
Abstract
Abstract
Bailey, Damian Miles, Benjamin S. Stacey, and Mark Gumbleton. A systematic review and meta-analysis reveals altered drug pharmacokinetics in humans during acute exposure to terrestrial high altitude—clinical justification for dose adjustment? High Alt Med Biol. 19:141–148, 2018.
Objective:
While physiological responses during acute ascent to terrestrial high altitude (HA) have the potential to alter the pharmacokinetics (PKs) that define absorption and disposition of medicinal drugs, there have been no systematic reviews and meta-analyses performed to date.
Methods:
We conducted a systematic literature search in June 2017 using NCBI PubMed, EMBASE, Web of Science, and Ovid MEDLINE databases to identify relevant observational studies. Studies were deemed eligible based on the following criteria: (1) participants: healthy, nonacclimatized male or female lowlanders (born and bred at sea level) and (2) environment: exposure to low altitude (LA, ≤600 m), followed by terrestrial high altitude (HA, ≤24 hours to ≥2500 m), the time course specifically selected to avoid interpretive complications associated with erythrocytosis. All PK parameters were standardized to be in the same units and the weighted standardized mean difference (SMD) calculated using a combination of fixed and random effects models with heterogeneity evaluated using χ2 and I2 statistics.
Results:
Of 20,840 studies reviewed, 6 prospective cohort studies (n = 75) qualified for inclusion, with participants exposed to a mean altitude of 4025 (mean) ± 380 (SD) m. We observed increases for absorption half-life (SMD: 0.40, 95% CI: 0.01–0.80, p = 0.04], elimination half-life (SMD: 0.89, 95% CI: 0.30–1.48, p = 0.003), and erythrocyte binding (SMD: 0.52, 95% CI: 0.16–0.88, p = 0.004) and reduction in clearance (SMD: −0.56, 95% CI: −1.13 to 0.00, p = 0.05).
Conclusions:
Collectively, these findings reveal impairments in both oral absorption and corresponding clearance of the, although limited, sample of drugs at HA that may potentially require closer patient monitoring and dose adjustments to maintain therapeutic efficacy and avoid incidental toxicity.
Introduction
T
These physiological adjustments have the capacity to alter the pharmacokinetics (PKs) that define absorption and disposition of drugs subsequent to alterations in, among others, cytochrome P (CYP)-450 activity, pH, protein binding, distribution volumes, and perfusion (Fig. 1A, B). This is clinically relevant given the millions of lowlanders who sojourn to HA for occupational, recreational, or religious purposes (Li et al., 2009) and increasing number of mountaineers who prophylax with a cocktail of drugs in an attempt to accelerate acclimatization and improve summit success (Donegani et al., 2016; Nieto Estrada et al., 2017).

Environmental stressors and physiological responses during acute (<24 hours) exposure to terrestrial high altitude
However, to what extent drug PKs change in response to the multiple stressors encountered at terrestrial HA (hypoxia, exercise, and cold, see Fig. 1) remains unclear, complicated, in part, by conflicting findings from a limited number of studies constrained by small sample sizes and limited ability to detect treatment effects with participants exposed to different drugs, altitudes, and exposure times. Thus, for the first time, a systematic review and meta-analysis was conducted to summarize the results of relevant studies in an attempt to increase sample size and corresponding statistical power. The primary aim was to determine the effects of acute exposure (≤24 hours) to terrestrial HA on drug PKs with a secondary aim of determining optimal sample sizes to help guide the design of future trials.
Methods
Database and search strategy
A systematic review of the published literature was conducted (Fig. 2) in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement as a guide (Knobloch et al., 2011). Specific care was taken to fulfill key requirements to ensure the validity of our meta-analysis, namely (1) well-defined objectives, including precise definitions of clinical variables and outcome, (2) an appropriate and well-documented study identification and selection strategy, (3) evaluation of bias in the identification and selection of studies, (4) description and evaluation of heterogeneity, (5) justification of data analytic techniques, and (6) use of sensitivity analysis (Walker et al., 2008). Two independent investigators searched NCBI PubMed, EMBASE, Web of Science, and Ovid MEDLINE databases before June 27th (2017) using the following key words and Boolean connectors: (pharmacokinetics OR pharmacodynamics OR drugs OR medicines) AND (altitude OR high-altitude).
