
Abstract
Abstract
Pichler Hefti, Jacqueline, Philipp Hoigné-Perret, and Raimund Kottke. Extensive microhemorrhages of the cerebellar peduncles after high-altitude cerebral edema. High Alt Med Biol. 18:182–184, 2017.—Neuromagnetic resonance imaging (MRI) of subjects who suffered from high-altitude cerebral edema (HACE) typically shows cerebral microhemorrhages (MH) of the corpus callosum, in particular the splenium, and supratentorial white matter. This is a case report of a 43-year-old male, who suffered from unusually prolonged severe ataxia and amnesia after having been rescued during the ascent to Mount Everest at 6400 m. MRI of the brain 63 days after the incident showed the typical MH in the corpus callosum, but, in addition, extensive MH were found in the middle cerebellar peduncles. These infratentorial MH might reflect the pronounced atactic gait disorder. This case describes the first HACE-associated MH in the cerebellar peduncles in a high-altitude mountaineer indicating a potential vulnerability of infratentorial brain areas to hypobaric hypoxia.
Introduction
H
Case
The 43-year-old male mountaineer planned to climb Mount Everest from the north side in spring 2014. He is an experienced climber and the highest peak he successfully summited before was Mount Ama Dablam (6814 m) in 2012 with only little symptoms of AMS. His medical history is unremarkable and neither severe AMS nor HACE or HAPE were reported in the past.
Our patient and three other mountaineers, who did not know each other before, and their respective personal local climbing guides joined to an expedition group to share expenses for climbing permit and logistics. The ascent protocol to climb Mount Everest was in accordance with the usual practice: after the journey from Kathmandu (1400 m) to Everest Base Camp (5100 m) on the Tibetan side 7 days were spent at Base Camp for acclimatization, followed by acclimatization climbs to 5600 m, 5800 m, and four more days of acclimatization. Advanced Base Camp (6400 m) was reached on day 11. Soon after arrival at 6400 m, the mountaineer noted uncertainty in walking with impaired balance and moderate left occipital headache. He did not complain about dyspnea, severe headache, nausea, or emesis. However, clinical deterioration proceeded with somnolence, amnesia for an episode of 3 days, and sustained ataxia. Since there was not strong affiliation between the expedition members, the others proceeded with the climb. Due to the atypical presentation, which was not obviously associated with a life-threatening condition for nonmedics, he was not immediately evacuated. He was brought down by his local guide on a yak to Base Camp after these 3 days, where he was examined by a doctor, but communication was impossible due to language problems. He received no specific medical therapy, especially no dexamethasone which would have been indicated in HACE. Although oxygen was administered, somnolence and ataxia persisted over another 10 days before the symptoms resolved. He left Base Camp after these 10 days after weather conditions had improved and he had received the authority permit to travel to Nepal. He returned to Switzerland on his own, without medical assistance.
Back home, the mountaineer sought medical advice. Clinical inspection nearly 2 months after the incident revealed a well-trained general condition. Neurological examination showed no signs of cerebellar abnormalities with a normal finger-to-nose test, diadochokinesia, motility of the eyes, and regular gait. Neurocognitive and neurophysiological examinations were not performed.
Although the retrospective diagnosis of HACE was very likely, contrast-enhanced magnetic resonance imaging (MRI) of the brain at 3 Tesla was additionally performed to rule out other cerebral alterations. On the susceptibility weighted imaging sequence multiple small hypointensities, most likely representing MH were found in the corpus callosum, deep white matter of the centrum semiovale, and the middle cerebellar peduncles (MCP) in a symmetrical distribution (Figs. 1–3). The most pronounced affection was seen in the genu and splenium of the corpus callosum and in the MCP. The superior and inferior cerebellar peduncles were not affected. On T1-weighted, T2-weighted, and fluid-attenuated inversion recovery images, signal of the brain parenchyma was normal with the exception of a cystic parenchymal defect of the vermis and adjacent left cerebellar hemisphere. The lesion showed gliotic changes and peripheral susceptibility artifacts in keeping with small hemosiderin deposits (Fig. 3). There were no signs of subacute bleeding.
