elementary school age. Among the patients with HAPE, there was a male predominance of 73%. Four children developed severe hypoxemia during the H1N1 influenza season in 2009, including a 13-year-old boy who died at home 5 days after a diagnosis of influenza. These data are presented in Table 1.
HAPE, high-altitude pulmonary edema.
Patients in all three HAPE groups appeared nontoxic and presented with cough and fatigue as their most prominent symptoms. All patients identified as having reentry HAPE or MRHAPE had oxygen saturations <89% on ambient air. Patients identified as having classic HAPE had oxygen saturations <75% on ambient air. Auscultation of the lungs was either normal or revealed rales at one or both lung bases. Those with normal lungs on initial evaluation would often have rales the following day. No consolidations were appreciated on physical examination. In most patients, treatment with an inhaled bronchodilator did not improve hypoxemia, ruling out significant asthma. These data are presented in Table 2.
C, cough; F, fever; R, rales; URI, upper respiratory infection; V, vomiting.
Of the 33 patients determined to have MRHAPE, fever was present at the time of evaluation in 21%, but some may have been medicated with antipyretics before evaluation. An increased respiratory rate (>20 breaths per minute) was documented in 24%. Most had tachycardia. Two of the children (both 5 years old) had heart rates under 100 bpm, and two 2-year olds had heart rates over 150 bpm. Associated symptoms commonly included cough, congestion, sore throat, and vomiting. Abnormal lung findings such as rales, crackles, rhonchi, or wheezing on physical examination were recorded in 64% of children. Ten children had some scattered wheezes. Because of their age, many were not able to cooperate and breathe deeply for the examination. These data are presented in Table 3.
Primary diagnoses are designated by F (fever), C (cough), ST (sore throat), URI (upper respiratory infection), W (wheezing), R (rales), V (vomiting), OM (otitis media), AP (abdominal pain), FLU (influenza), Rh (rhonchi), and Cr (crackles).
mo, months.
In younger children everywhere, bronchiolitis is common. They have wheezing and rhonchi on examination, and when they have severe hypoxemia they have retractions and tachypnea. In contrast, small children with MRHAPE do not have wheezing or retractions. Some children undoubtedly have both bronchiolitis and MRHAPE although we tried to exclude them from this review.
Radiologic case review
In the review of 48 chest X-rays on mountain resident children from 2006 to 2017, five patients had definite HAPE, with follow-up X-rays performed within 48 hours showing rapid clearing on oxygen. Findings consistent with mild HAPE or viral pneumonia were found on 27 films showing mainly increased perihilar markings. These patients did not have follow-up studies. Two patients had findings consistent with bacterial pneumonia and HAPE, three had pneumonia only, and four had peribronchial cuffing. Pneumonia was characterized by an area of focal consolidation. Four studies were read as normal and three patients were interpreted as having hypoinflation due to poor inspiratory effort or other nonspecific findings.
Discussion
High-altitude pulmonary edema, or HAPE, is a well-recognized syndrome in mountain communities throughout the world. The hypoxia at high altitude is thought to cause uneven regional vasoconstriction of the pulmonary blood vessels in those who are susceptible to HAPE (Bartsch and Swenson, 2013). The victim experiences a wet cough, dyspnea, confusion, fatigue, and eventually cyanosis. Death may occur within 48 hours when the progression of symptoms and severity goes unrecognized or undertreated. Oxygen is effective in treating HAPE because it will correct the hypoxemia by reversing vasoconstriction, thereby decreasing the edema and impaired gas exchange. Pulmonary hypertension decreases quite quickly with oxygen in HAPE (Gallagher and Hackett, 2014). Oxygen does not resolve either pneumonia or asthma.
Normal oxygen saturations at our clinic are 90%. A reading of 89% oxygen saturation is suspicious for a lung parenchymal process or hypoventilation. MRHAPE patients in 2015 had saturations in the 80% range. It is not unusual to have lower values, as demonstrated in Patient A, but with the availability of home pulse oximeters, hypoxemia is detected earlier and lower values are less common as patients present earlier in their illness. This is also true of reentry HAPE. Tourist children presenting at our clinic with classic HAPE have lower values; in this review, they were on average 72%–73%. More severe cases in all categories are seen in the emergency department due to the greater signs and symptoms of marked hypoxemia.
Patients with hypoxemia seen at the hospital have chest X-rays and bloodwork done. Those treated as inpatients usually have a second X-ray showing resolution. In our clinic, an X-ray is not routinely done and the diagnosis is made clinically unless parents request studies. In most cases, the children are seen in follow-up within 24 hours. The pediatrician can be accessed by phone at all times for any change in condition or parental concern.
Recurrent episodes of reentry and resident HAPE are common. Fifteen percent of children seen in 2015 with MRHAPE had prior episodes. Some children with MRHAPE also have had prior episodes of reentry HAPE. Since reentry HAPE is easier to prevent with oxygen on return to elevation or acetazolamide, most cases are not documented after the initial diagnosis is made and they are treated without physician involvement.
Although these hypoxemic children improve markedly within hours of starting oxygen, they sometimes require up to 10 days of supplemental oxygen before their oxygen saturations return to normal. This may be due to continued residence at high altitude and ongoing inflammation from the underlying illness.