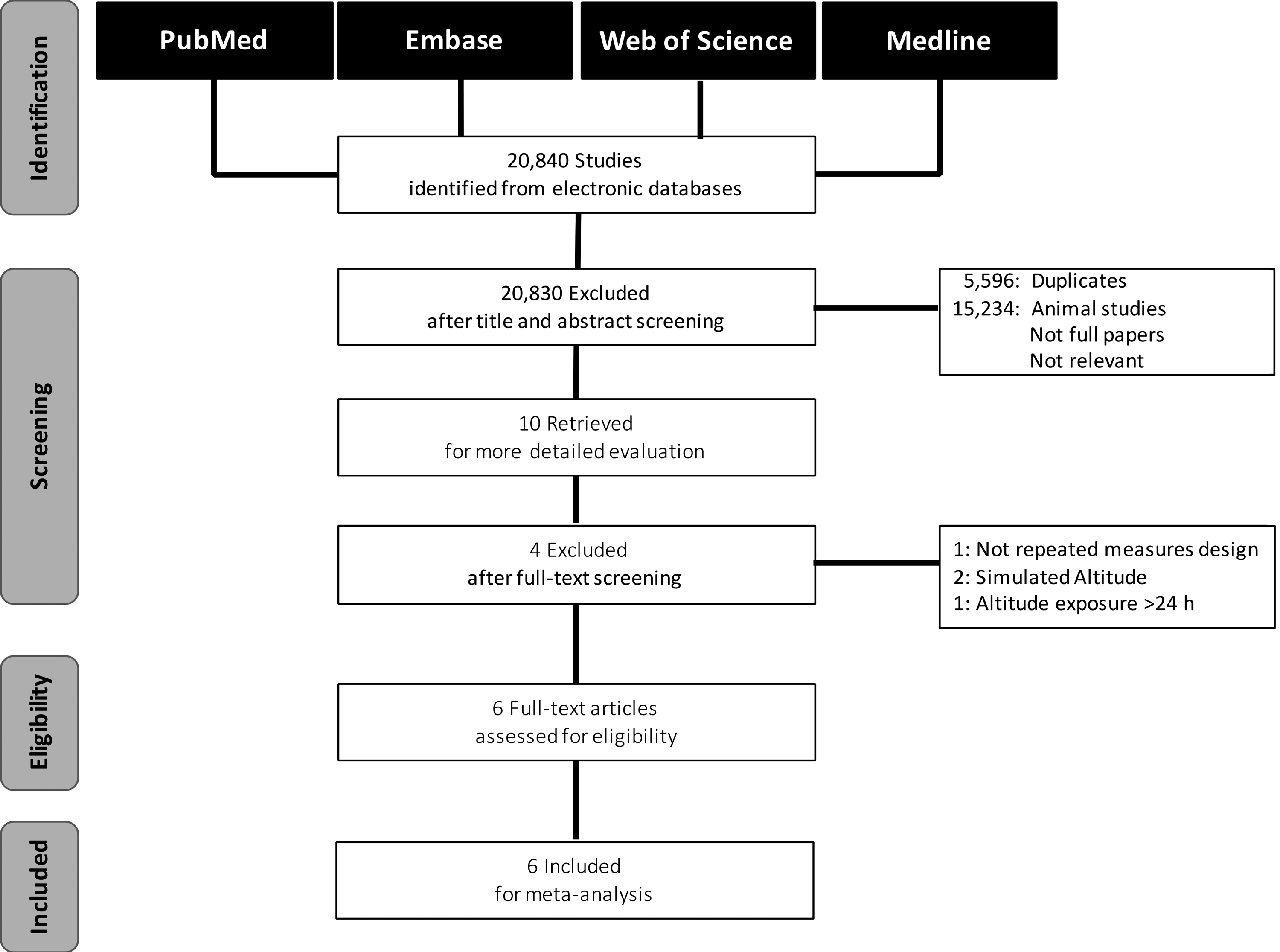
PRISMA flowchart.