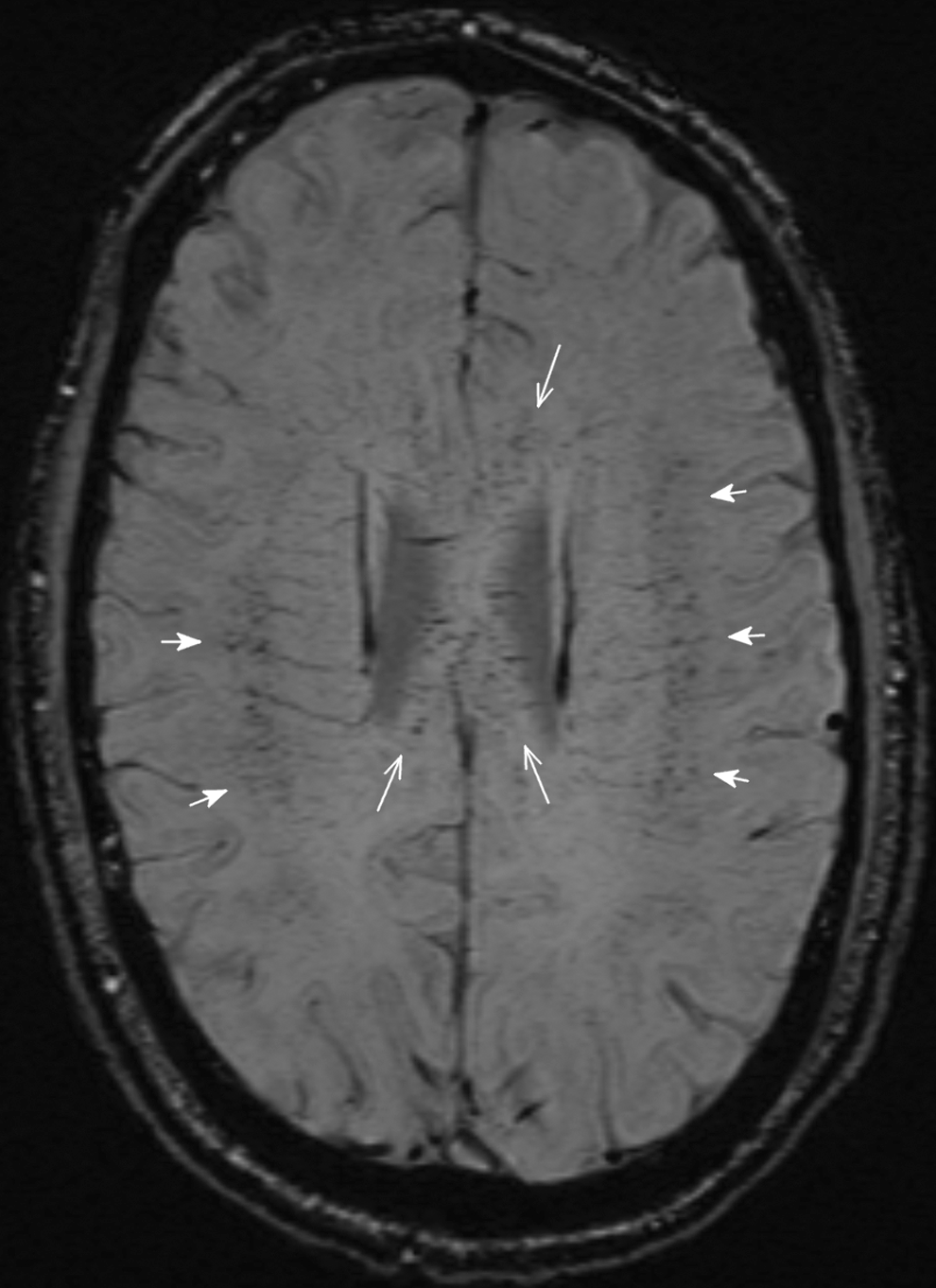
Symmetric distribution of MH in the deep white matter (short arrows) and the corpus of the corpus callosum (long arrows). MH, microhemorrhages.