All the children in this report were fully vaccinated, screened for cystic fibrosis at birth, and live in an environment with very little air pollution. If these 33 children had pneumonia, that would indicate an incidence 4.5 times higher than the 14.5/10,000 incidence of community-acquired pneumonia reported for children in the United Kingdom and Norway (Harris et al., 2011). Our estimate is based on census data showing 9087 children younger than the age of 18 in the three Colorado counties above 2800 m, about half of whom receive care at the Ebert Family Clinic. Research has shown that one of the predisposing factors for HAPE is a viral illness at the time or just preceding arrival to altitude (Durmowicz et al., 1997). One study infected rats with a common respiratory virus and exposed them to hypoxia 7 days later. Compared with control groups that were not exposed to viral infection and/or hypoxia, measurements of lung water, protein, and perivascular cuffing were increased in the infected hypoxic group (Carpenter et al., 1998).
Increasingly, doctors working in the mountains are recognizing that some residents who are well acclimatized may experience HAPE as a complication of a respiratory or other infection. Hypoxemia occurs several days after the onset of other respiratory illnesses. When patients present to medical facilities in the mountains with dyspnea, cough, and hypoxia, they are usually told they have pneumonia. Coding for hypoxia, pneumonia, asthma, and/or cough obscures possible MRHAPE cases. The symptoms and even X-ray findings overlap making it difficult to distinguish between HAPE and pneumonia during a single encounter. Rapid resolution of hypoxemia and pulmonary infiltrates is more consistent with HAPE than pneumonia or asthma.
Treatments and outcomes are different for an infectious process versus HAPE. Viral or bacterial pneumonia is treated with antibiotics and oxygen, while for HAPE, only high-dose oxygen and descent to lower altitude is needed (Hackett and Roach, 2001). A child with a viral pneumonia and an oxygen saturation of 84% would be very ill and require hospital care as opposed to children with MRHAPE who can do well at home. Those with pneumonia would not improve dramatically in 24 hours with decreased cough and increased activity. In addition, children seen at the Ebert Family Clinic with classic presentations of pneumonia, focal findings on physical examination, fever, and toxicity are often not hypoxemic.
Definitive physiologic evidence for the diagnosis of MRHAPE comes from a study done over 30 years ago. Nine children from Leadville (3010 m) with hypoxemia, rales, and typical radiographic changes of HAPE underwent cardiac catheterization in Denver after recovery from their illness. Pulmonary pressures were measured on ambient air and 16% oxygen. Pulmonary hypertension was documented during hypoxemic challenge that did not occur in the control group without a history of HAPE. All nine children were suspected to have developed HAPE associated with a viral illness and three had no recent travel history (Fasules et al., 1985).
Echocardiograms done during the hypoxic illness could indirectly measure pulmonary artery pressures and detect pulmonary hypertension and thus supporting the diagnosis of MRHAPE (Allemann et al., 2000). However, they are not available in our community on an urgent basis. Children who have more than one episode of HAPE are evaluated by a visiting pediatric cardiologist in our office quarterly to rule out underlying abnormalities. The risk for HAPE increases with conditions such as pulmonary hypertension, absent right pulmonary artery, certain heart defects such as patent foramen ovale that allow right to left shunting across the atrial or ventricular septa, and Down's syndrome (Bärtsch et al., 2007).
Incidence and significance of pneumonia and HAPE
Large numbers of people living at high elevation is a fairly new phenomenon in the United States. Ancient mountain societies, less susceptible to HAPE due to adaptation, thrive in Tibet, Nepal, China, Africa, and South America. For example, the city of Gondar, in Ethiopia, at 3000 m, has a population of over 100,000. Between migration and tourism, many more people are ascending above 2500 m without acclimatization that protects the natives who have lived in these locations for centuries. Medical personnel treating persons with respiratory symptoms in these areas need to know the various presentations of HAPE. Individuals and families traveling to or residing in the mountains should be aware of the dangers of HAPE. Many cases can be prevented and vacations salvaged by awareness and early detection.
Children and young adults in mountainous areas around the world could be experiencing HAPE complicating viral illnesses or pneumonia. Khan et al. (2009) report a higher incidence of “pneumonia” and recurrent pneumonia among children living at high altitude in Pakistan and other developing countries, similar to our experience in Colorado.
The connection between viral respiratory illness and HAPE may explain why MRHAPE is so much more common than pneumonia in mountain residents. Although we do see children with pneumonia in our clinic (6 in 2015), the population is basically healthy and progression from viral illnesses such as influenza to pneumonia is rare. Differentiating between pneumonia and HAPE is an important part of the clinical analysis at altitude because the course of the disease and risk of recurrence depend on the diagnoses. Patients with MRHAPE are encouraged to purchase a home pulse oximeter to monitor their oxygen saturation during any respiratory illness. Early treatment with oxygen may shorten the course and prevent visits to the emergency room and hospitalization.
Conclusion
Physicians working at altitudes over 2800 m have noted an increasing incidence of mountain residents presenting with acute hypoxemia. Many may have MRHAPE, which is often associated with an underlying concurrent URI viral illness and not with travel to or from low altitude. MRHAPE responds well to oxygen treatment alone and close follow-up care. Further study on the etiology and incidence of MRHAPE could lead to more accurate treatment and prevention along with the avoidance of unnecessary antibiotics and hospitalization.
Footnotes
Acknowledgments
This study was funded by the Ebert Family Clinic. Assistance in data collection and analysis and preparation of the article and tables was provided by Mariela Quijada, Noe Takada, MD, Kelly Kyte, Shail Patel, Atsuhiro Saisho, Claire Murray, Bryant Reinking, Matt Olney, DO, Anicia Santos, Mandy Allen, Meaghan Zeigler, Meg Ticknor, and other staff and students at the clinic. Encouragement and advice were appreciated from Erik R. Swenson, MD, Todd Carpenter, MD, Peter Hackett, MD, and Logan Spector, PhD.
Author Disclosure Statement
No competing financial interests exist.