
Abstract
Abstract
Wang, Chi, Hui Jiang, Jinyan Duan, Jingwen Chen, Qi Wang, Xiaoting Liu, and Chengbin Wang. Exploration of acute phase proteins and inflammatory cytokines in early stage diagnosis of acute mountain sickness. High Alt Med Biol. 19:170–177, 2018.
Background:
Early diagnosis of acute mountain sickness (AMS) is currently based on personal appreciation of the severity of symptoms. A more objective method to diagnose AMS is required. Inflammatory cytokines and acute phase proteins have been reported to be different at high altitude.
Methods:
A total of 104 male soldiers rapidly ascending from Beijing (20–60 m) to Germu, Qinghai (3200 m), were divided into AMS group and non-AMS group according to the Lake Louis Score system. Blood pressure, pulse rate, and oxygen saturation were measured. Forty-nine blood samples were collected before and on the 3rd day after ascending to the high altitude. Serum haptoglobin (Hp), transferrin (Tf), and complement C3 were detected by immune scattered nephelometry, whereas serum interleukin-1beta (IL-1β), IL-6, and tumor necrosis factor-α (TNF-α) were detected by chemical luminescence immunity analyzer. The sensitivity, specificity, and receiver operating characteristic curve were evaluated. Youden index with the maximum value was used to determine cutoff values of each parameter. Logistic regression was performed to determine the diagnostic efficiency of combination of three cytokines.
Results:
Differences of physical indexes between AMS group and non-AMS group were of no statistical significance. In AMS group, serum Tf significantly increased while Hp decreased when compared with non-AMS group. Serum IL-1β, IL-6, and TNF-α were higher in the AMS group than in the non-AMS group. The cutoff values for Tf, Hp, IL-1β, IL-6, and TNF-α were 263.5 mg/dL, 119.35 mg/dL, 6.2 pg/mL, 15.05 pg/mL, and 18.35 pg/mL, respectively. Area under the curve (AUC) of combining three cytokines together was higher than AUC of each cytokine separately.
Conclusions:
Acute phase proteins and inflammatory cytokines (IL-1β, IL-6, and TNF-α) show significant changes between the AMS group and the non-AMS group. Combination of inflammatory cytokines or acute phase proteins improves the specificity for diagnosis of AMS. This might provide objective indexes for scanning and screening individuals susceptible to AMS in the early stage of rapid ascending.
Background
H
The most frequently used criteria for AMS are based on the self-reported Lake Louise consensus scoring system (LLS), which was generally accepted on the eighth international hypoxia conference (Savourey et al., 1995). LLS depends on the subjects' personal appreciation of the severity of symptoms, including headache, gastrointestinal upset, fatigue, dizziness, and insomnia. Whereas, as a categorical score, LLS lacks the quantification of a continuous spectrum of disease severity and statistical analysis, which make it difficult to quantitatively compare different symptoms (Hall et al., 2014). Owing to the inconspicuous and hidden onset of AMS, early diagnosis is difficult to make simply based on these subjective symptoms, thus leading to delay in treatment.
Ascending to high altitudes can modify metabolic and physiological functions, whereas body homeostasis reestablishment occurs under the condition of hypoxia (Mazzeo et al., 2000). Hypoxia leads to multiple changes in physiological system, such as hematopoietic, respiratory, or sympathetic nervous function (Rohm et al., 2015). In addition, hypoxia has been indicated to trigger vascular inflammation, which leads to increased vascular permeability, leukocyte adherence, and leukocyte emigration (Wood et al., 2000; Jung et al., 2012; Lam et al., 2012). Exposure to hypoxia promotes expression of transcription factors, including nuclear factor-κB (NF-κB), which plays a central role in stimulating the release of proinflammatory cytokines (Taylor, 2008).
Proinflammatory cytokines including interleukin-1beta (IL-1β), IL-6, and tumor necrosis factor-α (TNF-α) have been suggested to increase under the condition of hypoxia (Dosek et al., 2007; Seys et al., 2013). IL-1β, IL-6, and TNF-α are proinflammatory interleukins released by activated T cells and macrophages (Boos et al., 2016). However, in published articles (Kleger et al., 1996; Swenson et al., 1997; Bailey et al., 2004), researchers found that elevation of these proinflammatory cytokines was not significant enough, which also encouraged us to further the study about this.
In addition, acute exposure to elevated altitudes can result in changes of immunological parameters (Thake et al., 2004; Mazzeo, 2005). Acute phase proteins including haptoglobin (Hp), transferrin (Tf), and complement C3 have been found to change between individuals at sea level and at high altitude through plasma proteome (Ahmad et al., 2013). However, whether these parameters differentiate between the AMS and non-AMS people is rarely discussed.