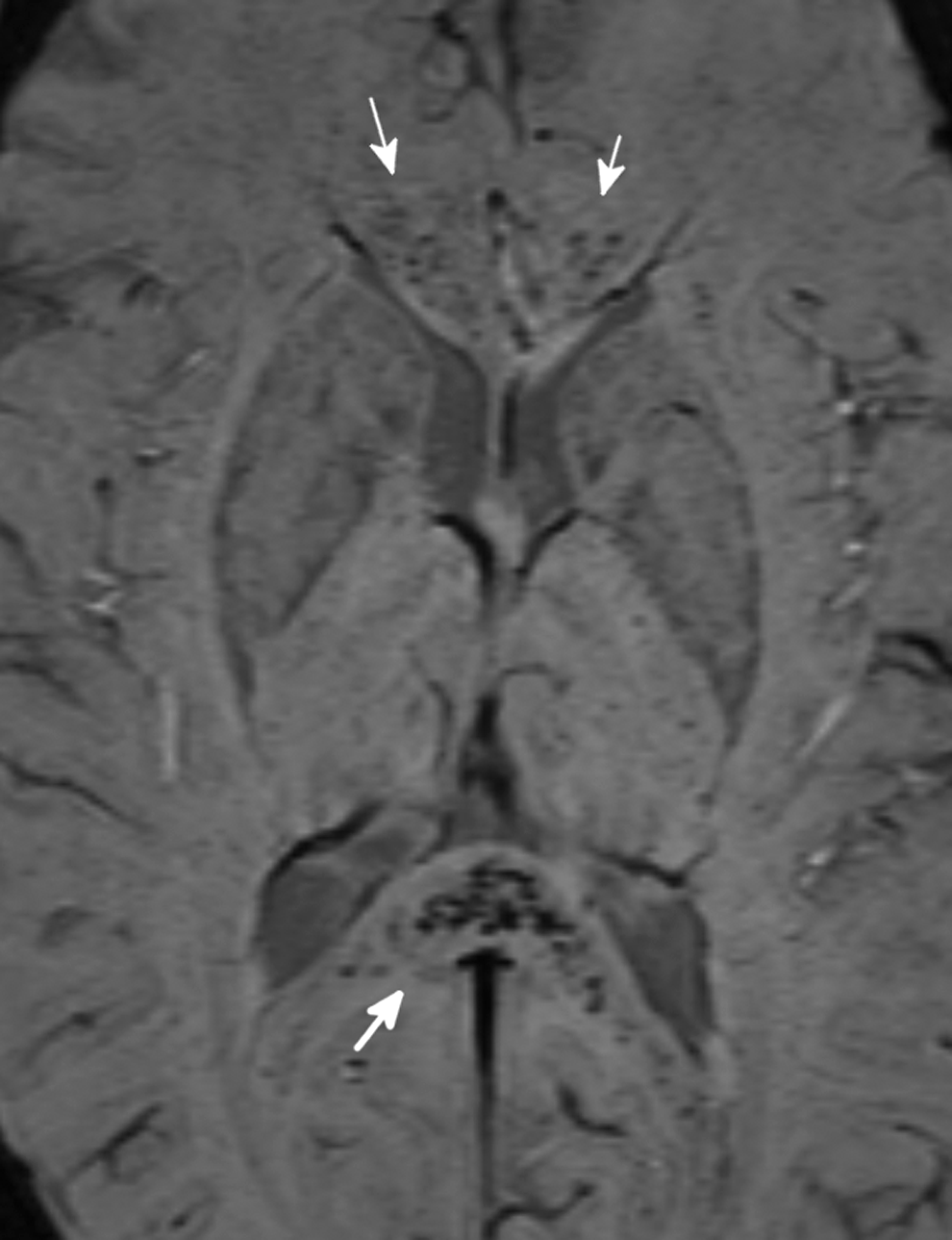
Multiple MH in the splenium (white arrow) and the genu of the corpus callosum (small arrows) typical for HACE. HACE, high-altitude cerebral edema.
