
Abstract
Abstract
The number of avalanche accidents involving winter recreationists has notably increased in recent decades due to the increasing popularity of outdoor winter activities. The International Liaison Committee on Cardiopulmonary Resuscitation, the International Commission for Mountain Emergency Medicine (ICAR Medcom), and the Wilderness Medical Society have recently published evidenced-based recommendations for the on-site treatment of snow avalanche victims. Despite these recommendations, recent studies found poor knowledge and compliance by both healthcare providers and laypersons. The aim of this nonsystematic review is to provide an updated overview of avalanche accident epidemiology, to present recent advances in snow avalanche pathophysiology, and to discuss recent advancements in on-site treatment of snow avalanche victims.
Introduction
S
Underlying Epidemiological Considerations
Recreational activities that expose individuals to avalanche accidents are not only exclusive to high-risk winter season pursuits such as backcountry skiing and snowshoeing but also to snowmobile use and all occupational or recreational mountain activities (e.g., ice climbing and mountaineering) (Haegeli et al., 2011; Procter et al., 2014; Pasquier et al., 2017). However, backcountry skiers and snowboarders are considered the largest group of all annual avalanche accidents in Europe, closely followed by off-piste accidents (Haegeli et al., 2011). Whereas snowmobilers are currently one of the largest group of all annual avalanche accidents in the United States and Canada (Haegeli et al., 2011; Jekich et al., 2016). Summer snow avalanche occurrence (6% of total avalanche fatal accidents in a Swiss study) reportedly involved mainly individuals engaged in mountaineering (Pasquier et al., 2017), similarly to avalanches in open terrain in the Andes and the Himalaya (Stokes et al., 2015).
Between 1983 and 2010, the annual number of avalanche fatalities involving winter recreationists in Europe and the United States and Canada was stable at ∼165 per year (∼130 per year in Europe and 36 per year in the United States and Canada) (International Commission for Alpine Rescue, 2016). Backcountry recreationists account for ∼50% of all annual avalanche fatalities in European alpine countries (Haegeli et al., 2011; Techel et al., 2016; Höller, 2017) and up to ∼60% in the United States and Canada, where overall snowmobile use accounted for ∼20%–25% of fatalities (Haegeli et al., 2011; Jekich et al., 2016). In comparison, avalanche fatalities are not systematically reported in developing countries or other remote mountainous regions, for example, areas of the Andes and the Himalaya.
Recent data from avalanche accidents in Austria, Canada, and Switzerland confirm previous assertions from Brugger et al. (2001) related to survival in completely buried avalanche victims (from 48% to 56%) (Haegeli et al., 2011; Procter et al., 2016). Specifically, the latest avalanche survival curves of completely buried avalanche victims from Austria and Switzerland (data from the period 2005–2013) (Fig. 1) (Procter et al., 2016) are similar to the survival curve published previously using an earlier data set from Switzerland (data from the period 1980–2005) (Haegeli et al., 2011). Overall, data in both curves demonstrate a rapid initial drop in survival probability to 87%–91% (after only burial duration of ∼7–10 minutes compared with ∼18 minutes of the previous survival curve), followed by a second drop to a survival probability of 25%–28% after ∼35 minutes, where an inflection point exists and the curve levels off until 180 minutes (Procter et al., 2016). A further avalanche survival curve, calculated in 2011 using data from Canadian avalanche accidents, also showed a similar rapid initial drop to a lower survival probability (77%), but in the parallel second drop, the survival probability was calculated to be as low as only 4% (i.e., poorer survival associated with longer burials) (Haegeli et al., 2011). However, the incidence of traumatic injuries, predominant snow climate, plus longer rescue and transport times in Canada versus Europe seems to explain the observed difference in Canada versus Austria and Switzerland (Haegeli et al., 2011; Procter et al., 2016). Nevertheless, avalanche survival curves specific to backcountry skiing, off-piste skiing, and snowmobiling did not differ significantly based on data from Canada (Haegeli et al., 2011).