Therefore, one of the main research objects of high-altitude medicine is to make full use of local laboratory resources and dig out effective diagnostic indexes for AMS. Based on these requirements, our study collected plasma samples from healthy young men both at sea level and at high altitude. We compared the level of serum inflammatory cytokines and acute phase proteins and figured out the diagnostic value of these indexes. In addition, we aim to test whether the combination of these parameters could generate a higher diagnostic efficiency of AMS.
Materials and Methods
Subject recruitment
All subjects were well informed of the study and they provided their written informed consent. A total of 104 healthy male volunteers, who ascended together from Beijing (20–60 m) to Germu, Qinghai (3200 m), by train within 48 hours, were recruited for this study. Inclusion criteria were as follows: absence of acute infection during the past 6 months, absence of chronic inflammatory diseases, with no organic diseases, with the age >18 years, and >6 months stay at sea level. We also excluded subjects with high blood pressure (BP) or its complications, with mental diseases, age >50 years, or subjects who had been to high altitude during the past 6 months. All subjects are Han Chinese men without blood relationship. The Ethics Committee of the People's Liberation Army General Hospital approved the study protocol.
Self-assessment of symptoms from questionnaires
AMS diagnosis was based on the self-assessment of LLS system of symptoms. Questionnaires based on LLS system were designed and sent out to volunteers on the third morning after arriving at Germu. General information including age, body mass index, smoking history, underlying health problems, past experience related to high altitude, means of transport, and preventative treatment were also acquired through questionnaires. In addition, five symptoms including headache, gastrointestinal symptoms, fatigue/weakness, dizziness/lightheadedness, and difficulty in sleeping were assessed. Participants scored the severity of each symptom from 0 (no symptom) to 3 (maximal severity). Individuals whose total score exceeded >3 and were accompanied with headache were diagnosed as AMS. Based on the LLS system, volunteers were divided into AMS group and non-AMS group.
Measurement of physiological indexes
Primary physiological indexes including BP, oxygen saturation (SpO2), and pulse rate were detected both at sea level (Beijing) and on the third morning after arriving at high altitude (Germu). BP measurements were performed after 5 minutes of inactivity. Arm BP monitor (KD-5903; Andon Health Co., Ltd. Tianjin) was used to determine brachial artery BP of each volunteer for three times and average value was acquired. SpO2 of fingertip and pulse rate were measured with pulse oximeter (YX301; Yuwell Medical Equipment & Supply Co., Ltd., Jiangsu), both of which were performed on right index fingers in the morning before breakfast.
Blood sample collection and conservation
Fasting venous blood (with EDTA as an anticoagulant) was obtained via antecubital vein from 49 individuals both in Beijing and on the third morning after arriving at Germu. Plasma was separated immediately by centrifugation (3000 g, 5 minutes). The harvested plasma samples were then aliquoted into polystyrene tubes, then transported to Beijing in dry ice and stored at −80°C until further analysis.
Measurement of acute phase proteins and inflammatory cytokines
Plasma concentrations of Hp, Tf, and complement C3 (C3) were determined with immune scattered nephelometry analyzer (BN II System; Siemens Healthcare Diagnostic, Inc.). Plasma concentrations of inflammatory cytokines (IL-1β, IL-6, and TNF-α) were determined with chemical luminescence immunity analyzer (Immulite 1000; Siemens Healthcare Diagnostic, Inc.). All manipulations were performed critically in accordance with the manufacturer's instructions and all kits originated from manufacturers.
Statistical analysis
All data were analyzed with SPSS software (version 17.0; IBM) and all figures were created using GraphPad Prism (version 6.0). All data are presented as mean ± standard deviation. Normal distribution was checked with Kolmogorov–Smirnov test and confirmed by frequency histograms and analysis of skew. t-Test was performed to compare the differences of physical indexes, including BP, heart rate, and SpO2. Repeated-measures analysis of variance was performed to compare the changes of targeted proteins and cytokines at sea level and at high altitude. Altitude and AMS status were included as main effects, whereas AMS status × altitude was considered as interaction term to observe whether there was interaction effect.
Variables that differed significantly (p < 0.05) between the AMS group and the non-AMS group were assessed further by a receiver operating characteristic (ROC) curve analysis, which was performed by calculating the sensitivity and specificity. The area under the curve (AUC) and 95% CI were calculated for each ROC curve. Maximum of Youden index (sensitivity+specificity–1) was calculated to determine cutoff values of each parameter (Habibzadeh et al., 2016).