Selection and quality assessment
Inclusion criteria
Studies were deemed eligible for meta-analysis based on the following criteria: (1) participants: healthy, nonacclimatized male or female lowlanders (born and bred at sea level) and (2) environment: exposure to low altitude (LA, ≤600 m), followed by terrestrial high altitude (HA, ≤24 hours to ≥2500 m).
Exclusion criteria
We excluded studies that were (1) performed on animals, (2) duplicates (originating from the same participants by the same investigators, but published in different journals), (3) letters to editors, reviews, commentaries, case reports, unpublished articles, and articles providing insufficient information relating to PK parameters, (4) simulated normobaric hypoxic (laboratory-based) studies given the acknowledged physiological differences compared with hypobaric hypoxia (Millet et al., 2012), and (5) those incorporating chronic (>24 hours) exposures to avoid interpretive (PK) complications associated with erythrocytosis.
Quality
Study quality could not be formerly assessed given that none of the studies were randomized, blinded, or provided sample size calculations. The final decision about inclusion or exclusion was achieved through mutual agreement.
Data extraction
The two investigators extracted data using structured data collection tables. All data entries were double-checked manually and all discrepancies resolved through discussion. The following information was extracted from selected studies: authors, publication year, experimental design, drug examined, sample size, altitude, and PK parameters. The PK parameters were standardized to be in the same units and included absorption rate constant (kA), volume of distribution as a function of bioavailability (Vd/F), mean residence time (MRT), absorption (t½A) and elimination (t½) half-lives, clearance as a function of bioavailability (CL/F), elimination rate constant (K), time to peak plasma concentration (TMAX), and erythrocyte binding (CE).
Statistical analyses
Statistical analyses were conducted using the Cochrane Review Manager software (RevMan, Version 5.3.5 for Windows, Cochrane Collaboration, Oxford, United Kingdom, www.cc-ims.net/RevMan) to pool data for each of the PK parameters and associated variables. Continuous outcomes were presented as a standardized mean difference (SMD, Hedges g) along with 95% confidence intervals (CI). Effect sizes of <0.2, <0.5, <0.8, and >0.8 were considered trivial, small, moderate, and large, respectively (Cohen, 1992). Heterogeneity was evaluated using the Cochran χ2-based Q and Higgins I2 statistics that assess the appropriateness of pooling individual study results (Higgins et al., 2003). Random effects models (DerSimonian and Laird, 1986) were applied if heterogeneity was evident (χ2 p < 0.10/I2 > 50%), otherwise fixed effects models (Mantel and Haenszel, 1959) were employed. Publication bias was assessed using a funnel plot in combination with Egger et al.'s test (Egger et al., 1997). Power and sample size calculations were performed using G*Power (version 3.1.9.2). Significance was established at p < 0.05 for all two-tailed tests and data presented as mean ± SD unless otherwise stated.
Results
Study identification and characteristics
Applying the search terms, a total of 20,840 publications were identified, of which ten were considered relevant after initial screening by title and abstract (Fig. 2). After applying the inclusion and exclusion criteria, six full-text articles employing separate drugs were selected for meta-analysis (Table 1). The general properties of the six drugs are summarized in Table 2. These articles constituted nonrandomized single-arm studies comprising a total of 75 healthy males of either Chinese or Chilean descent. Participants were 21 ± 3 years old and exposed to both LA (267 ± 301 m) and HA (4025 ± 380 m) for 14.2 ± 1.7 hours. There was no consistent evidence of systematic publication bias (p > 0.05).
Cited as day after arrival.
Age expressed as mean ± SD (or range).
IM, intramuscular; PO, oral; NR, not reported.
Sources: The DrugBank Database; Medscape; electronic Medicines Compendium (eMC); TOXNET US National Library of Medicine.
t½, elimination half-life; cLogP (using ALOGPS), logarithm of compound's partition coefficient; PSA (using CHEMAXON), polar surface area; Å, angstrom.