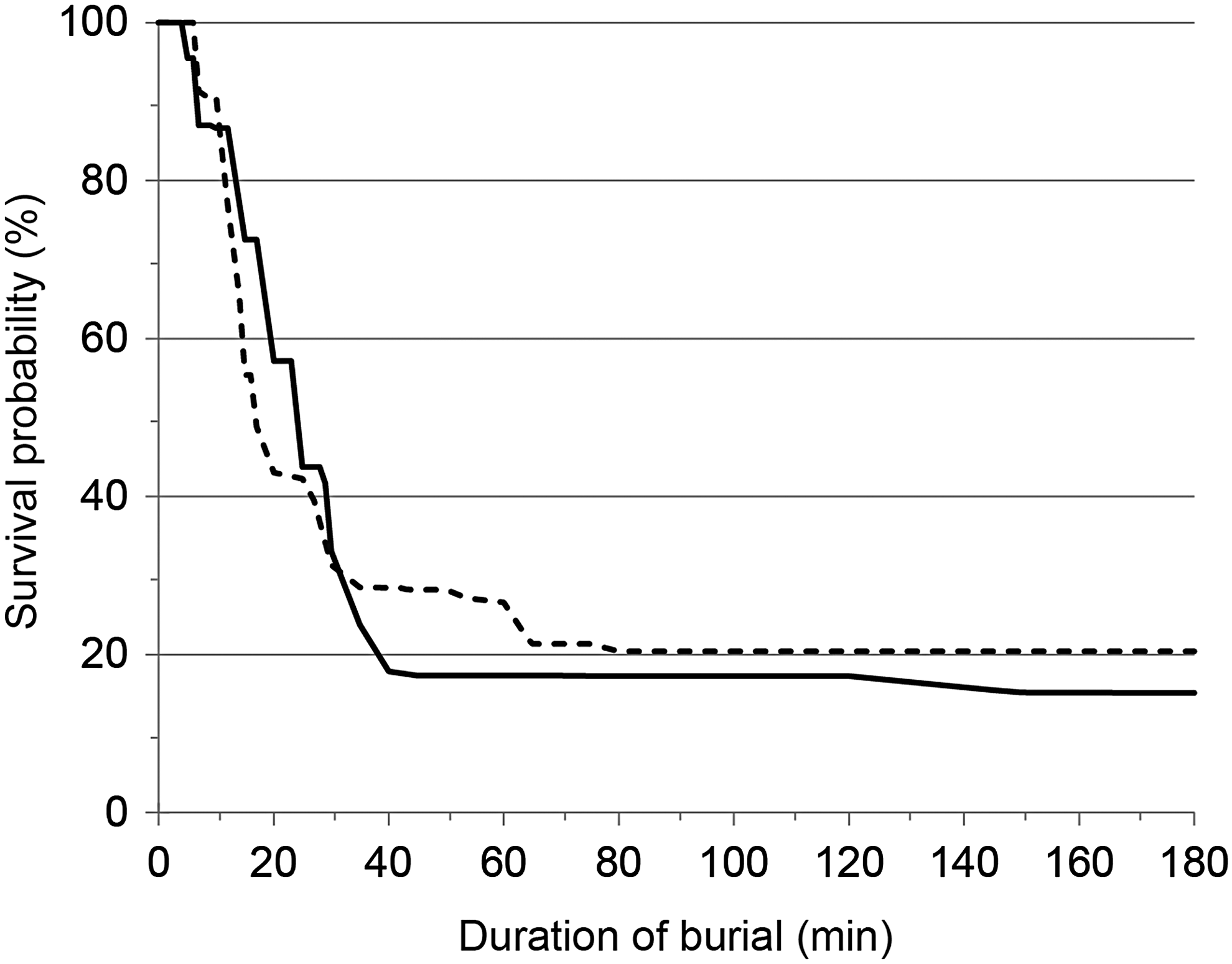
Survival curve for Austria (solid line; n = 333) and Switzerland (dashed line; n = 300) for completely buried victims between 2005 and 2013 [modified from Procter et al. (2016) with permission from Elsevier].
Underlying Pathophysiological Considerations
Survival analyses have shown that for a snow avalanche victim, the grade of burial (complete/partial) is the most determinant factor of survival, followed by duration of burial, patency of the airways, and mechanical injuries (Brugger et al., 2013). The different pathophysiological mechanisms can be temporally and quantitatively related to the phases of all available avalanche survival curves (Brugger et al., 2001; Haegeli et al., 2011; Procter et al., 2016). Trauma is the first cause of death in the initial (survival) phase, asphyxia is the main cause of death but is mainly related to the second (asphyxia) phase, and finally the combination of severe hypothermia, hypoxia, and hypercapnia (triple H syndrome) is the cause of death when the victim remains buried and the curve levels off (latent and long-term survival phases) (Brugger et al., 2013). Thus, if the pathophysiology of trauma in avalanche victims is mainly related to the type of injuries sustained during avalanche descent, the pathophysiology of avalanche burial is a unique situation determined by possibility to breath under snow debris and the total duration of burial length.