Logistic regression models were developed in a forward stepwise manner. The best laboratory variable was retained in the model. Additional variables were then added to that two-variable model. Once the addition of additional variables did not improve the model (candidate model), individual variables were removed from that model, and interactions of variables in that model were included and the results compared with the candidate model; thus, it was determined whether the addition or removal of a variable changed the effects of other variables. Variables that improved the model prediction were retained. By use of this approach, sensitivity and specificity of the model were calculated and an ROC curve was constructed. Significance for all analysis was based on p < 0.05.
Results
General subject characteristics
The volunteers with an average age of 30 ± 5.1 years, height of 176.5 ± 8.7 cm, and weight of 78.2 ± 10.2 kg were divided into AMS group and non-AMS group based on the LLS system. Two questionnaires were incomplete and excluded. Among the 102 qualified volunteers, 58 volunteers were identified as AMS, which accounted for 56.7% of all the volunteers. Among the 49 volunteers whose blood samples were obtained both at sea level and at high altitude, 24 of them suffered from AMS and the other 25 were non-AMS based on LLS. All occurred symptoms and their percentages are shown in Table 1.
AMS, acute mountain sickness.
Changes of physical indexes
Systolic blood pressure (SBP) (113.8 ± 8.4 mmHg at sea level vs. 119.2 ± 10.2 mmHg at high altitude), diastolic blood pressure (DBP) (82.4 ± 5.2 mmHg at sea level vs. 89.1 ± 8.3 mmHg at high altitude), and pulse rate (70.3 ± 9.2 at sea level vs. 80.9 ± 8.3 at high altitude) of volunteers at high altitude were higher than those at sea level, whereas SpO2 (98.4 ± 1.2 at sea level vs. 88.4 ± 7.2 at high altitude) was lower at high altitude (p < 0.05, Table 2). Whereas differences of BP, SpO2, and pulse rate between the AMS group and the non-AMS group were of no statistical significance (p > 0.05, Table 2).
p > 0.05 compared with AMS group.
DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure; SpO2, oxygen saturation.
Plasma inflammatory cytokine levels were significantly higher in the AMS group than in the non-AMS group
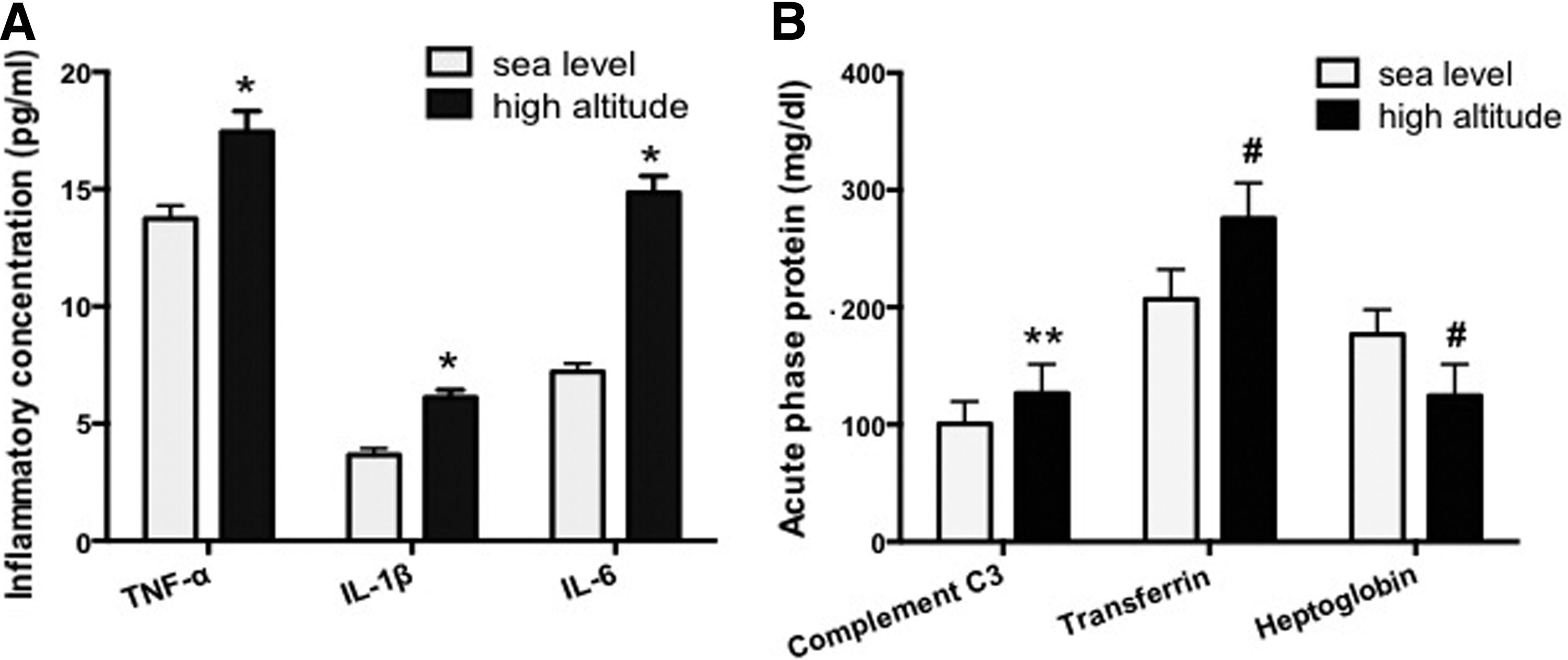
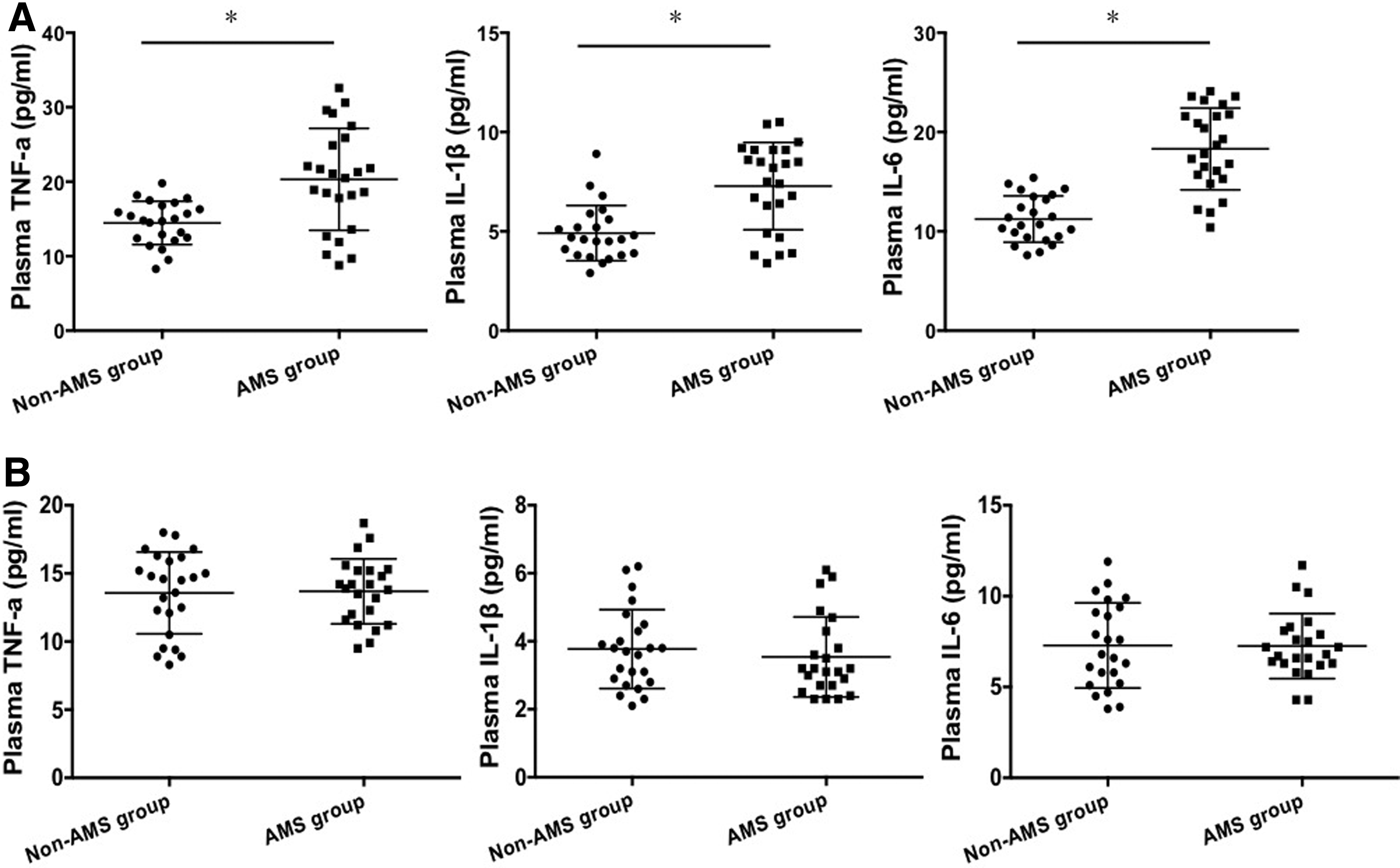
The interaction between AMS status and altitude was of no statistical significance (p > 0.05). Mean concentrations of IL-1β, IL-6, and TNF-α at sea level (3.67, 7.21, and 13.74 pg/mL, respectively) were significantly lower than those on the 3rd day after arriving at high altitude (6.12, 14.84, and 17.45 pg/mL, respectively, Fig. 1A). These inflammatory cytokines in the AMS group were significantly higher than those in the non-AMS group at high altitude (p < 0.05, Fig. 2A). Then we compared the levels of cytokines at sea level based on the LLS result and found that these cytokines had no statistical difference between the AMS group and the non-AMS group at sea level (p > 0.05, Fig. 2B). Among the three cytokines, sensitivity of IL-6 (79.2%) is higher than that of IL-1β (75%) and TNF-α (66.7%). Specificity of IL-6 (95.7%) is also higher than that of IL-1β (87%) and TNF-α (91.7%). The cutoff values for IL-1β, IL-6, and TNF-α were 6.2, 15.05, and 18.35 pg/mL, respectively (Table 3).
