
Abstract
Abstract
Promising benefits on cardiometabolic risk factors have been reported with prolonged programs of cyclic hypoxia. The aim of this study was to examine whether cyclic hypoxia exposure while exercising through two protocols of high-intensity interval training in overweight/obese women is more effective to improve cardiometabolic risk markers than exercising in normoxia. Participants included 86 overweight/obese women, who started a 12-week program of 36 sessions, and were randomly divided into four groups: (1) interval training in hypoxia (IHT; FIO2 = 17.2%; n = 13), (2) interval training in normoxia (INT; n = 15), which included 3-minute high-intensity exercise (90% Wmax) followed by 3 minutes of active recovery (55%–65% Wmax), (3) repeated-sprint training in hypoxia (RSH; FIO2 = 17.2%; n = 15), and (4) repeated-sprint training in normoxia (RSN; n = 18), which included 30 seconds of all-out effort (130% Wmax) followed by 3 minutes of active recovery (55%–65% Wmax). Body composition, anthropometric, biochemical, and clinical parameters were assessed at baseline (A), after 18 training sessions (B), and during the 7 days after the last session (C). IHT and RSH showed a significant (p < 0.001 and p = 0.016, respectively) decrease in the waist circumference at both B and C assessments compared with A. Hypoxia groups presented a significant reduction in the percentage of trunk fat with a moderate effect size (IHT: d = 0.56; RSH: d = 0.93). In the normoxia groups, total cholesterol (CHOL) tended to decrease (INT: −4.21% and RSN: −5.18%), whereas it tended to increase in the hypoxia groups (IHT: +2.91% and RSH +4.07%). An interaction effect between conditions (through pooled data) on waist circumference (p = 0.01), percentage of trunk fat mass (p < 0.001), and CHOL (p = 0.019) was observed. Both training regimens under normobaric cyclic hypoxia were more effective at causing decreased abdominal fat in overweight/obese women than the same protocols in normoxia.
Introduction
O
In addition to improvements in fat mass, promising benefits on some cardiometabolic risk factors, such as blood glucose and BP, have been reported with the use of prolonged programs of moderate cyclic hypoxia (Bailey et al., 2000; Haufe et al., 2008; Urdampilleta et al., 2012; Debevec et al., 2014; Woolcott et al., 2014; Wee and Climstein, 2015). Actually, imprecise terminology exists in the field of intermittent hypoxia research (Xi and Serebrovskaya, 2012). With the aim to distinguish between different forms of intermittent hypoxia, experts (Xi and Serebrovskaya, 2012) suggested using “cyclic hypoxia” for short periods followed by periods of normoxia, to distinguish it from “intermittent hypoxia” associated with sleep-disordered breathing.
In this context, the key regulator of oxygen homeostasis is the stabilization of transcription of hypoxia-inducible factor 1 (HIF-1) (Halberg et al., 2009). Under hypoxic conditions, HIF-1α is stabilized and translocated to the nucleus where it heterodimerizes with HIF-1β forming HIF-1 complex and increasing the mRNA expression of a wide variety of genes (Dehne and Brune, 2009). Thus, during intermittent hypoxia, the many cycles of hypoxia and reoxygenation are stimulus for HIF-1 activation, but during cyclic hypoxia, HIFs accumulate strictly during the periods of hypoxia (Xi and Serebrovskaya, 2012). This aspect is the essential reason that explains the beneficial effects of cyclic hypoxia.
In this sense, HIF-1α would not be activated to the same extent by passive hypoxic exposure (during rest) or by active hypoxic exposure (during exercise) (Millet et al., 2016). There is scientific evidence suggesting that lower degradation of HIF-1α results when hypoxia and physical activity are combined (Urdampilleta et al., 2012). It seems likely that the main underlying mechanism is the larger hypoxemia resulting from the combination of muscle deoxygenation (exercise) and systemic desaturation (hypoxia) (Millet et al., 2016). Although hypoxia may contribute to changes in BP (Auer et al., 2004; Shave et al., 2004; Foster et al., 2005; Fukuda-Matsuda et al., 2007; Wiesner et al., 2010), glucose uptake (Haufe et al., 2008; Wiesner et al., 2010), and lipid profile (Bailey et al., 2001; Greie et al., 2006; Netzer et al., 2008; Minvaleev, 2011), the results are inconclusive.