Several studies showed that breathing under avalanche debris is possible in the presence of a patent airway (Grissom et al., 2000, 2004; Brugger et al., 2003; Paal et al., 2013); new studies confirmed previous observations and showed that (i) breathing under the snow is possible even with only a “virtual” air pocket (i.e., any space in front of mouth and nose) with significantly increased work of breathing initially (Roubík et al., 2015) and (ii) a larger (although unknown) air volume from the surrounding snow is available to enable prolonged breathing under snow, thanks to gas diffusivity (Fig. 2) (Strapazzon et al., 2017a). Specifically, this study from Strapazzon et al. (2017a) demonstrated that the decrease in SpO2 in participants breathing from a predefined snow air pocket was much less than that observed in participants breathing into a flexible plastic bag of the same volume (i.e., SpO2 >75% up to 30 minutes in 50% of study participants versus <4 minutes in 100% of the latter). Higher snow densities were associated with the speed of decrease in O2 and increase in CO2 as measured in the air pocket, leading to premature interruption of some tests due to SpO2 falling less than the predefined safety criteria (SpO2 ≤75%) (Strapazzon et al., 2017a). These data provide an experimentally supported explanation to those epidemiological observations from Canadian avalanche accidents, that there is potentially a different survival pattern in relation to high snow density (i.e., maritime snow climate due to mild temperatures) versus low snow density (i.e., continental snow climate due to cold temperatures) (Haegeli et al., 2011). Moreover, the presence of an air pocket favors a later onset of hypoxemia based on its volume (Brugger et al., 2003), and new epidemiological data have shown that there was a lower survival within avalanche victims from Austria without an air pocket compared with those with an air pocket (of the victims buried ≤15 minutes, 69% without an air pocket survived compared with 95% with an air pocket [p < 0.001]; if the victims were buried >15 minutes, only 4% without an air pocket survived compared with 67% with an air pocket [p < 0.001]) (Procter et al., 2016).
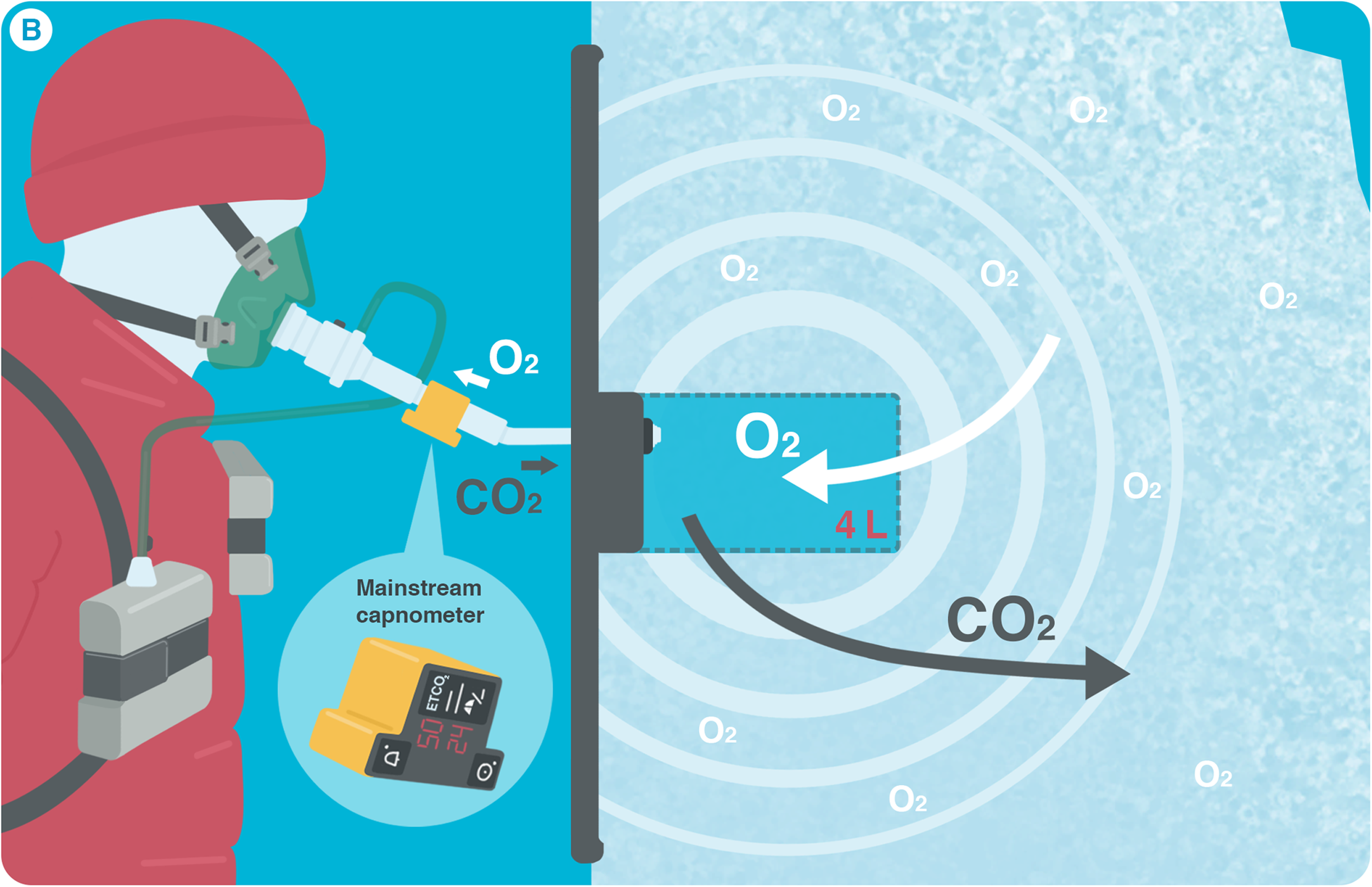
Breathing into an artificial snow avalanche. Snow is a highly porous medium containing high amounts of interstitial air (e.g., ∼70% air with a snow density of 300 kg/m3). The porosity of the snow seems to favor O2 diffusion from snow debris into the air pocket and exhaled CO2 adsorption into the surrounding snow. CO2, carbon dioxide; ETCO2, end-tidal CO2; L, liter, O2, oxygen [modified from Strapazzon et al. (2016) with permission from Springer Nature].
When there is a long burial time (i.e., >35–60 minutes), a hypothermic avalanche victim shows a level of consciousness, as well as cardiovascular and respiratory parameters, which are rarely determined only by effect of core temperature: traumatic injuries as well as O2 and CO2 levels usually complicate pathophysiology of accidental hypothermia in avalanche buried victims. Also the rise of serum potassium levels is determined by previous factors: if cooling precedes critical levels of hypoxia, hypothermia will delay the rise of potassium levels; conversely, accidental hypothermia alone results in hypokalemia in the absence of trauma and asphyxiation (Buse et al., 2017). However, serum potassium can rise due to severe acidosis and hypoxia in avalanche victims with triple H syndrome: the result of long burial times, without sufficient air supply. Paal et al. (2013) observed a mixed respiratory and metabolic acidosis with increased serum potassium in hypoxemic animals without a sufficient resupply/removal of respiratory gases. Serum potassium was also associated with signs of cerebral hypoxia when investigated through brain computed tomography in complete avalanche burials with cardiac arrest (Cohen et al., 2016), but it should be used only for long burials (i.e., hypothermic victims) (Strapazzon et al., 2016).