Outcomes
The drugs appeared to be well tolerated since there were no serious adverse events reported. Figure 3 provides a summary of the mean changes (SMD) observed in each of the PK parameters documented at HA based on the individual studies (Supplementary Fig. S1a–j; Supplementary Data are available online at www.liebertpub.com/ham). We observed significant increases for t½A (SMD: 0.40, p = 0.04) and t½ (SMD: 0.89, p = 0.003), while the hybrid parameter CL/F showed a corresponding reduction (SMD: −0.56, p = 0.05). These were considered of potential physiological significance given the SMD cutoff of ≥0.50 standardized units as illustrated (Fig. 3). In contrast, no changes (p > 0.05) were observed in the remaining parameters, notably kA, TMAX, Vd/F, or K (latter SMD: −0.53). Similarly, MRT, while not significant, showed a marked tendency to be increased (SMD: 0.56, p = 0.09). Finally and as expected, significant increases in Hct (SMD: 1.02, p = 0.01) and CE (SMD: 0.52, p = 0.004) were observed.
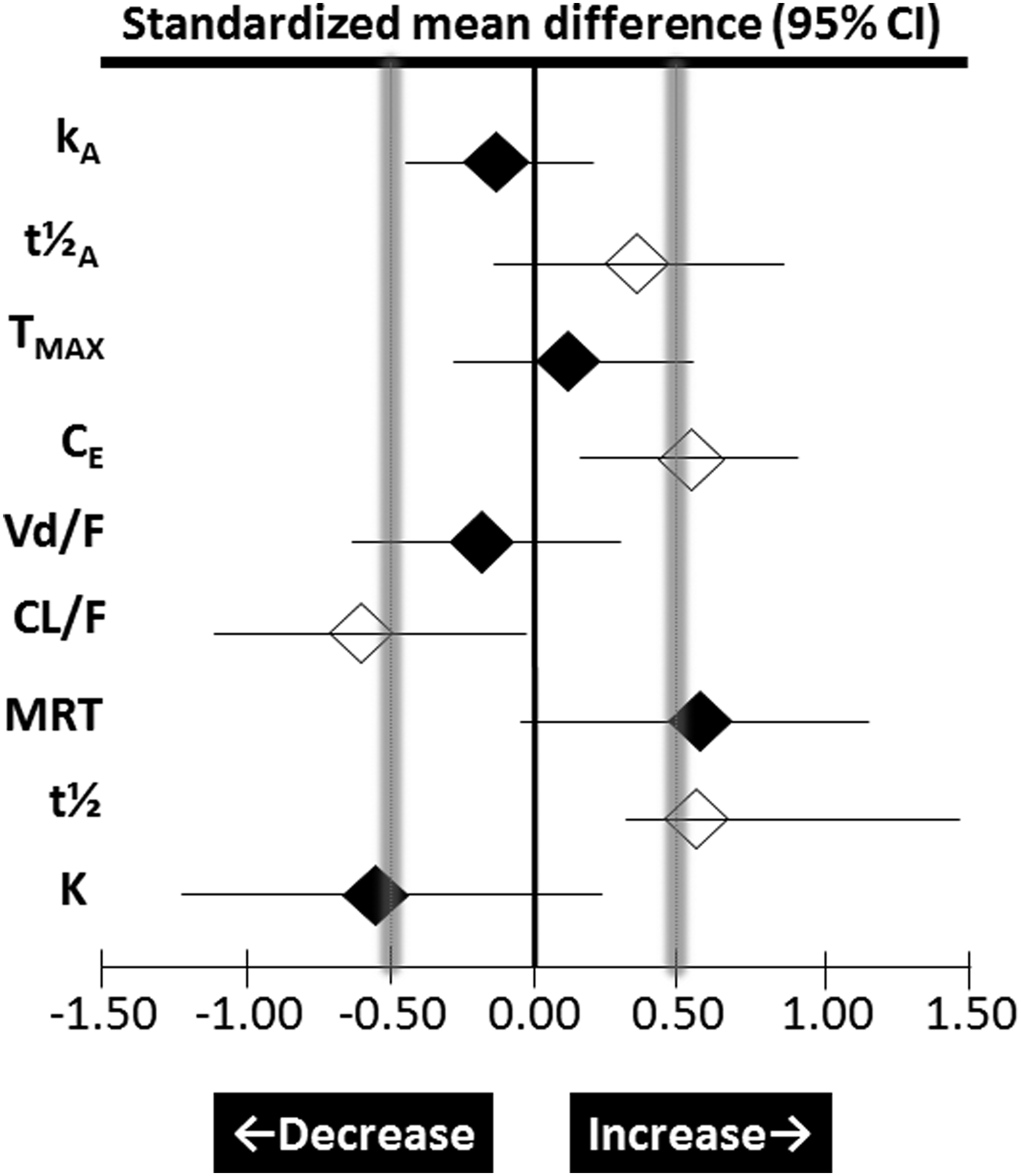
Forest plot of drug pharmacokinetics at high altitude. Forest plot data expressed as the standardized mean difference (SMD) with 95% confidence intervals; open diamonds represent significant changes (p < 0.05 vs. sea level), whereas closed diamonds are not significant (p > 0.05); stippled lines reflect boundaries beyond which changes are considered physiologically meaningful; kA, absorption rate constant; t½A, absorption half-life; TMAX, time to peak plasma concentration; CE, erythrocyte binding; Vd/F volume of distribution as a function of bioavailability; CL/F, clearance as a function of bioavailability; MRT, mean residence time; t½, elimination half-life; K, elimination rate constant.