Despite exercise programs typically involving moderate-intensity, continuous exercise (Haufe et al., 2008; Netzer et al., 2008; Wiesner et al., 2010; Kong et al., 2014; Gatterer et al., 2015), it needs to be pointed out that the improvements in response to moderate-intensity exercise may be influenced by several factors, including the length of training period (Morishima et al., 2015). It seems that more than 4 weeks of intervention with active hypoxia are required for positive effects (Hobbins et al., 2017). However, long periods may impede regular exercise, so a shorter training regimen could be needed for more effective outcomes. In this way, cyclic hypoxia and high-intensity interval training (HIIT) may have a synergistic effect because of both stimuli regulating crucial pathways in glucose and lipid metabolism (Vogt et al., 2001).
HIIT refers to repeated sessions of relatively brief intermittent exercise, often performed with an “all-out” effort or at an intensity ≥85% VO2peak (Norton et al., 2010). To the best of our knowledge, only one recent study (Kong et al., 2017) investigated the effect of short-term HIIT with normobaric hypoxia exposure on cardiometabolic parameters in young women. They showed that 5 weeks of HIIT with moderate hypoxia improved cardiorespiratory fitness, but it had no additive effect to enhance body composition or lipid profile.
Obviously, more research is needed to examine the impact of cyclic hypoxia exposure while exercising through HIIT therapy on physiological responses, the mechanisms underlying these benefits, and the optimal combination of exercise (intensity, type of activity, etc.) and hypoxia (altitude level, dose, type, etc.) Interval training alone could not represent a sufficient intense training to achieve beneficial adaptations (Millet and Girard, 2017). Previous authors showed that the repeated-sprint training that is based on all-out sprints with active recovery (Girard et al., 2017) results in higher exercise intensity than usual interval training. Higher intensity leads to a lower rate of oxygen delivery to the working muscles, stimulating the glycolytic flux, and thus induces beneficial adaptations (Millet and Girard, 2017).
Thus, the aims of this study were (1) to examine whether cyclic hypoxia exposure while exercising through two protocols of HIIT in overweight/obese women is more effective to improve cardiometabolic risk markers compared with exercising in normoxia and (2) to examine whether two different protocols of HIIT under cyclic hypoxia lead to different effects on cardiometabolic risk markers. It is hypothesized that the greater physiological stress caused by the combination of HIIT in hypoxia conditions, especially repeated sprint, would be more effective to improve risk markers than exercising in normoxia.
Methods
Participants
Participants were recruited through advertising in the community, in the researchers' host institution, and by personal contact. Inclusion criteria assessed during a screening visit were as follows: body mass index (BMI) >25 kg/m2 (overweight or obese for adults according to World Health Organization [WHO]) or percentage fat mass (%fat) >29.9% [elevated risk of cardiovascular disease (ACSM, 2014)], absence of other associated diseases, premenopausal, sedentary [<2 bouts of exercise lasting a minimum of 30 minutes per bout per week (WHO, 2010)], and have not been above 1500 m during the past 3 months. The exclusion criteria were diseases not compatible with study exercise: myocardial infarction or stroke within 6 months before the start of the study, unstable angina pectoris, malignant hypertension, or chronic kidney disease.
In total, 112 female volunteers were informed about the study procedures and, after verifying inclusion and exclusion criteria through an examination, they were asked to sign a declaration that they voluntarily consented to participate in this research. The eligible volunteers (n = 86; body mass: 78.12 ± 14.70 kg; BMI: 28.98 ± 5.19; %fat: 38.63 ± 5.78) started interval training treatment under normoxic or hypoxic conditions. Owing to health problems (not related to the study protocol), occupational factors, and other personal problems, 26 participants dropped out during the intervention period (Fig. 1).