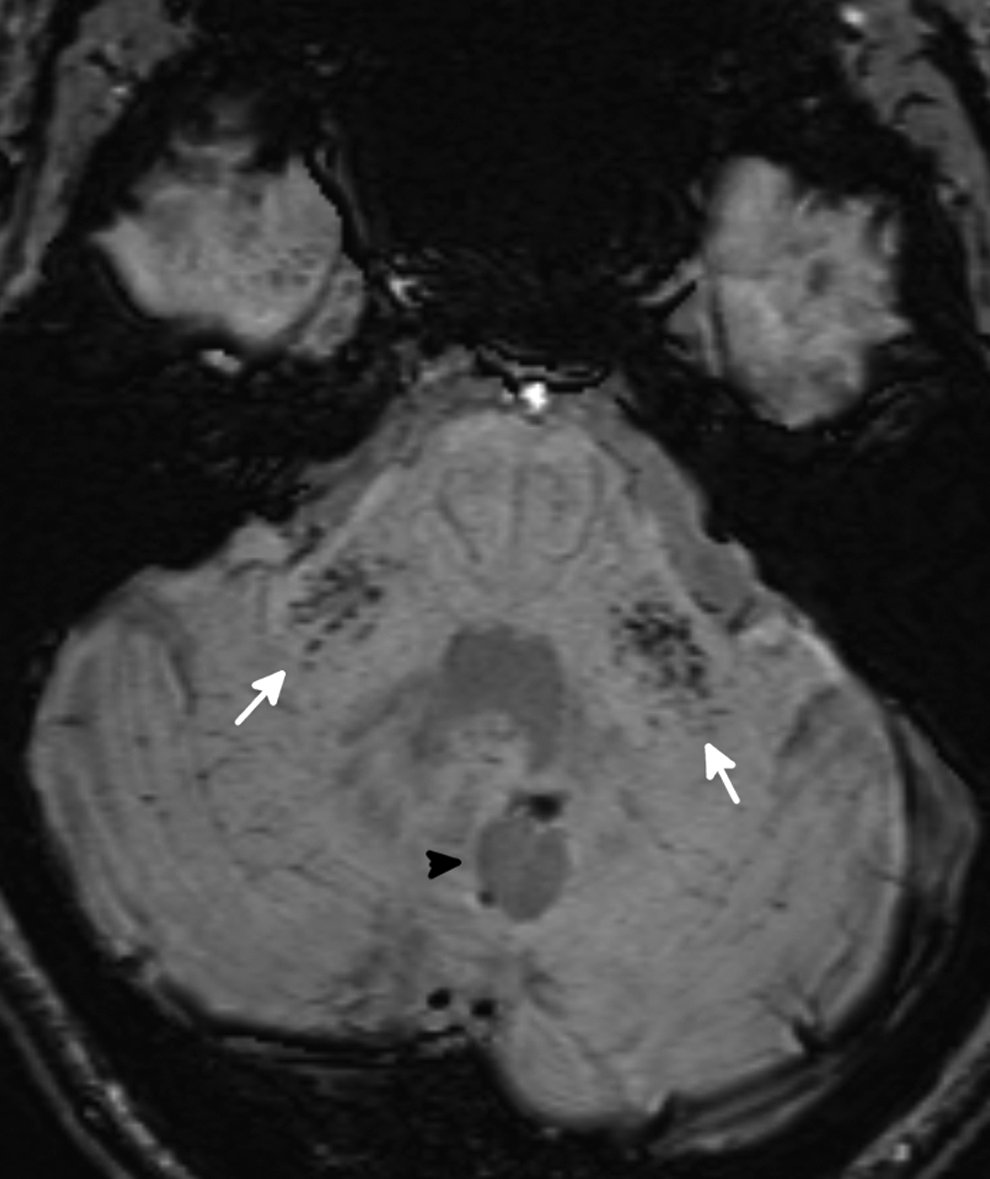
Multiple MH in both middle cerebellar peduncles (white arrows). Black arrowhead indicates old cystic hemorrhagic defect.