Statistical power and sample size
Post hoc analyses revealed that studies were generally underpowered with no singular pharmacokinetic parameter achieving the (minimal) requisite power of 0.8 (Fig. 4). Prospective calculations indicated that sample sizes needed to be in the order of ∼2 to over 1500-fold larger to be adequately powered to detect a treatment effect.
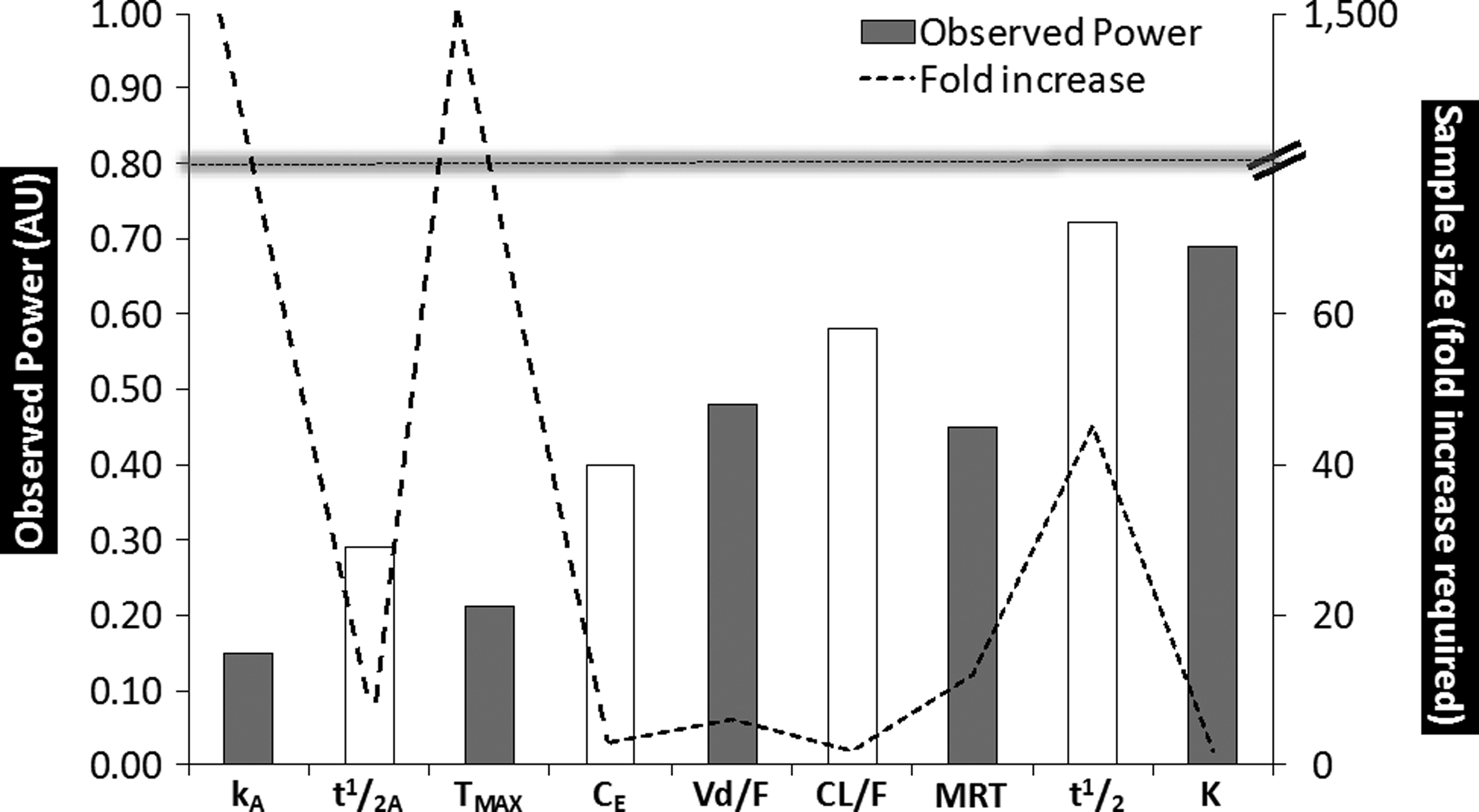
Statistical power and sample size. Data based on pooled studies for each pharmacokinetic parameter. Open bars represent those parameters that were significantly different at high altitude (p < 0.05 vs. sea level). Power (AU, arbitrary units) was retrospectively calculated and sample size (fold increase required relative to that employed) prospectively calculated based on (minimal) requisite power (1-β = 0.80, α = 0.05), as indicated; kA, absorption rate constant; t½A, absorption half-life; TMAX, time to peak plasma concentration; CE, erythrocyte binding; Vd/F, volume of distribution as a function of bioavailability; CL/F, clearance as a function of bioavailability; MRT, mean residence time (unclear if the MRT refers to global absorption + disposition residence or disposition alone); t½, elimination half-life; K, elimination rate constant.
Discussion
This systematic review and meta-analysis has revealed important changes in PK parameters that define the absorption and disposition of the, although limited, selection of medicinal drugs displaying diverse physicochemical and PK properties that may be indicative of a broader impact of the HA environment upon the body's handling of pharmaceuticals. First, by pooling relevant studies and improving statistical power, our analysis extends original works described in a published review (Hui et al., 2016) highlighting impairments in both oral absorption and corresponding clearance of drugs that (from a clinical perspective) encourage the need for closer patient monitoring and dose adjustments to maintain therapeutic efficacy and avoid incidental toxicity. Second, prospective calculations have helped inform the design of future trials highlighting the need for considerably larger sample sizes to more rigorously address PK changes and ultimately define safer, more effective pharmacological interventions at HA.