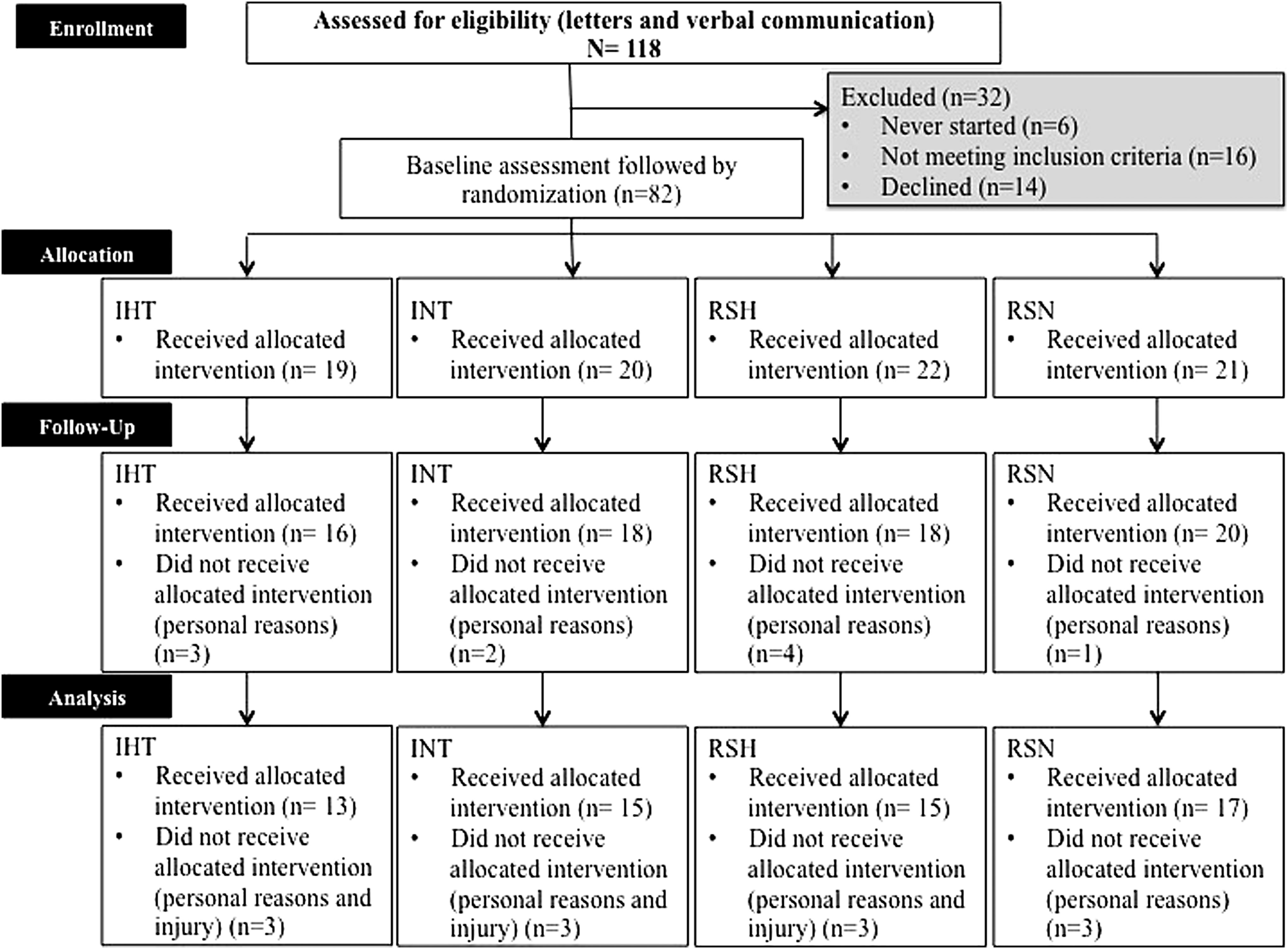
Flow of participants through each stage of the trial. IHT, interval-training hypoxia group; INT, interval-training normoxia group; RSH, repeated-sprint hypoxia group; RSN, repeated-sprint training normoxia group.
The study was performed in line with the ethical standards of the Declaration of Helsinki. The Bioethical and Biosecurity Commission of the University of Extremadura approved the study protocol (Number Register: 13/2016).
Procedures
The study was designed as a randomized double-blind control study. There were separate intervention and assessment teams. The volunteers were randomly divided into four groups: (1) interval training in hypoxia (IHT; n = 13), in which interval training was performed under normobaric hypoxic conditions; (2) interval training in normoxia (INT; n = 15), in which interval training was performed under normoxic conditions; (3) repeated-sprint training in hypoxia (RSH; n = 15), in which sprint interval training was performed under normobaric hypoxic conditions; and (4) repeated-sprint training in normoxia (RSN; n = 18), in which sprint interval training was performed under normoxic conditions. For 12 weeks, the volunteers completed an intervention supervised by an experienced member of the research group. Approximately 2 weeks before baseline measurements, participants reported to the laboratory for familiarization with experimental trials and fitness testing. A general questionnaire was completed to collect medical and personal data before entering the study. To assess maximal workload (Wmax), all participants performed a maximal ramp incremental test to exhaustion (Lanzi et al., 2014, 2015) on the same cycle ergometer (Ergoselect series 100/200; Ergoline GmbH, Bitz, Germany) as training, before the training protocol (phase 1) and after the middle of the program (phase 2). At the middle of program, the incremental tests were carried out again to adapt power values to current level and thus ensure that the effort was adequate.
All participants were assessed at three time points by a group of researchers who were blinded to the treatment assigned. Outcomes were evaluated at baseline (A), after 18 training sessions (B), and during the 7 days after the last session (C). All time points for evaluations consisted of the same measurements (Fig. 2).