On-Site Avalanche Treatment
Avalanche survival depends largely on the immediate extrication of completely buried avalanche victims. Despite that in Austria, similarly to most European countries, rescue is available from search and rescue, and helicopter medical emergency service (HEMS) on stand-by, survival rate of completely buried avalanche victims was ∼80% if the avalanche victim was extricated by bystanders versus <20% when extricated by HEMS crew (Mair et al., 2013). Longer on-scene arrival times (mean ∼45 minutes) than calculated rapid initial drop in survival probability could explain differences in survival probability. HEMS crews had to manage medical emergencies on-scene in 11% of rescue missions (Mair et al., 2013), and made on-site triage decisions about either termination of cardiopulmonary resuscitation (CPR) or transport of victims to the hub center (which is equipped with extracorporeal life support [ECLS] facility), or other spoke hospitals based on victim's clinical conditions. Medical management should be withheld on-site if it increases risk to the rescue team (Brugger et al., 2013; Truhlar et al., 2015; Van Tilburg et al., 2017).
Since the first algorithm publication for the on-site triage of avalanche victims with asystole was published in 1996 (Brugger et al., 1996), continuous update has been followed by ICAR Medcom (the latest published in 2013) (Brugger et al., 2013). These recommendations have been approved by ILCOR and were incorporated into the European Resuscitation Council (ERC) and American Heart Association recommendations in 2010 (Soar et al., 2010; Morrison et al., 2010). New algorithms and recommendations for the on-site management of avalanche victims have been recently released by ERC (Fig. 3) and WMS in 2015 and 2017, respectively (Truhlar et al., 2015; Van Tilburg et al., 2017). Unfortunately, compliance to the ICAR Medcom recommendations from 1996 to 2009 seems to be poor in a reference area for avalanche accidents such as Austria: CPR was often continued to hospital admission in avalanche victims with short burial and asphyxial cardiac arrest, but withheld or terminated at the scene in those with long burial and possible hypothermic cardiac arrest (Strapazzon et al., 2017b). Another study surveyed about the knowledge of ILCOR and ICAR Medcom recommendations in courses related to healthcare management in avalanche accidents in Italy (Strapazzon et al., 2018). Despite the fact that 75% of the participants were either advanced life support (ALS) or basic life support (BLS) providers or members of mountain rescue services (working in areas at risk of being involved in the management of avalanche victims—either on-site or in the hub/spoke hospitals), most of the respondents had never participated in specific lessons/courses. In an attempt to improve quality of on-site treatment of snow avalanche victims, ICAR Medcom created and implemented the AVReCh and promoted a standardized lecture (Fig. 4) (Kottmann et al., 2015, 2017).