The overall outcomes of our analysis highlighted a significant prolongation in t1/2A at HA. This change in rate is not necessarily underpinned by any change in the extent of absorption [bioavailability (F)], a parameter not reported in any of the primary studies forming this meta-analysis. Our analysis would suggest that the data for sulfamethoxazole, meperidine, and lithium made the greatest contribution to the overall absorption outcomes of our study. These drugs possess different biopharmaceutical characteristics with respect to the biopharmaceutics classification system (BCS) for orally administered drugs (Kasim et al., 2004). Sulfamethoxazole is a Class IV drug (low permeability and low solubility), whereas meperidine and lithium (WHO, 2005) are Class I drugs (high permeability and high solubility). The other drugs in the analysis being acetazolamide (Class IV), furosemide (Class IV), and prednisolone (Class I). However, there is little that can be concluded from such biopharmaceutical characteristics in terms of a unifying mechanism to support a slower absorption rate at HA, and the BCS itself does not provide a definitive measure of in vivo absorption outcomes.
Acute exposure to HA is often associated with gastrointestinal complaints attributed to delayed gastric emptying, although more severe hypoxemia associated with higher elevations (>5000 m) is typically required before nutrient malabsorption becomes apparent (Bailey et al., 2000; Bailey et al., 2001; Bailey et al., 2004). The absorption of Class IV drugs such as sulfamethoxazole is generally not affected by gastric emptying, but by other complex and variable issues acting on the drug formulation within the gastrointestinal tract. Furthermore, the meperidine data in this analysis were represented as a drug delivered through the intramuscular route. Changes in hemodynamics at the absorption site (intestinal or intramuscular) could be responsible for slowed drug absorption, as indicated by one study that reported a reduction in superior mesenteric blood flow both before and following a standard meal in response to acute exposure (2 hours) to hypobaric hypoxia equivalent to a simulated altitude of 4800 m (Loshbaugh et al., 2006). Similarly, subtle effects of a hypobaric hypoxic environment upon local capillary pressures and epithelial–luminal biochemistry, including membrane carriers, metabolism, and local intestinal secretions that influence pH, could be highly relevant to the drug absorption process.