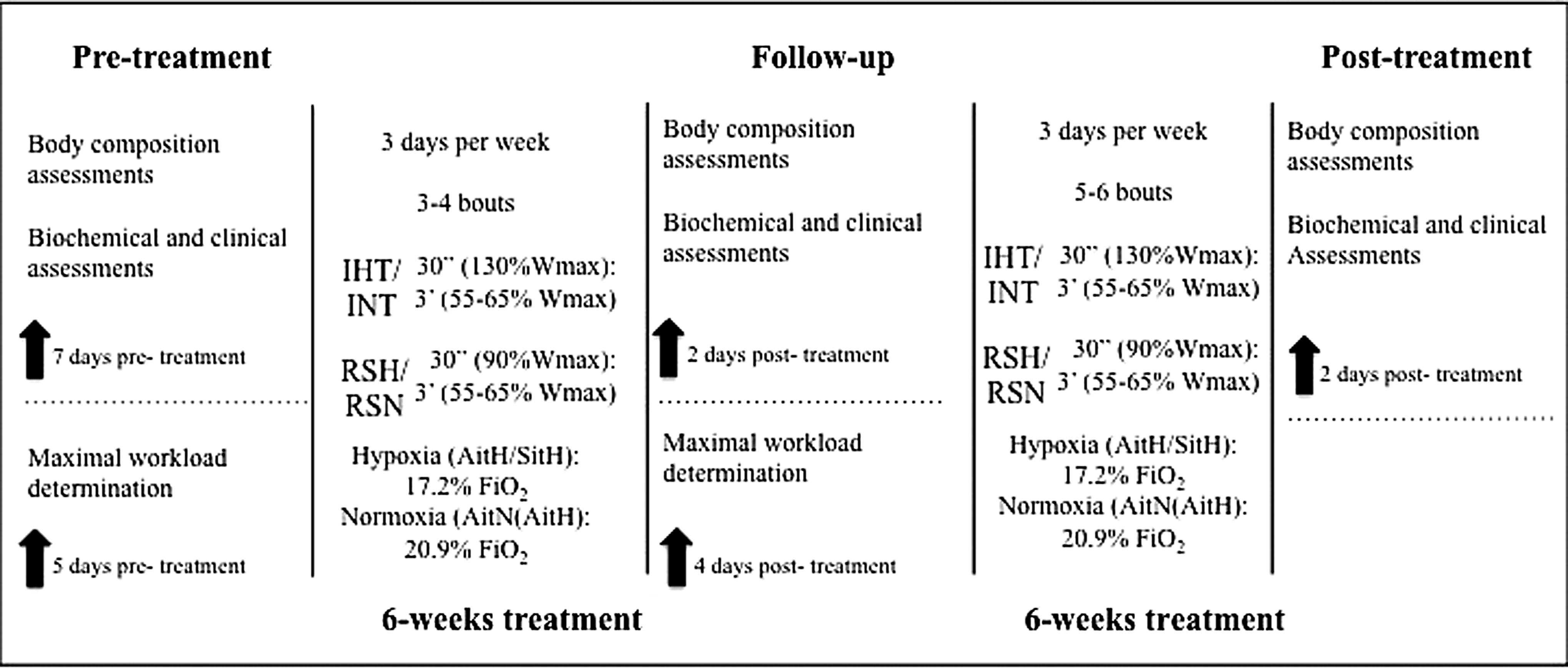
The timeline of pre-, follow-up, and posttreatment measurements, as well as the 12-week intervention. Wmax, maximal workload; FiO2, inspired fraction of oxygen.
Training program
All participants started the training protocol after the baseline assessments. During 12 weeks, the participants completed 36 sessions within 3 days per week. Sessions were scheduled with at least 1 day of rest between for optimal recovery (Mondays, Wednesdays, and Fridays) and participants were requested to train at the same time throughout the 36 sessions. At each session, an exercise physiologist recorded adherence, exercise workloads, and physiological responses in a daily training log. Oxygen saturation (SpO2) was controlled regularly through pulse oximeter (Konica Minolta, Japan). Heart rate (HR) was monitored during each session with an HR monitor (Team System, Polar, Finland). Participants rated their perceived exertion (0–10 scale) at the end of each training session (Borg, 1982).
Interval training protocol
Participants performed two different HIIT protocols 3 days per week on a cycle ergometer (Ergoselect series 100/200; Ergoline GmbH), the recommended exercise in this population to reduce the level of impact on joints (Rampinini et al., 2016; Vannini et al., 2016). The two exercise protocols were designed to maintain progressive overall work over the 12 weeks of study. During the 1st and 2nd weeks, subjects finished three high-intensity intervals, four intervals between the 3rd and 5th weeks, five intervals between the 6th and 8th weeks, and six intervals from the 9th to the 12th week.