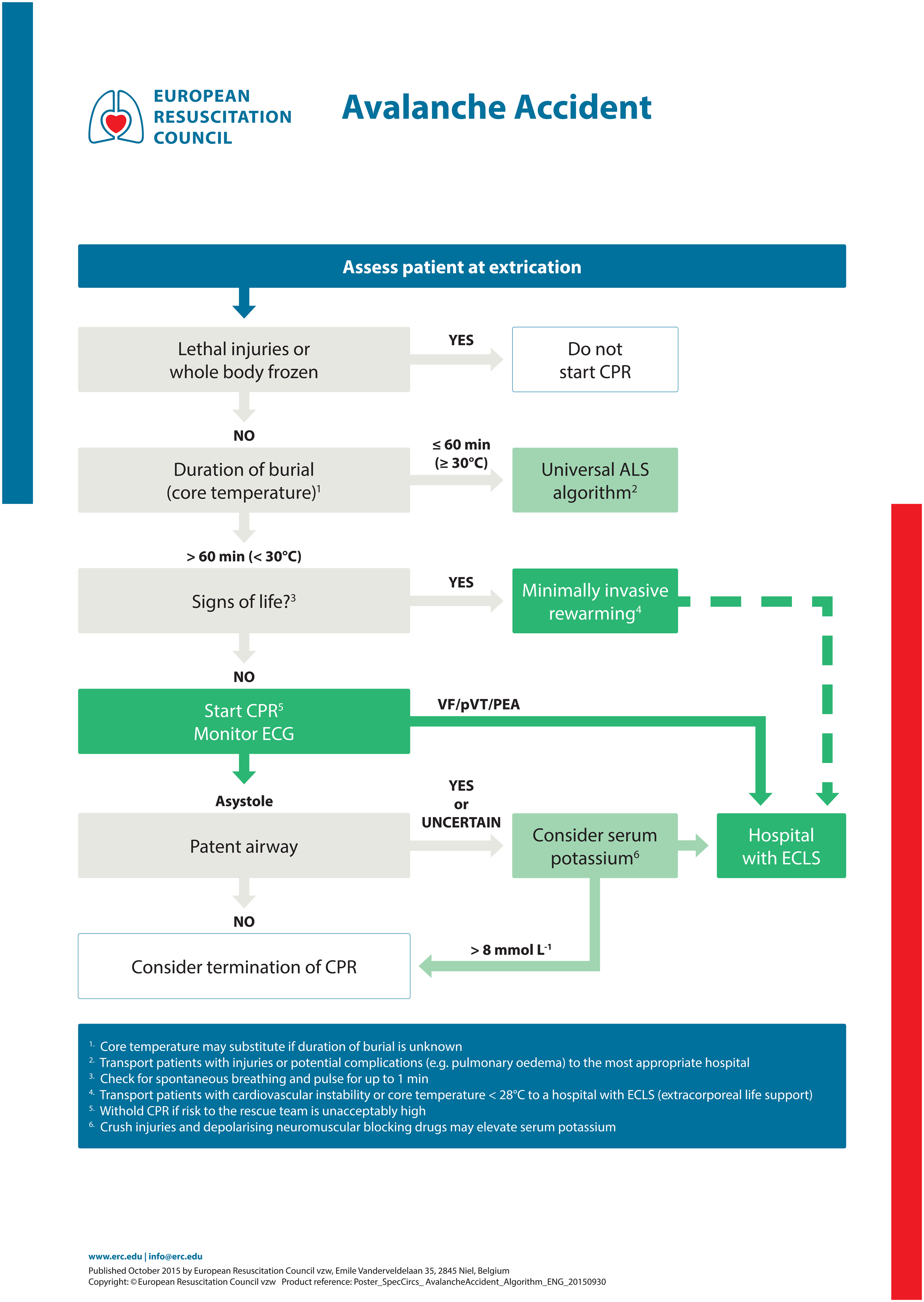
Avalanche accident algorithm. Management of completely buried victims. ALS, advanced life support; BLS, basic life support; CPR, cardiopulmonary resuscitation; ECLS, extracorporeal life support [modified from Truhlar et al. (2015) with permission from Elsevier].