We observed a consistent increase in CE that has traditionally been attributed to an increase in Hct and/or total protein, including albumin, assuming CE includes all sources of binding in blood (Hui et al., 2016). In the current study, we specifically chose to focus our attention on acute HA exposure (<24 hours) and are thus confident that the increase in CE was unrelated to any increase in erythrocyte mass given the 2–3 day time lag between erythropoiesis and de novo appearance of reticulocytes in the circulation. Thus, the increased Hct observed likely reflects an apparent hemoconcentration subsequent to hyperventilation/diuresis-induced plasma volume contraction, notwithstanding potential increases in capillary hydrostatic and interstitial osmotic pressures that collectively drive fluid from the intravascular to the extravascular space (Fall et al., 2011).
The analysis revealed a consistent and significant trend for the CL/F parameter to be reduced at HA. The decrease in CL/F could reflect decreases in CL and/or increases in F. However, increases in F would not be consistent with a trend for a reduced rate of absorption and, moreover, the Vd/F parameter remained essentially unchanged, indicating neither Vd nor F to have changed significantly, or both parameters to have changed in a simultaneous and directly proportional manner, that is, if F were to have increased, then Vd would also need to have increased in direct proportion. In this context, while acute HA exposure can be associated with fluid extravasation, any such conductive fluid transfer would not in its own right change the effective estimate for Vd, when this estimate is based upon total drug plasma concentrations, which is indeed the case in the primary studies underpinning the analysis of this systematic review. As such, we interpret the reduced CL/F to reflect a decrease in CL per se, entirely consistent with the prolonged t½ and indeed the trend for MRT to be prolonged in the studies, although it is important to note that the method of calculation of the MRT parameter was not explicitly defined in most of the primary works. The apparent discrepancy between t½ and K (the latter not significant), although trending toward an (expected) inverse relationship, is a likely consequence of the marked heterogeneity of SMDs associated with each of the selected studies.
Previous observed or presumed decreases in drug CL at HA have more often than not been interpreted in the context of altered capacity for enzymatic metabolism, particularly diminished monooxygenase activity of CYP-450, for which O2 is a substrate (Fradette and Du Souich, 2004). However, a drug's CL (i.e., one based on measurement of total protein-bound and free drug levels) may also be impacted by changes in drug plasma protein binding. This is particularly the case for those drugs displaying medium to low extraction efficiencies across an organ(s) of elimination where a change in the fraction of unbound drug in plasma (Fu) may deliver a concordant change in a drug's total (bound and unbound) plasma CL. In the context of the current molecules and with respect to metabolism-mediated elimination, any potential HA-induced changes in Fu could possibly impact upon the CL of prednisolone and sulfamethoxazole as examples of medium to low extraction drugs. However, the CL/F of prednisolone, a drug recognized to display concentration-dependent changes in Fu (Al-Habet and Rogers, 1980; Frey et al., 1986), did not change at HA in the primary study (Arancibia et al., 2005). A number of drugs in the present analysis have limited or no metabolic elimination but rather substantial renal excretion (acetazolamide, furosemide, and lithium), but nevertheless displayed, in the primary studies, significantly reduced CL/F with HA exposure. Collectively, this raises the potential role of altered hemodynamics in HA-induced changes in CL either through direct or indirect mechanisms. The extent by which HA alters renal hemodynamics remains equivocal (Goldfarb-Rumyantzev and Alper, 2014) despite some evidence for a reduction in the glomerular filtration rate at comparable elevations (Pichler et al., 2008). Collectively, our findings are broadly consistent with those reported in the animal/in vitro literature with the reduction in drug clearance classically attributed to hypoxia, although the additional impact of other environmental stressors typically encountered at HA such as exercise and cold (highlighted in Fig. 1A) warrants investigation (Bailey, 2017).