High altitude induced significant changes of serum proteins (n = 49).
Comparison of plasma inflammatory cytokines (IL-1β, IL-6, and TNF-α) between the AMS group and the non-AMS group both at sea level and at high altitude (n = 49).
AUC, area under the curve; Hp, haptoglobin; IL-1β, interleukin-1beta; Tf, transferring; TNF-α, tumor necrosis factor-α.
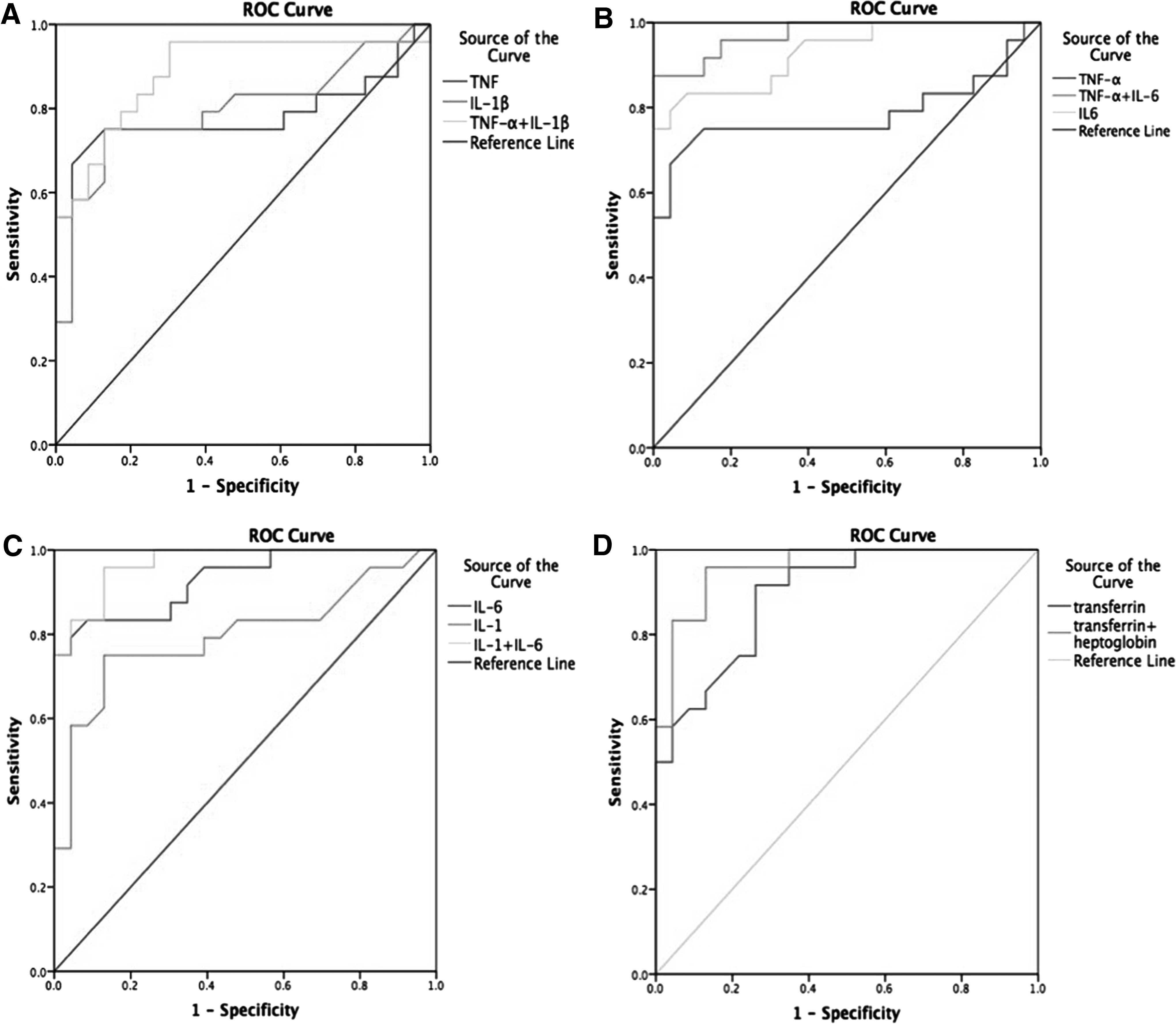
In addition, logistic regression models in a forward stepwise manner were developed. Only two of the cytokines could exist in each equation, which generated three different types of combination (TNF-α and IL-1β, TNF-α and IL-6, and IL-6 and IL-1β). By use of this approach, sensitivity and specificity of the model were calculated and an ROC curve was constructed. AUCs of TNF-α and IL-1β, TNF-α and IL-6, and IL-6 and IL-1β were 0.886, 0.973, and 0.969, respectively. All of these were higher than the AUC of each cytokine alone (AUCs of IL-1β, IL-6, and TNF-α were 0.797, 0.929, and 0.783, respectively) (Fig. 4A–C). Sensitivity and specificity increased after combining two cytokines together: the specificity of combining TNF-α and IL-6 was 95.7%; the sensitivity of combining IL-1β and IL-6 was 91.6% (Table 3).
Changes of plasma acute phase proteins' concentrations vary at high altitude and in the AMS group
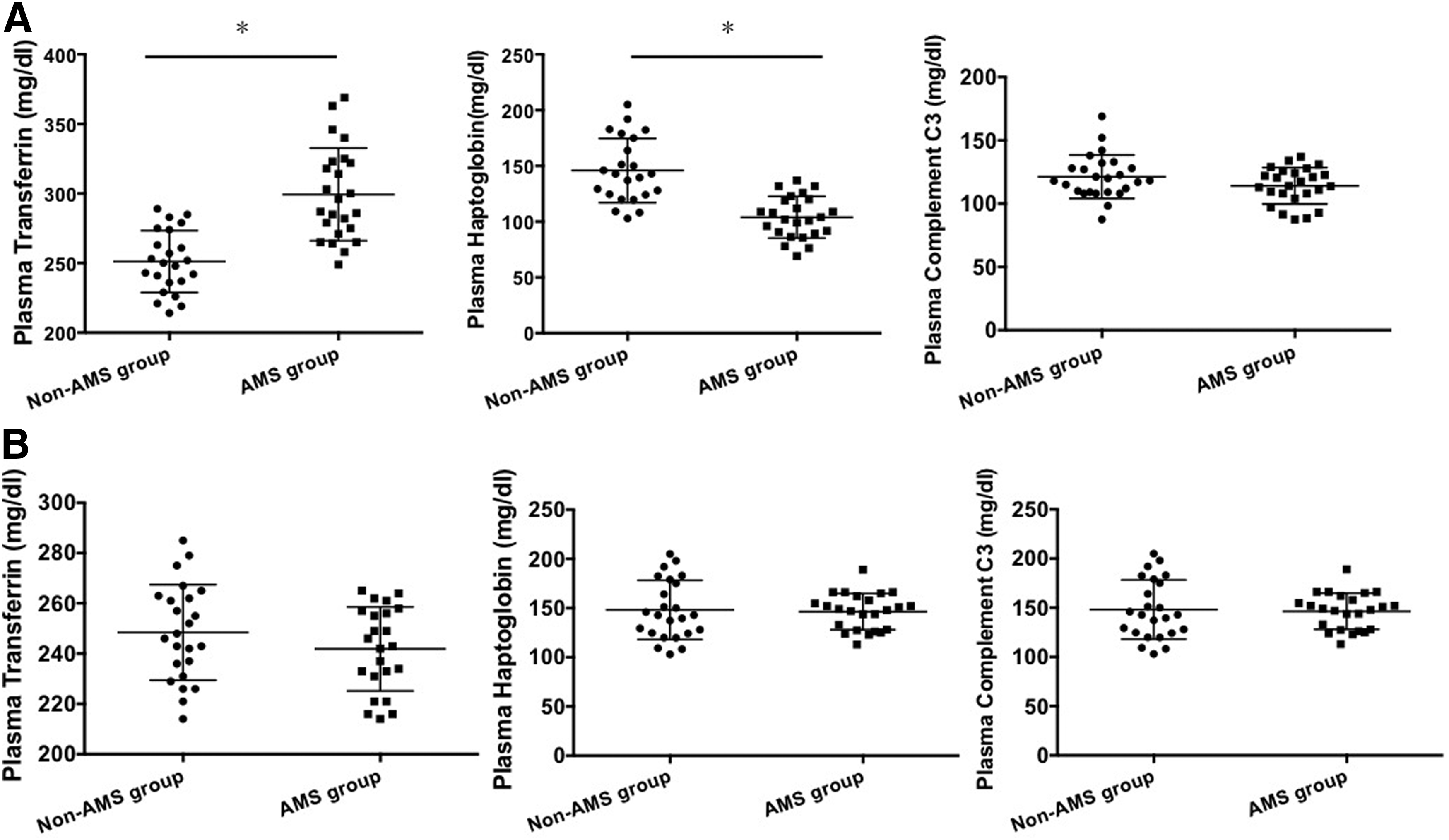
Plasma Tf and complement C3 increased on the 3rd day after ascending to high altitude, whereas Hp decreased when compared with those at sea level (Fig. 1B). Tf of the AMS group (299.38 ± 33.33 mg/dL) significantly increased when compared with that of the non-AMS group (251.17 ± 22.23 mg/dL, p < 0.05); whereas Hp of the AMS group (104.01 ± 18.71 mg/dL) was lower than that of