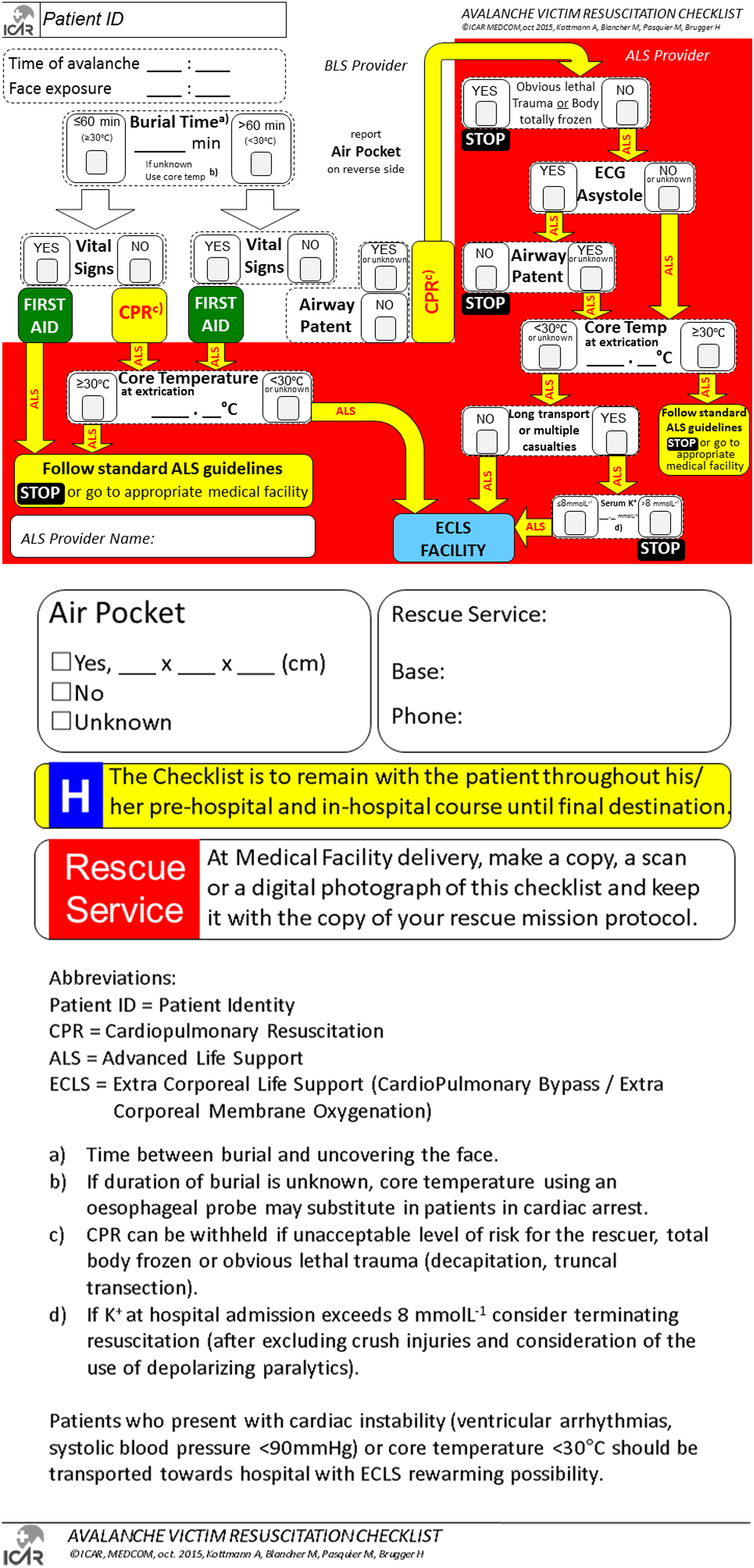
Avalanche victim resuscitation checklist. The white section is addressed to a BLS-trained first responder, the red section to an ALS-trained provider. ALS, advanced life support; patient ID, patient identity; CPR, cardiopulmonary resuscitation; BLS, basic life support; ECLS, extracorporeal life support (cardiopulmonary bypass/extracorporeal membrane oxygenation) [modified from Kottmann et al. (2017) with permission from Elsevier].