Participants completed a 10-minute warm-up and 3-minute cooldown at 25% Wmax (Heydari et al., 2012; Keating et al., 2014; Lanzi et al., 2015). In the exercise protocol, the IHT and INT groups performed 3 minutes of high-intensity exercise (90% Wmax) followed by 3 minutes of active recovery (55%–65% Wmax). The RSH and RSN groups underwent 30 seconds of all-out (130% Wmax) followed by 3 minutes of active recovery (55%–65% Wmax) (Wood et al., 2015). Exercise time per session was 24 minutes during the 1st and 2nd weeks, 30 minutes between the 3rd and 5th weeks, 36 minutes between the 6th and 8th weeks, and 42 minutes during the last 9th through 12th weeks in the interval training (IT) groups. In the repeated sprint (RS) groups, the exercise time per session was 16 minutes and 30 seconds during the 1st and 2nd weeks, 20 minutes between the 3rd and 5th weeks, 23 minutes and 30 seconds between the 6th and 8th weeks, and 27 minutes during the 9th through 12th weeks. The exercise prescriptions are summarized in Figure 2.
Hypoxic stimulus
All training sessions were performed in two normobaric hypoxia chambers (CAT 310, Louisville, CO) placed in the laboratory (24°C and 40% relative humidity). The IHT and RSH groups exercised at an inspired fraction of oxygen (FIO2) of 17.2% ± 0.3% corresponding to ∼2500 m, whereas the INT and RSN groups exercised at FIO2 of 20.9% corresponding to sea level in the laboratory (459 m). Insufflating nitrogen that was produced from chamber air through a molecular sieve could have reduced the oxygen content within the chamber. FIO2 was controlled regularly with an electronic device (HANDI+; Maxtec, Salt Lake City, UT). To ensure the blinding process, subjects of all groups performed the training inside the hypoxic chamber with the ventilation system running with the window closed. The efficacy of the blinding process was assessed by interviewing the participants immediately after the last training session.
Outcome measures
Assessments took place in one session at all three time points. Participants attended the research laboratory after a minimum of 8 hours overnight fasting for measurements.
Medical history and lifestyle questionnaires
Subjects in all groups were instructed to maintain their usual eating habits and physical activities during the study period. On their first and last visit to the laboratory, subjects were provided the International Physical Activity Questionnaire (IPAQ) (Craig et al., 2003) and a 7-day diet inventory that was analyzed using the diet software Nutriber (Nutriber v1.1.1.r5; Funiber, Barcelona, Spain).
Maximal workload determination
A maximal incremental test on a cycle ergometer (Ergoselect series 100/200; Ergoline GmbH) with gas analyzer (Metalyzer 3b; CORTEX Biophysik GmbH) was performed. After a 5-minute warm-up at 50 W and 1-minute rest, participants were allowed to expire before initiating formal data collection to allow acclimation to the apparatus, and then the test was initiated. Subjects started cycling at 30 W and the work rate was increased 15 W every 3 minutes until exhaustion. HR was recorded continuously during the test using a cardio belt (Polar H7 HR; Polar, Kempele, Finland) integrated with the gas analyzer software (MetaSoft Studio; CORTEX systems, Leipzig, Germany). The measurement finished when at least three of the following four criteria were met (Wood et al., 2010): (1) plateauing of VO2 (defined as an increase of no more than 2 mL/(kg·min) with an increase in workload) during the latter stages of the exercise test, (2) HR >90% of the age predicted maximum (220 − age), (3) respiratory exchange ratio >1.1, and (4) inability to maintain the minimal required pedaling frequency (i.e., 60 rpm) despite maximum effort and verbal encouragement. Thus, the peak power was defined as maximal power achieved during the last 3-minute step completed during the incremental test.
Anthropometric measures and body composition
Anthropometric data comprised weight and height measures to the nearest 0.1 kg and 0.5 cm, respectively. Hip and waist circumferences were measured to the nearest 0.5 cm. Measurements were completed according to the manufacturer's guidelines. Waist–hip index (WHI) was calculated as the waist circumference divided by hip circumference.
Body composition was determined by bioelectrical impedance analysis (BIA) using a standardized body composition analyzer (Tanita BC 418 MA; Tanita Corp., Tokyo, Japan) and included estimation of body fat percentage (%fat), trunk fat percentage, and BMI (coefficient variation = 1.1% for body fat). Subjects maintained a standing position, with feet side-by-side on the scale and were barefoot. They wore sport clothes without metal objects. BIA scales are practical, safe, and have acceptable accuracy for estimating %fat when compared with dual-energy x-ray absorptiometry, the gold standard for body composition assessment (Ramirez-Velez et al., 2018).