the non-AMS group (145.93 ± 28.80 mg/dL, p < 0.05, Fig. 3). However, complement C3 had no significant difference between the AMS group and the non-AMS group. We compared the levels of acute proteins at sea level based on the LLS result and found that these proteins had no statistical difference between the AMS group and the non-AMS group at sea level (p > 0.05, Fig. 3B). Sensitivities of Tf and Hp were 91.7% and 87%, respectively, whereas specificities were 74.9% and 75%, respectively. Cutoff values of Tf and Hp were 263.5 and 119.35 mg/dL, respectively (Table 3).
Comparison of plasma acute phase proteins (Tf, Hp, complement C3) between the AMS group and the non-AMS group both at sea level and at high altitude (n = 49).
A combination of Tf and Hp showed an increase in the diagnostic value: with an AUC of 0.958, higher than that of either Tf (0.894) or Hp (0.899) (Fig. 4D). The sensitivity and specificity of the combined indexes were 95.8% and 87%, respectively, which were also higher than those of each protein alone (Table 3).
ROC of inflammatory cytokines and acute phase proteins and the combination of several biomarkers.
Discussion
China is one of the countries with the largest area of high altitude in the world. With the advent of economical construction, tourism development, and tensed military relationship with surrounding areas, the number of individuals ascending plateau rises drastically. This causes the elevated incidence of high-altitude sickness to vary from 40% to 80% based on the specific altitude and the speed of ascend (Waeber et al., 2015). The present international consensus defines AMS as a spectrum of nonspecific symptoms experienced after exposure to high altitude (West, 2011). An LLS of ≥3 points confirmed the diagnosis of AMS, whereas a score of ≥5 points was defined as severe AMS (Chen et al., 2013).