Trauma management
Avalanche victims can sustain potentially any type of injury. Head, cervical spine, chest, and extremities are body parts more frequently severely injured (Hohlrieder et al., 2007; McIntosh et al., 2007; Boyd et al., 2009). Current resuscitation recommendations emphasize to extricate the body gently and use spinal precautions in all avalanche victims (Truhlar et al., 2015; Van Tilburg et al., 2017). As the association of trauma with hypothermia can be deleterious, traumatic avalanche victims should receive a multilayer full-body insulation with heat packs on the trunk to prevent further cooling, immediately after extrication.
Cardiac arrest management
The survival rate of avalanche victims presenting with cardiac arrest ranges from 4% to 17% (Boué et al., 2014; Mair et al., 2014; Strapazzon et al., 2017b) The neurological outcome of avalanche victims will first depend on the severity of asphyxia, less on trauma and hypothermia.
BLS management
BLS management is indicated by companions/bystanders in all avalanche victims without vital signs (movements, breathing, or pulse), independently from the time of burial (or the core temperature) and the patency of the airway (Kottmann et al., 2015, 2017). The rate of chest compressions and ventilation should be the same as standard BLS (30:2) with minimal interruptions, both in normothermic and hypothermic avalanche victims in cardiac arrest (Brugger et al., 2013; Truhlar et al., 2015; Van Tilburg et al., 2017). Owing to the mainly asphyxial etiology of cardiac arrest, an important component for successful resuscitation is both chest compressions and ventilations (Truhlar et al., 2015). Completely buried avalanche victims were mainly found prone and were often buried with their heads in a downhill position in a United States survey of avalanche accidents (Kornhall et al., 2016), making it challenging to perform efficient resuscitation maneuvers. Nevertheless, an attempt to clear the airway should be made as soon as possible during extrication, even if chest compressions may be delayed due to body position.
ALS management
Determination of the duration of burial (or core temperature if the latter is unknown) is considered essential to determine ALS management. If the duration of burial is ≤60 minutes (or initial core temperature is ≥30°C) and cardiac arrest is confirmed, a normothermic cardiac arrest should be suspected: standard ALS recommendations should be followed (Fig. 3) (Truhlar et al., 2015; Van Tilburg et al., 2017). During CPR, oxygen should be given, insulation and heat packs should be applied to the trunk, core temperature should be measured, drugs and fluids should be given (only if intravenous or intraosseous access can be established within a few minutes), and ECG should be monitored (Truhlar et al., 2015). Resuscitation may be terminated if ALS is not successful after 20 minutes, in the absence of reversible causes (Truhlar et al., 2015). If the duration of burial is >60 minutes (or initial core temperature <30°C) and cardiac arrest is confirmed, a hypothermic cardiac arrest should be suspected: CPR should be started (Truhlar et al., 2015; Van Tilburg et al., 2017). If there is any electrical activity or a patent airway in an asystolic avalanche victim, CPR should be continued. If continuous CPR is not possible (due to insufficient logistical/human resources or lack of mechanical chest compression devices), the use of delayed or intermittent CPR has been newly proposed (Gordon et al., 2015). A hypothermic patient with a core temperature of 20°C–28°C, or an unknown core temperature, should receive at least 5 minutes of CPR alternating with periods of up to 5 minutes without CPR: pauses in CPR can be extended to up to 10 minutes if core temperature is <20°C.
The advantage of a secure airway and oxygenation outweighs the risk of triggering arrhythmias or ventricular fibrillation, and defibrillation beyond three attempts may be delayed until core temperature is ≥30°C. Drugs administration is controversial because the impact of adrenaline on survival and neurological outcome in a hypothermic cardiac arrest is contradictory (Truhlar et al., 2015), as suggested also in a recent experimental animal study wherein adrenaline was associated with an increase in global cerebral oxygen extraction despite an increase in cerebral perfusion pressure (Putzer et al., 2016).
Hypothermia management
Hypothermia should be suspected in a cold (i.e., trunk) and unconscious avalanche victim who has not died of asphyxia within 35 minutes, especially with a burial time >35–60 minutes (Boyd et al., 2010). ERC and WMS include recommendations for the treatment of accidental hypothermia (Truhlar et al., 2015; Van Tilburg et al., 2017). However, the level of consciousness, as well as cardiovascular and respiratory functions, demonstrated by an avalanche hypothermic victim is rarely determined, except by effect on core temperature. Traumatic injuries, as well as O2 and CO2 levels in any viable air pocket surrounding the victim, usually complicate the pathophysiology of accidental hypothermia in avalanche scenarios.