Biochemical and clinical measurements
Blood samples were taken from the antecubital vein by one experienced nurse in the research laboratory and included the determination of TG, total cholesterol (CHOL), and glucose concentration (G). One hundred microliters of whole blood was collected in heparinized microwells and centrifuged for 5 minutes at 6000 rpm (MC6 centrifugue; Sarstedt, Nümbrecht, Germany). Centrifugation of samples was performed with an automatic dry-chemistry analyzer system (Spotchem EZ SP-4430; Arkray, Inc., Kyoto, Japan). The calibration was checked daily according to the manufacturer's recommendation through indicated reagent cards. The reproducibility of each parameter was evaluated by measuring the level 15 times from a single blood sample and determining the coefficient of variation [CV (G) = 2.5%; CV (CHOL) = 3.4%; CV (TG) = 1.9%]. Systemic BP determinations and resting HR (rest) were measured with a mercury sphygmomanometer, following the recommendations of the American Heart Association (Pickering et al., 2005).
Statistical analysis
Statistical analyses were performed using the statistical package SPSS v.20 for MAC (IBM, Armonk, NY). Data are presented as mean ± standard deviation (SD). Standard statistical methods were used for the calculation of mean and SD. Kolmogorov–Smirnov tests were conducted to show the distribution of the studied variables and Levene's test was used for homogeneity of variance. All data were normally distributed and baseline characteristics were compared using one-way analysis of variance (ANOVA). Mixed factorial ANOVA was performed taking into account the interaction between conditions (hypoxia and normoxia), time, and training (IT and RS). If a global difference over time appeared, a Bonferroni post hoc analysis was used to identify where changes occurred. The effect size (Cohen, 1992) was calculated for all variables between baseline and after 12 weeks of intervention. The magnitude of the difference was considered small (0.41), moderate (1.15), or large (2.70) (Ferguson, 2009). The p < 0.05 criterion was used for establishing statistical significance.
Results
Demographic and physiological baseline characteristics for all treatment groups are provided in Table 1. No initial difference in these parameters was found. Because of the neutral training place, subjects could not discriminate whether they were in hypoxia or normoxia. Blinding was successful as >60% of subjects did not guess their conditions correctly. There were no serious health problems reported by the volunteers.
p-Values of analysis of variance to compare differences between groups at baseline.
Differences with respect to SitH (post hoc t-test with Bonferroni correction).Values in bold are significant.
Differences with respect to AitH (post hoc t-test with Bonferroni correction).
BMI, body mass index; VO2max, maximal oxygen uptake; IHT, interval-training hypoxia group; INT, interval-training normoxia group; RSH, repeated-sprint hypoxia group; RSN, repeated-sprint training normoxia group; SD, standard deviation.
Control training variables, energy intake, and estimated physical activity level during the week before and after the intervention are presented in Table 2. Oxygen saturation during the training session was lower (p < 0.01) and RPE was higher (p > 0.05) for the hypoxia groups. HR and average power during training sessions were not significantly different between groups. No significant difference was noted before and after the intervention for habitual energy intake (p > 0.05); similar results were also found for estimated physical activity level (p > 0.05).
p-Values of analysis of variance to compare differences between groups at baseline.
Differences with respect to AitH (post hoc t-test with Bonferroni correction).
Differences with respect to AitN (post hoc t-test with Bonferroni correction).
Differences with respect to SitH (post hoc t-test with Bonferroni correction). Values in bold are significant.
Differences with respect to SitN (post hoc t-test with Bonferroni correction).
Pave, average power; HRave, average heart rate during total training session; HR max, maximal heart rate during main part training session; SO2, oxygen saturation during training session; RPE, rated perceived exertion; EE, energy expenditure.
In Figure 3 is given the average power output developed during the training sessions in phase 1 (1st and 18th training sessions) and phase 2 (19th and 36th training sessions). IHT, RSH, and RSN groups increased significantly the average power output in phase 2 compared with phase 1.

Average power output during training sessions in phase 1 (1st and 18th training sessions) and in phase 2 (19th and 36th training sessions). *Differences with respect to initial power output.
Anthropometric and body composition measurements
In Table 3 the variables of anthropometric and body composition at pretreatment (A), follow-up (B), and posttreatment (C) are given. Hypoxia groups showed a significant decrease in waist circumference and percentage of trunk fat mass. IHT and RSH showed a significant (p < 0.001 and p = 0.016, respectively) decrease in waist circumference at both times of evaluation compared with baseline. All training groups presented a reduction in the percentage of trunk fat mass, the reduction being significant only in the hypoxia groups (p < 0.001) with a moderate effect size (IHT: d = 0.56; RSH: d = 0.93), especially at posttreatment where the IHT group decreased 10.24% and the RSH group decreased 8.33%. The IHT group achieved a statistically significant (p = 0.003) decrease in WHI at follow-up (Δ −3.80%) and in the posttreatment with a moderate effect size (Δ −5.78%; d = 0.67).