Changes in lung or brain imaging appear later than symptoms, which indicate the occurrence of lung or brain edema. Physiological index including arterial BP, SpO2, blood gas analysis, pulmonary function, and echocardiogram can also indicate AMS and are present at high altitude (Rhodes et al., 2011; Guo et al., 2014). However, researchers have found that the prediction of AMS using these indexes varied individually and the relationship between these indexes and AMS is not entirely clear (West, 2014). Our study indicated that there was no statistical significance between the AMS group and the non-AMS group in terms of SBP, DBP, heart rate (HR), and SpO2 (%), which paralleled other studies (Chen et al., 2012; Wagner et al., 2012; Song et al., 2013). Although the LLS system is currently regarded as the diagnostic standard, there still lacks efficient and precise quantitative markers to identify AMS at early stage (Shah et al., 2015).
Therefore, this study focused on the quantitative and precise diagnosis of AMS using serum acute phase proteins and proinflammatory cytokines. We found that high-altitude exposure induced an increase of circulating TNF-α, IL-1β, and IL-6 in human plasma, which was in accordance with previous literature (Hartmann et al., 2000). In addition, we compared the level of these cytokines between the AMS group and the non-AMS group and found that there was a statistical significance in all these three cytokines. The ROC curve indicated that the specificity of each cytokine alone varied from 87% to 95.7%, whereas the sensitivity varied from 85.8% to 91.6%.