In a follow-up MRI after 1 year, the lesion, vermis, and cerebellar hemisphere presented completely unchanged and thus was considered an incidental finding, most likely corresponding to a residuum of an old, possibly even prenatal, hemorrhage or infarct and was not related to MH and HACE. The MH were unchanged in number and distribution on follow-up imaging, at best a slight haziness of some MH was observed. Both examinations were performed on a 3 Tesla MR unit (MAGNETOM Skyra; Siemens, Erlangen, Germany).
Discussion
The course of the events and symptoms are strongly suggestive for HACE, although information on the case history is limited due to the 3-day amnesia and statements of a third party are missing. In this case, it is rather unusual, that no mild-to-severe AMS was reported earlier and that gait ataxia was very pronounced and persisted for an uncommonly long time. And, although the severity of symptoms was alarming, it is exceptional that no fatal progression occurred with the delayed treatment that was restricted to oxygen supply, only.
In line with typical findings on neuroimaging in subjects who suffered from HACE, we found MH in the corpus callosum and cerebral white matter of the centrum semiovale (Figs. 1 and 2). But, in addition, multiple infratentorial MH were present in the MCP (Fig. 3) indicating major blood–brain barrier dysfunction in this area, a finding, which has not been described before in the context of HACE. The amount of MH in our case is comparable to the images published by Schommer and Kallenberg in patients who suffered from severe HACE (Schommer et al., 2013).
It has been shown that vasogenic edema is the major factor in the pathophysiology of HACE (Hackett, 1999). Vasogenic edema, indicating blood–brain barrier disruption, occurs with a predilection for the splenium of the corpus callosum and deep white matter and can lead to MH. In the study of Hackett (1999), no mention of symmetric vasogenic edema in the cerebellar peduncles has been made. The reason for these predilection sites is unknown, but it is assumed that vasogenic edema is more likely to occur in white matter due to its orderly structure. A possible common feature of the corpus callosum and the MCP may be that in both sites white matter fibers are highly structured. Vasogenic edema of the MCP is not very common but has been described in other pathologies affecting the blood–brain barrier as in posterior reversible encephalopathy (Morales and Tomsick, 2015).
The corpus callosum is supplied by short perforating arteries, whereas the MCP are mainly supplied by the anterior inferior cerebellar arteries, so the vascular supply of both structures does not readily explain the common findings in our case.
The patient's history did not reveal any previous episodes of severe AMS or HACE, although little AMS symptoms have been reported in the context of an earlier mountain expedition. Therefore, and as there is some evidence for cerebral MH in asymptomatic but severely hypoxemic mountaineers at high altitude (Kottke et al., 2015), it cannot be excluded that some of the MH may have been preexisting from a previous sojourn to high altitude. Ataxia is a common symptom in HACE, in this case severity and duration of gait ataxia were very pronounced. This somehow unusual presentation might be reflected by the exceptional peduncular MRI findings.
Conclusion
This case demonstrates that MH in the setting of HACE may also occur in an infratentorial location in the MCP, in addition to the classic affection of the corpus callosum and supratentorial white matter of the centrum semiovale. Furthermore, these findings suggest the MCP to be an additional predilection site of hypoxemic or HACE-induced blood–brain barrier disruption. Both, the corpus callosum and the MCP are highly ordered white matter structures, which may make them more susceptible to vasogenic edema and ultimately MH under certain conditions. We can only hypothesize that the prolonged stay at high altitude after symptom onset and the lack of adequate treatment are etiologic for the unusual pattern of MH in our case. The exact pathophysiology remains to be elucidated. Future MRI studies will show whether involvement of the MCP in HACE as in this case is rare or actually more common than currently thought.
Footnotes
Author Disclosure Statement
No competing financial interests exist.