Differences with respect to baseline (post hoc t-test with Bonferroni correction).
WHI, waist–hip index.
The analysis revealed an interaction effect between conditions (hypoxia or normoxia) on waist circumference (p = 0.01) and percentage of trunk fat mass (p < 0.001). No interaction effect between either training (IT or RS) was observed on any anthropometric or body composition outcomes.
Biochemical and clinical measurements
Table 4 provides the effect of the training protocols on glucose, CHOL, and TG measurements in venous blood samples. CHOL decreased significantly in the follow-up compared with baseline (p = 0.033) in the RSN. Although no significant changes were observed, in the normoxia groups, this parameter tended to decrease after the training program (INT: −4.21% and RSN: −5.18%) and tended to increase in the hypoxia groups (IHT: +2.91% and RSH +4.07%), with a moderate effect size (d = 0.58) in the IHT. All training groups showed a significant reduction in TG levels in the posttreatment measures with a moderate effect size (INT: 0.57; RSN: 0.46; IHT: 1.06; RSH: 0.71), especially in the hypoxia groups where the IHT group decreased 27.49% and the RSH group decreased 24.48%. Plasma glucose levels did not show significant differences in the within-subjects analysis, but tended to decrease in all groups after intervention compared with baseline with a moderate effect size (d > 0.41).
Differences with respect to baseline (post hoc t-test with Bonferroni correction).
An interaction effect between conditions (hypoxia or normoxia) on CHOL (p = 0.019) was observed. No interaction effect was observed between training protocol (IT or RS) on any blood parameter.
In Table 5 the effect of the training protocols on BP (systolic, diastolic, and mean) and resting HR are given. There were no significant differences in any parameters in the within-subjects analysis. No interaction effect was observed either between conditions (hypoxia or normoxia) or training (IT or RS) on any cardiovascular outcomes.
Discussion
This study examined the effects of cyclic hypoxia exposure while exercising through two protocols of HIIT compared with exercising in normoxia on cardiometabolic risk markers. The main findings confirm, at least partly, the hypothesis that both 12-week programs of high-intensity training in hypoxia resulted in larger improvements regarding abdominal fat than exercising in normoxia. Besides, both HIITs under cyclic hypoxia altered TG and CHOL differently compared with normoxia groups. As lack of time is often a key barrier to regular exercise participation (Smith-Ryan et al., 2016), sprint interval training under cyclic hypoxia may provide a time-metabolic effective alternative. There were no significant changes in clinical parameters.
The pattern of body fat distribution is recognized as an important predictor of the health risks of obesity (Bankoff and Zago, 2014). The presence of excess fat in the abdomen that reflects the amount of visceral fat mass (Wajchenberg, 2000) has been shown to be associated with an increased risk of all causes of mortality (Zhang et al., 2008). In this context, different researches have shown that waist circumference correlates with the amount of fat in the abdomen, and thus it has been shown to be strongly associated with the amount of visceral fat (Wajchenberg, 2000). In addition, abdominal fat mass was significantly associated with chronic pain, suggesting that this parameter per se may play a role in pain (Ray et al., 2011), especially among women (Yoo et al., 2014). In this way, reducing abdominal fat mass could be indisputably essential to decrease musculoskeletal pain in obese patients and support meeting the current physical activity guidelines (Girard et al., 2017). Beneficial effects of hypoxic exposure with low-intensity exercise on body composition in overweight and obese people have already been reported (Netzer et al., 2008; Wiesner et al., 2010; Kong et al., 2014). A marked increase in lipid oxidation during recovery time of cyclic hypoxia seems be the main underlying mechanism (Kelly and Basset, 2017). Thus, it is reasonable to postulate that the additive effects of combined cyclic hypoxia with HIIT on greater reduction in body fat could be attributed to higher postexercise lipid oxidation (Kendzerska et al., 2016; Camacho-Cardenosa et al., 2018). However, findings regarding body fat and hypoxic exposure combined with HIIT are limited. In this study, greater reductions in both percentage of trunk fat mass and waist circumference were observed after both hypoxic HIIT regimes compared with the normoxic equivalents. These improvements were observed even after completing half of the training program (T2). The reduced time required to achieve health improvements may be one important aspect for many obese adults, showing potential for higher rates of adherence (Heinrich et al., 2014). In fact, the positive feedback to complete a task increases enjoyment and, in this way, adherence to exercise (Hu et al., 2007). To our knowledge, this is the first study analyzing regional body fat with HIIT under hypoxia exposure in overweight/obese individuals. In a study on overweight women (Kong et al., 2017), 5 weeks of HIIT under hypoxia did not show an additive effect on whole body and regional body composition. In this way, the different impact on body fat might be derived from participants' initial adiposity levels (Forbes, 2000). Participants with a higher adiposity level seem to have more fat loss after an intervention compared with those possessing lower levels (Hansen et al., 2001). In this study, the initial fat mass located in the trunk (≈37%) of the overweight/obese women seemed to be higher than that (≈19%) reported in the previous study.