There is striking evidence that IL-6 may be involved in hypoxia-induced lung inflammation and pulmonary vascular remodeling and is possibly responsible for the occurrence of high-altitude diseases (Savale et al., 2009). Synthesis of IL-6 is stimulated by TNF and IL-1, which has been identified as a critical mediator of inflammation in tissues (Li et al., 2015). An increasing number of articles indicated a correlation between systematic inflammatory response and AMS since hypoxia was shown to alter cellular immunity as well as cytokine release. Boos et al. (2016) reported the increase of IL-6 and IL-17a at high altitude and these cytokines were correlated with high-altitude exercise. In addition, Lu et al. (2016) identified four cytokines including IGFBP6 (insulin-like growth factor binding protein 6), Dkk4 (dickkopf WNT signaling pathway inhibitor 4), SAA1 (serum amyloid A1), and IL-17RA (interleukin 17 receptor A), which might be predictable for AMS susceptibility in a low-altitude environment. Liu et al. (2017) found IL-10 dysregulation, which was involved in immune and inflammatory responses, in AMS through transcriptome analysis. The reduction of IL-10 after exposure to high altitude presented strong correlation with AMS.
Besides the proinflammatory cytokines, specific acute phase proteins have also been demonstrated to change under the condition of high altitude. Hypobaric hypoxia is a pathophysiological condition triggering disturbances of cell organization, leading to proteins, lipids, or DNA damage through oxidative stress (Singh et al., 2010). Ahmad et al. (2013, 2014) studied changes in both the human and rat plasma proteome under the condition of high altitude using the proteomic approach. Among the upregulated and downregulated proteins in plasma, acute phase proteins including Hp, Tf, and complement C3 signify.
In addition, Padhy et al. (Bowman and Kurosky, 1982; Padhy et al., 2013) also found an increase in plasma Hp in rats tolerant of hypobaric hypoxia. Hp is an acute phase protein that functions as an antioxidant by virtue of its ability to bind to hemoglobin (Bowman and Kurosky, 1982). This important protective mechanism has been illustrated in Hp knockout mice in which oxidative tissue damage develops in response to hemolysis (Lim et al., 1998). Possessing both anti-inflammatory and antioxidative properties, it forms a complex with free hemoglobin released as a result of cell membrane damage by reactive oxygen species (Pimenova et al., 2010). In addition, it has been demonstrated that expression level of Hp is regulated by several cytokines, including IL-1, IL-6, TNF-α, and TGF-β. Plasma Hp significantly increased when compared with sea level. Whereas the difference between the AMS group and the non-AMS group attracts our interest, and we found that Hp might be regarded as a diagnostic marker for early stage AMS with a sensitivity of 87% and a specificity of 75%.
Iron, which is incorporated in the newly synthesized hemoglobin throughout erythropoiesis, plays an important role in protecting the organism from hypobaric hypoxia (Handelman and Levin, 2008). Tf is an important constituent of the iron homeostasis system, regulating cellular iron levels (Lok and Ponka, 1999). Evidence from cell culture studies indicates that HIF-1 induces Tf transcription under hypoxic conditions (Tacchini et al., 1999). Recent research has indicated that iron supplementation at high altitudes induced histopathological changes to lung tissues of rats that could be mediated through production of ROS and induction of inflammatory mediators (Salama et al., 2014). All the mentioned studies prove that Tf might play a critical role in the pathophysiological mechanism of high altitude. The finding of this study indicates that there is an upregulation in plasma Tf in individuals after they ascend from sea level to high altitude. Tf in the AMS group is higher when compared with the non-AMS group.
The complement system plays a major role in body defense as part of the innate and adaptive immune systems for cellular integrity and tissue homeostasis (Cook and Botto, 2006). Complement components C3 and C4a have been implicated as biomarkers of idiopathic pulmonary hypertension (Abdul-Salam et al., 2006). A recent study proves that deficiency of C3 attenuates chronic hypoxia-induced pulmonary hypertension in mice (Bauer et al., 2011). In our study, the level of complement C3 was found upregulated after arriving at high altitude but no difference between the AMS group and the non-AMS group. We, therefore, analyzed comprehensively Hp and Tf together and found a slight increase in the diagnostic value when identifying AMS from non-AMS.
Limitations of our study include the number of subjects, which might not generate precise cutoff values for AMS diagnosis. In addition, due to the extreme environment at high altitude, we could not obtain blood samples in the following days, thus not being able to make a vertical comparison and observe the dynamic changes of these indexes.
In conclusion, this study further verifies the increase of inflammatory cytokines, including IL-1β, IL-6, and TNF-α at high altitude and found there was a higher increase in the AMS group. We also determined the cutoff values for identification of AMS with these cytokines. We then demonstrated that acute phase proteins (Hp and Tf) might also be used as diagnostic markers for early stage AMS.
Footnotes
Author Disclosure Statement
No competing financial interests exist.