Triage and transport decisions
Transport of avalanche victims should consider the risk of critical illness (e.g., cardiac arrest and pulmonary edema) or injury of any other system (i.e., trauma care). Equally, futile attempts to transport avalanche victims should be avoided where contraindications are clear (i.e., asphyxial cardiac arrest with no return of spontaneous circulation (ROSC) after 20 minutes of standard ALS on-site). ERC recommendations implemented criteria for triage and transport decisions on-site by ALS providers (Fig. 3) (Truhlar et al., 2015). Specifically, based on epidemiological and experimental studies, duration of burial, initial core temperature, and serum potassium values have been revised and modified for avalanche victims in cardiac arrest to avoid futile primary and secondary transports (Truhlar et al., 2015; Van Tilburg et al., 2017). ERC recommendations state that avalanche victims are not likely to survive when (i) the duration of burial is ≤60 minutes (or if burial time is unknown, when the initial core temperature is ≥30°C), and the victim is in cardiac arrest without ROSC after 20 minutes of standard ALS management on-site; (ii) the duration of burial is >60 minutes (or if burial time is unknown, when the initial core temperature is <30°C) and the victim is in cardiac arrest with an obstructed airway on extrication (Truhlar et al., 2015; Van Tilburg et al., 2017); or (iii) the duration of burial is unknown but the victim is in cardiac arrest on extrication with an initial serum potassium >8 mmol/L. Consequently, if the duration of burial is >60 minutes (or initial core temperature is <30°C) and the avalanche victim is found in cardiac arrest with patent airways, the victim should be transported under continuous (ideally) CPR to a hub center with ECLS facility. If direct transport to an ECLS rewarming center is not possible in a timely manner, for example, by HEMS, a check of serum potassium level at the nearest hospital has been proposed: if potassium exceeds >8 mmol/L, termination of resuscitation should be considered (after excluding crush injuries and considering if depolarizing muscle relaxants were used) (Truhlar et al., 2015).
A new score (the Hypothermia Outcome Prediction after ECLS survival probability—HOPE score) is under external validation also for avalanche victims, as it seems superior to dichotomous triage based on serum potassium level in assessing which hypothermic patients in cardiac arrest would benefit from ECLS (Pasquier et al., 2018).
All avalanche victims with cardiovascular instability (i.e., ventricular arrhythmias, systolic blood pressure <90 mmHg) or core temperature <28°C should be transported to an ECLS rewarming center (Truhlar et al., 2015).
Multicausality accidents
Multiple victims can be found in avalanche accidents; more than four victims have been reportedly involved in >10% of avalanche HEMS operations in Austria (Mair et al., 2013). ICAR Medcom has recently released recommendations for on-site management of avalanche multicausality accidents (Blancher et al., 2018). Unless sufficient resources are available: (i) extrication is the first priority and medical care should focus on victims with vital signs with a burial time <35 minutes, (ii) no CPR should be started on avalanche victims in cardiac arrest with a burial time between 35 and 60 minutes, and (iii) CPR should only be initiated if the airway is patent if burial time is >60 minutes.
Avalanche victim resuscitation checklist
If an avalanche victim is found in cardiac arrest, it is crucial for those administering prehospital management and triage to know the duration of complete burial (or core temperature), presence of vital signs, status of the airway, and data about the air pocket that the victim was extricated from. ICAR Medcom created the AVReCh in an attempt to improve the quality of on-site treatment and triage decision management and care (Fig. 4) (Kottmann et al., 2015, 2017). AVReCh not only helps to guarantee strict adherence to on-site avalanche victim management (both for BLS and ALS providers) but also guarantees a reliable data transfer from the avalanche site to hospital for further diagnostic and therapeutic decisions.
Future Perspectives
Avalanche survival depends largely on the immediate extrication of completely buried avalanche victims by bystanders before HEMS crew arrival and, thereafter, on the use of established prognostic markers. It is crucial to know the duration of complete burial (or core temperature), presence of vital signs before cardiac arrest, and airway status; novel prognostic markers (e.g., presence of an air pocket) are emerging. Without a robust knowledge and training, the choices in the prehospital management can be wrongly affected by safety and other logistical challenges. Tools such as AVReCh, in combination with dedicated education programs, should be fostered to improve the knowledge and good clinical practice regarding principles of avalanche management. Dissemination should be adapted to different emergency medical systems and addressed to all providers of the avalanche rescue chain. Dedicated standard operating procedures for avalanche accidents should be implemented, and tailored to a local and nearby ECLS capacity.
Footnotes
Acknowledgment
We thank Rachel Turner for help in editing the article.
Author Disclosure Statement
No competing financial interests exist.