In general, the response of biochemical and clinical parameters to exercise and hypoxia is varied, and different factors may play a role in the response, such as initial concentration or the protocol employed. Similar to previous studies (Netzer et al., 2008; Wiesner et al., 2010; Gatterer et al., 2015; Gonzalez-Muniesa et al., 2015; Morishima et al., 2015; Kong et al., 2017), changes in TG levels do not seem to be significantly affected by active hypoxia in overweight or obese individuals compared with normoxia. Interestingly, an interaction between conditions was observed regarding CHOL. A previous study (Leggate et al., 2010) demonstrated that exercise protocols that result in greater inflammatory responses could generate greater improvements in lipid profile by increasing the HDL concentration. On the contrary, there is evidence of a positive correlation between plasma TG concentration and LDL concentration (Kondo et al., 2001). In this way, it may be reasonable to presuppose that the observed increases in CHOL in both hypoxia groups, and the decrease in triglyceride concentrations, might be because of a positive effect of hypoxia on HDL cholesterol. Unfortunately, in this study, HDL and LDL levels were not assessed. Futures studies that corroborate this hypothesis are necessary. Previous studies regarding glucose metabolism are rare and inconclusive (Wiesner et al., 2010; Morishima et al., 2014). In our study, levels of plasma glucose decreased in all groups with a moderate effect size, although none of the effects reached statistical significance. BP parameters did not change significantly in any training groups. Despite abundant evidence in hypertensive patients that suggests adding hypoxic stimuli to exercise induces greater reductions in BP compared with normoxic training (Millet et al., 2016), in healthy individuals these results are contradictory (Wiesner et al., 2010; Kong et al., 2014; Gatterer et al., 2015; Gonzalez-Muniesa et al., 2015).
This study has both strengths and limitations. To our knowledge, this is the first study that investigates the effect of short-term and long-term exercise in overweight/obese patients through a four-group randomized controlled study combining cyclic hypoxia with two different HIIT protocols. Regarding limitations, although participants were informed not to change their normal physical activity and eating habits and nonsignificant differences were found between records, some favorable behavioral alterations might have occurred outside the study procedure. However, maintaining the subjects on their normal food habits seems to be the most logical choice, and their effect should be low and not influence current conclusions. On the contrary, the findings of this study regarding glucose and lipid metabolism are limited by the biochemical parameters assessed (Ford et al., 2008). Although previous research analyzed similar outcomes, further studies are warranted to corroborate our assumptions with direct markers of insulin sensitivity or lipid profile (HDL and LDL cholesterol). Despite cycling other types of exercise are justified (Rampinini et al., 2016; Vannini et al., 2016), for example, speed walking in hypoxia was demonstrated to be an effective therapy to optimize weight management (Fernandez Menendez et al., 2018). Regular physical exercise such as walking is generally recommended for the obese population (Girard et al., 2017), especially because this is the principal component of daily life involving energy expenditure (Fernandez Menendez et al., 2018). Finally, as improvements achieved can decrease because of unexpected causes such as illness or vacations (Toraman, 2005), it seems interesting to know whether the possible benefits are maintained once training ceases (Lobo et al., 2010), not only on cardiovascular risk factors but also on fitness parameters.
Conclusion
In conclusion, both interval training protocols under normobaric cyclic hypoxia for 12 weeks were more effective in causing a decrease in abdominal fat in overweight/obese women and, possibly, beneficial changes on TG at the middle of the program. Thus, sprint interval training under normobaric cyclic hypoxia could be a time-metabolic alternative for those subjects with less time available, by causing beneficial effects on metabolism with time sparing intervention.
Footnotes
Acknowledgments
This research was funded by the Consejería de Educación y Empleo, Junta de Extremadura (GR15020) and the Ministerio de Educación, Cultura y Deporte (FPU15/00450).
Author Disclosure Statement
No competing financial interests exist.