However, these findings contrast with those reported during more controlled laboratory-based exposures to normobaric hypoxia. In one of the most rigorous trials conducted to date, 2 hours of passive exposure to a simulated altitude of 4500 m failed to alter hepatic blood flow and corresponding metabolism of theophylline (low hepatic extraction ratio metabolized mainly by CYP1A2) and verapamil (high hepatic extraction ratio metabolized mainly by CYP3A4), arguing against the need for dose adjustment (Streit et al., 2005). Differences between normobaric and hypobaric hypoxia (Millet et al., 2012) notwithstanding the contributory impact of additional stimuli such as exercise, cold, and psychological stress exclusive to terrestrial ascent (Peng and Cheung, 2009; Peng and Cheung, 2011; Bailey, 2017) may contribute, at least in part, to these conflicting findings and clearly highlight the need for further research.
Limitations
It is important to recognize the limitations associated with the current meta-analysis. Our findings are restricted to participants of either Chilean or Chinese descent and thus the interpretive implications for other ethnic groups remain unclear, especially given established differences in the catalytic activities of CYP-450 isoforms (Yang et al., 2012). Furthermore and subject to inclusion/exclusion criteria, our analysis was confined to a limited selection of compounds that exhibit diverse clearance pathways and thus it is unlikely that changes in active tubular ion exchange, oxidative metabolism, phase II pathways such as N-acetylation, sulfation, and glucuronidation, or active tubular efflux can collectively be ascribed to a single common mechanism induced by HA. The situation is clearly more complex, further complicated by exposure to multiple stressors whose independent and combined impacts on drug PKs remain largely unknown. Equally, it may be considered pharmacologically unfounded to pool study data from such physiochemically diverse compounds, the fundamental basis of a meta-analysis, although we have adhered to stringent guidelines (Walker et al., 2008; Knobloch et al., 2011), including a description and evaluation of heterogeneity, to optimize the validity of our findings.
Conclusions
This analysis reveals impairments in both oral absorption and corresponding clearance of the, although limited, sample of drugs that exhibit diverse clearance pathways that may potentially require modifications in dosage regimens to maintain efficacy or prevent toxicity especially for those with a narrow therapeutic index. Given that studies have traditionally been underpowered, characterized by a high degree of variability and relatively small effect sizes, larger scale, randomized controlled trials in humans are encouraged to better define safer and more effective pharmacological interventions at HA, including the experimental (laboratory-based) isolation of independent and combined influences of the composite PK-modulating stressors (hypoxia, exercise, and cold). Given the prevalence of drug use at HA (Donegani et al., 2016), it would seem reasonable to extend PK research to other commonly used drugs for prevention and treatment of HA illness, including AMS, HAPE, and HACE, as recently highlighted (Nieto Estrada et al., 2017), namely steroids (budesonide, dexamethasone), bronchodilators (salmeterol, theophylline or aminophylline, montelukast), phosphodiesterase 5-inhibitors (tadalafil, sildenafil), calcium channel modulators (nifedipine, flunarizine), nonsteroidal anti-inflammatories, and other analgesics (aspirin, carbasalate, and ibuprofen). Furthermore, it would be equally important to include those drugs commonly prescribed to treat pre-existing cardiovascular, cerebrovascular, metabolic, endocrine, and pulmonary diseases within a tourist population (antiplatelets, statins, β-blockers, nitrates, angiotensin-converting enzyme inhibitors, and angiotensin II receptor antagonists).
Contributors
D.M.B. contributed to the conception and design of the study. D.M.B. and B.S.S. contributed to development of the search strategy. D.M.B. and B.S.S. conducted the systematic search. D.M.B. and B.S.S. completed the acquisition of data and performed the data analysis. M.G. provided specialist pharmacological input. All authors assisted with the interpretation. D.M.B. wrote the first draft of the manuscript. All authors contributed to drafting and revision of the final article. All authors approved the final submitted version of the manuscript.
Footnotes
Acknowledgments
D.M. Bailey is a Royal Society Wolfson Research Fellow (# WM170007) and received funding from the Higher Education Funding Council of Wales to support B.S.S.'s PhD scholarship.
Author Disclosure Statement
All authors declare no conflict of financial interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.